Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
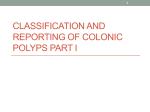
7/24/2012 Colon Polyps and Polyposis Syndromes Douglas K Rex Two histologies account for 99% of colorectal polyps • Adenomas and adenomas with invasive carcinoma • Serrated polyps – Hyperplastic polyps – Sessile serrated adenomas (SSAs) – Traditional serrated adenomas (TSAs) 1 7/24/2012 Polyp classifications • Shape • Size • Histology Shape – Paris Classification 2 7/24/2012 Shape classification • Type 1 – the “polyps” – Pedunculated (1p) – about 5% of all polyps – Sessile (1s)‐ about 50% of all polyps • Type 2 – 40‐50% of all precancerous lesions – also called “flat and depressed lesions” or “Non‐ polypoid colorectal neoplasia” – Flat • IIa ‐very common and not scary • IIb‐ rare and not scary – Depressed (IIc, IIa+IIc,IIc+IIa)‐ very uncommon and very bad histology Features indicating adenomas – red headed pedunculated polyps 3 7/24/2012 Sessile Polyps – Shape 1s Flat Lesions – Paris Classification IIa IIb 4 7/24/2012 IIa (flat) lesions in white light Depressed 5 7/24/2012 Polyp shape • Lateral spreading tumor (essentially a large IIa lesion: often called “carpet lesion” in U.S.) – Granular (most common, least worrisome) – Non‐granular( less common, worse histology) Lateral Spreading Tumor 6 7/24/2012 • Any given endoscopic technique is more likely to miss flat and depressed lesions than polypoid lesions Polyp size • Usual groupings – Diminutive (1‐5mm) – about 80% of all polyps – Small (6‐9) – about 10% of all polyps – Large (≥ 10 mm) – about 10% of all polyps 7 7/24/2012 Polyp size vs histology Size %adenoma % serrated 1‐5 mm 50% 50% 6‐9 mm 60% 40% ≥ 10 mm 85% 15% Adenomas • All adenomas are dysplastic • Atypia is an improper term in the description of adenomas • Dysplasia should be classified as low grade or high grade – Mild,moderate,severe: too much interoberserver variation • Most adenomas have LGD • Pathologists may use different definitions of HGD – Morphologic criteria: lower rates of HGD – Cytologic criteria: higher rates of HGD 8 7/24/2012 Discouraged (outdated) terms • Carcinoma‐in‐situ: severe dysplastic changes confined to the epithelium • Intramucosal carcinoma: dysplasia is present in the lamina propria but not the mucosa • Both “carcinoma‐in‐situ” and “intramucosal carcinoma” should be designated HGD – Both are benign – patients with completely resected polyps are cured 100% of the time 9 7/24/2012 Definition of cancer in the colon • Invasion of dysplastic elements into the submucosa – Why this definition? Because there are no lymphatics in the mucosa: lesions confined to the mucosa have no chance of metastasis 10 7/24/2012 Villous vs Tubular • Villous: greater risk of HGD and invasive cancer 11 7/24/2012 Tubular vs Villous • Tubular: > 75% tubular • Villous: > 75% villous • Tubulovillous: < 75% of both – Polyps with either villous or tubulovillous histology are often said to have “villous elements” • Marked variation in pathologic interpretation: up to 6 fold differences between pathologists 12 7/24/2012 Advanced adenoma • Concept developed as a surrogate marker of risk in post‐polypectomy studies • Most common definition is an adenoma with any of the following: – Size ≥ 10 mm – HGD – Villous elements Impact of variable interpretation of HGD • Randomized controlled trials of diffuse dye‐ spraying (chromoendoscopy) • Sheffield, U.K. (Hurlstone‐260 pts) and St Mark’s London,U.K. (Brooker – 259 pts) 13 7/24/2012 Impact of variable interpretation