Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
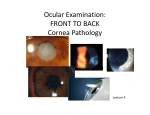
Corneal Stromal Dystrophies: A Clinicopathologic Review Emily S. Birkholz, MD, Nasreen A. Syed, MD, and Michael D. Wagoner, MD, PhD July 29, 2009 INTRODUCTION Corneal stromal dystrophies are a group of inherited disorders of the cornea that are caused by progressive accumulation of deposits within the stroma. These deposits are not caused by inflammation, infection, or trauma, but by genetic mutations that lead to abnormal proteins resulting in the accumulation of insoluble material within the stroma. The disorders may or may not affect vision and may or may not be symmetrical. They usually present in the second to third decade of life (1). Table 1 lists the different corneal stromal dystrophies. The major corneal dystrophies include lattice, granular, and macular dystrophy. A simple mnemonic for memorizing the corneal stromal dystrophy, the composition of the stromal deposit, and the method of staining these deposits is listed in Table 2. This mnemonic is well known by ophthalmology residents around the country. Table 1: Corneal Stromal Dystrophies • • • • • • • • Table 2: Mnemonic for remembering corneal stromal dystrophies • Marilyn — Macular Dystrophy • Monroe — Mucopolysaccharide • Always — Alcian Blue stain • Gets — Granular Dystrophy • Her — Hyaline • Man in — Masson Trichrome stain • Los— Lattice Dystrophy • Angeles — Amyloid • California — Congo Red Lattice Granular Avellino Macular Gelatinous Droplike dystrophy Schnyder Crystalline Corneal Dystrophy (SCCD) Francois-Neetens Fleck Dystrophy Congenital Hereditary Stromal Dystrophy GENETICS Four corneal dystrophies including granular, lattice, Avellino, and Reis-Bückler have been linked to a mutation in the Transforming Growth Factor Beta 1 gene (TGFβ1), also known as the BIGH3 gene. This gene, located on chromosome 5q31 codes for keratoepithelin, a protein secreted by corneal epithelium. This protein acts as an adhesion protein and is present in normal stroma. Being a small protein roughly the size of albumin, it has the capability to diffuse through the corneal stroma. When a mutation in the BIGH3 gene occurs, the keratoepithelin molecule is abnormal and accumulation of the insoluble protein occurs in the cornea (1). To date, thirty different mutations have been identified in the BIGH3 gene (2). Interestingly, the BIGH3 gene mutation was discovered in part at the University of Iowa. A group of researchers and clinicians including Edwin M. Stone, Robert Folberg, and Jay H. Krachmer mapped Avellino, granular, and lattice dystrophy to chromosome 5q in 1994 (3). LATTICE CORNEAL DYSTROPHY Lattice corneal dystrophy (LCD) is the most common of the corneal stromal dystrophies. It is an autosomal dominant, bilateral disease that typically presents toward the end of the first decade of life with symptoms of recurrent corneal erosions and decreased vision. It is characterized by lattice lines which are linear, radially oriented, branching refractile opacities described as "glass like" located in the anterior stroma (See Figure 1A and 1B). These lattice lines are usually restricted to the central cornea, sparing the periphery (1). Many patients with LCD will require surgical intervention for treating recurrent erosions and decreased vision. If the disease is located anteriorly in the stroma, patients can often be successfully treated with phototherapeutic keratectomy (PTK). Some require corneal transplantation. Because keratoepithelin, the protein produced by the BIGH3 gene, is produced mostly from corneal epithelium, the disease recurs in corneal grafts. 1 Figure 1. Lattice corneal dystrophy A. Left eye on retroillumination demonstrating anterior stromal deposits in lattice corneal dystrophy B. Left eye with higher power showing linear anterior stromal deposits. C. H&E stain of cornea with lattice. Note pink amorphous deposits in stroma D. A closer view of the pink, amorphous deposits E. Congo red stain, highlighting amyloid F. Apple‐green birefringence of amyloid with cross‐ polarization. 2 LCD is associated with a genetic mutation in the BIGH3 gene, resulting in deposits of amyloid within the anterior corneal stromal. Histopathologically, these deposits appear as amorphous pink deposits on hematoxylin and eosin (H&E) stains (See Figure 1C and 1D). Because the deposits consist of amyloid, they stain with Congo red stain and classically show apple green birefringence on cross-polarization (See Figure 1E and 1F) (1). Five subtypes of LCD have been identified. LCD type I is the classic form of LCD caused by a mutation in the BIGH3 gene resulting in isolated amyloid deposition in the cornea. LCD type II is a systemic amyloidosis affecting the skin, cranial nerves and cornea known as Meretoja syndrome. This presents in early adulthood with peripheral neuropathies, cranial neuropathies, hound-like facies, dry skin, blepharochalasis, protruding lips, and corneal lattice lines. This type has been linked to the gelsolin gene on chromosome 9, which encodes for an amyloid precursor protein which functions to remove actin from sites of injury and inflammation. LCD types III and IIIA present later in life with thicker linear opacities in the mid corneal stroma. LCD type III is an autosomal recessive condition presenting in the 7th-8th decade of life in which erosions rarely occur, and LCD IIIA is an autosomal dominant disease associated with a mutation in the BIGH3 gene that frequently leads to erosions and decreased vision in the 4th-5th decade of life. LCD type IV has been described as a late onset dystrophy occurring in the deep stroma, also associated with the BIGH3 gene (4) Figure 2. Type I granular