of HGD • Adenoma cohort RCTs colonoscoped at 1 and 3‐4 years • National Polyp Study and rofecoxib trial When is endoscopic resection of a malignant polyp adequate? • Rules developed for pedunculated malignant polyps: – Clear margin – Well or moderately differentiated – No lymphatic or vascular invasion – Endoscopist confident of complete resection 14 7/24/2012 Serrated polyps • Hyperplastic polyps in distal colon – Mostly diminutive and mostly clinically insignificant • In proximal colon these lesions share molecular features with a group of cancers in the proximal colon – CpG Island Methylator Phenotype (CIMP) – Sometimes with MSI (hypermethylation of MLH1) – BRAF mutations Typical proximal colon serrated polyps 15 7/24/2012 Serrated Polyps • TSAs are more obvious endoscopically • SSAs can have cytologic dysplasia and can be endoscopically very subtle • Marked interobserver variation between pathologists in interpretation of SSA vs hyperplastic • Risk for individual patients should consider number, size, location and histology of serrated polyps Sessile serrated adenomas 16 7/24/2012 SSAs Follow up of proximal colon serrated polyps • New recs coming for surveillance • Problems: – Miss rate unknown – Interobserver variation in pathologic interpretation – Significance of histology uncertain: sessile serrated polyp (adenoma) > hyperplastic polyp 17 7/24/2012 Serrated polyposis syndrome • WHO definition (not yet validated) – ≥ 5 serrated polyps proximal to sigmoid of which ≥ 2 are > 1 cm in size – 1 serrated polyp proximal to the sigmoid in patient with FDR who has SPS – > 20 serrated polyps “throughout the colon” • Many patients with SPS do not have a family history of SPS or CRC • Associated with smoking • Genetic basis not yet established Follow up of proximal colon serrated polyps • Aggressively search for and resect • Consider number, size, and histology of lesions in considering follow up intervals (clinical judgment) 18 7/24/2012 Other histologies – inflammatory • Often has exudate on surface • Reflects prior injury to colon • Common in IBD but occur sporadically also • Vascular – brisk venous bleeding with resection or biopsy – rarely clinically significant Hamartomas – and hamartoma syndromes • 3 hamartomatous polyp syndromes – JPS (juvenile polyposis syndrome): SMAD4 or BMPR1A – PJS (Peutz‐Jeghers syndrome): STK11 (also called LKB1 – Cowden syndrome: (PTEN) 19 7/24/2012 Juvenile polyp • Synonymous with “retention polyp” – Distended mucus filled glands, multiple blood vessels, cystic dilation (hamartomas) • Prevalence of 1‐2 % in children age 4‐14y – 70% of patients have only 1 polyp; most others have 2 or 3 • Sporadic juvenile polyps not associated with CRC risk Juvenile polyposis syndrome (JPS) • Mutations in SMAD4 or BMPR1A • Increase risk of CRC, stomach, small bowel (if polyps present) • No physical exam clues • Consider if ≥ 3 JPs in colon, JPs in stomach or small bowel, JPs with + FH of JPS 20 7/24/2012 Screening in JPS (www.nccn.org) • Colonoscopy q 2‐3 y when sx begin or in late teens • EGD q 1‐3 y Peutz‐Jeghers Syndrome • STK11(LKB1) mutations • Oral and buccal mucosal hyperpigmentation • Colorectal cancer, breast, stomach, small bowel, pancreas, testis, cervix, uterus, ovary, lung 21 7/24/2012 Screening in PJS (www.nccn.org) • Colonoscopy q 2‐3y • Annual mammogram and breast MRI;biannual breast exam beginning at age 25 y • MRCP or EUS q 1‐2y beginning at age 30 y • EGD and small bowel imaging q 2‐3y beginning at age 10 • Annual pelvic, Pap smear, and transvaginal ultrasound beginning at age 18 y • Annual testis exam beginning at age 10 y Cowden’s syndrome • PTEN • Hamartomas in all sections of the bowel including esophagus • Not a clear increased risk of CRC • Very high risk of thyroid and breast cancer 22 7/24/2012 Inherited Adenoma Syndromes 23 7/24/2012 FAMILIAL ADENOMATOUS POLYPOSIS • • • • • • • • • <1% of all CRC autosomal dominant >95% penetrance hundreds of adenomas cancers in duodenum desmoid tumors Germline mutations in APC gene screening: sigmoidoscopy or colonoscopy commercial genetic testing available 24 7/24/2012 25 7/24/2012 Screening in FAP • Colonoscopy q 1‐2 y beginning at age 10 • Screening can be delayed to late teens in AAFP • Prophylactic colectomy when polyps unmanageable • EGD q 1‐3 y beginning age 25y • Annual physical exam including thyroid • If remaining rectum or ileal pouch, screen every 6 mo to 2 y 26 7/24/2012 UGI tract polyps, cancer in FAP • Gastric fundic gland polyps – Can be dysplastic but rarely become malignant • Duodenal adenomas – Most cancers arise at papilla – Spigelman score predicts non papilla risk Modified Spigelman score Points 1 2 3 # polyps 1‐4 5‐20 >20 Polyp size,mm 1‐4 5‐10 >10 Histology Tub TV Villous Dysplasia LGD ‐ HGD Stage 0:no polyps; Stage 1: 1‐4 points Stage 2: 5‐6 points; Stage 3:7‐8 points; Stage 4: 9‐12 points 27 7/24/2012 MUTYH‐Associated Polyposis: MAP • Autosomal recessive • Due to germline mutations in MYH genes • MUTYH defends against oxidative DNA damage (helps prevent G:C to T:A transversions) • Phenotype mimics FAP especially AAPC (increase in adenomas) but also increase in serrated polyps • Duodenal polyposis Screening in MAP • Colonoscopy q 2‐3 years beginning at age 25 y • EGD q 1‐3 y beginning at age 20‐25y 28 7/24/2012 Lynch Syndrome HEREDITARY NON POLYPOSIS COLORECTAL CANCER (LYNCH SYNDROME) • • • • • • • • • • • 2‐5% of all CRC Germline Mutation in Mismatch repair genes: MLH1, MSH2, MSH6, PMS1 Patients usually have only a few adenomas Autosomal dominant 70% penetrance Cancers at young age Rightward distribution Cancers at other sites: endometrium, small bowel, renal pelvis,ureter, brain, ovary, stomach Microsatellite instability Screening: colonoscopy Commercial genetic testing available 29 7/24/2012 Amsterdam II • Cancers can be at any of following sites: – Colorectum – Endometrium – Small bowel – Ureter – Renal pelvis 30 7/24/2012 31 7/24/2012 32 7/24/2012 Revised Bethesda Guidelines • CRC in patient < 50 y • Synchronous, metachronous or other LS tumor • CRC in patient < 60y with MSI‐H • CRC with ≥ 1 FDR with LS tumor with ≥ 1 diagnosed at age < 50 y • CRC and ≥ 2 FDR or SDR with LS tumor regardless of age 33 7/24/2012 Alternative to MSI testing • Immunostaining for MMR gene protein products – Easier to do – More widely available General Approach to Lynch Syndrome • Test tumor for MSI or perform immunostaining • Follow with BRAF test or hypermethylation assay if MHL1 mutated • If tumor positive (but BRAF negative or hypermethylation negative) then proceed with genetic testing • OR: MSI or immunostaining of all CRCs 34 7/24/2012 CRC Syndromes • Muir‐Torre Syndrome – HNPCC (sebaceous carcinomas) • Turcot’s syndrome – HNPCC (indolent glioblastoma multiforme) – FAP (medulloblastoma) Familial Colon Cancer Syndrome X • Clinical features – High risk of colorectal cancer (mimics HNPCC) – Little evidence of rapid conversion – Not at increased risk of extracolonic cancers • Genetic basis – Not yet determined 35