corneal dystrophy. A. Slit lamp photo of Granular Corneal Dystrophy B. Note the “crumb‐ like” stromal deposits with clear intervening stroma. C. H& E stain of cornea showing eosinophilic “rock candy D. Hyaline material stains bright red with Masson‐ like” hyaline deposits in stroma Trichrome GRANULAR CORNEAL DYSTROPHY Granular corneal dystrophy (GCD) is a bilateral, autosomal dominant disease associated with a mutation in the BIGH3 gene that leads to the deposition of a hyaline material in the corneal stroma. It typically presents early in the first decade of life with gray-white, "crumb-like" opacities in the anterior to mid stroma. These opacities are discrete deposits located centrally, with clear cornea located in the periphery and clear cornea between deposits (See Figure 2A and 2B). The disease is typically asymptomatic early on, but with time the opacities can coalesce and lead to decreased vision. Recurrent corneal erosions can occur in GCD but at a lower incidence than in LCD (1,4). 3 Treatment early on in the disease process is often observation only. However, as the disease progresses, PTK and corneal transplantation may be needed to improve vision and erosion symptoms. Like LCD, the disease can recur in corneal grafts. Histopathologically the opacities are eosinophilic deposits often described as "rock candy like" in the anterior stroma made of a hyaline-like material. With time, the deposits progress into the deeper corneal stroma. The hyaline material stains bright red with Masson trichrome stain (See Figure 2C and 2D). Figure 3. Type II granular corneal dystrophy ‐ Avellino dystrophy A. Avellino dystrophy showing lattice like and granular like deposits in corneal stroma B. MassonTrichrome stain demonstrating anterior stromal hyaline deposits C. Congo red stain showing pink, amorphous amyloid deposits in the same corneal specimen. D. Cross‐polarization reveals apple green birefringence indicating amyloid. Three types of GCD have been described. GCD Type I is the classic form of GCD as described above. GCD Type II, also known as Avellino, or granular-lattice corneal dystrophy, is an autosomal dominant disease linked to a mutation in the BIGH3 gene that leads to a deposition of both hyaline and amyloid in the corneal stroma. Typically, patients present in their second decade with granular opacities like in GCD, but later in the disease process develop lattice lines as well (See Figure 3A and 3B). Histopathologically, the cornea will have stromal deposits that stain red with Masson Trichrome, indicating the presence of hyaline (See Figure 3C). In addition, staining with Congo red will demonstrate apple-green birefringence on cross-polarization indicating amyloid (See Figure 3D). The disease was thought to have originated from a family in Avellino, Italy. However, GCD type II has now been reported in patients from many other countries as well (2,4). GCD type III, also known as Reis Bückler or Corneal Dystrophy of Bowman's type I, is an autosomal dominant disease considered by some to be a superficial variant of GCD type I. Patients typically present with normal corneas at birth but develop painful recurrent erosions, opacification, and vision loss within the first decade of life. This disease has also been linked to the BIGH3 gene (2,4). Histopathology reveals anterior stromal and subepithelial 4 deposits of hyaline like material which disrupt and often replace Bowman's layer (See Figure 4A and 4B). The hyaline like material consists of rod like bodies which can best be seen with electron microscopy (1). Figure 4. Type III granular corneal dystrophy ‐ Reis‐Buckler dystrophy A. H&E of Reis Bückler showing destruction of Bowman’s layer and irregular epithelium B. Masson Trichrome stain demonstrating epithelial staining MACULAR CORNEAL DYSTROPHY Macular corneal dystrophy (MCD) is an autosomal recessive disease caused by a mutation on chromosome 16 that leads to a defect in the synthesis of keratan sulfate, the major glycosaminoglycan of the cornea. It is the least common of the major corneal stromal dystrophies, but thought to be the most severe. Although MCD is less common worldwide than LCD or GCD, it is the most common of the corneal stromal dystrophies in some areas such as Iceland and Saudi Arabia (5). Gray-white anterior stromal lesions similar to GCD appear in the cornea in the first decade of life. Unlike GCD, however, there is stromal haze between the deposits, and the entire cornea from limbus to limbus is often involved (See Figure 5A and 5B). Patients typically develop severe visual loss by the second to third decade of life due to diffuse corneal haze. PTK can be performed in some early cases of MCD. However, this condition is generally not as amenable to PTK as lattice or granular dystrophy and often requires corneal transplantation for treatment (6). Recurrence in grafts is less common in MCD than with granular or lattice dystrophy (1,2,4,5). The stromal deposits in MCD are composed of mucopolysaccharides that accumulate within the endoplasmic reticulum of keratocytes of the corneal stroma, extracellularly between stromal lamellae, and underneath and within the corneal epithelium (5). These deposits stain blue with Alcian blue (See figure 5C and 5D) (1). Three subtypes of MCD have been described based on the presence or absence of immunoreactive keratan sulfate within various tissues. Type I does not have immunoreactive keratan sulfate in the corneal stroma, keratocytes, sera or cartilage, and is the most common variant of MCD worldwide. Type IA lacks keratan sulfate in the stroma, sera, and cartilage, but has detectable levels inside keratocytes. Type II has keratan sulfate present at much reduced levels in the stroma, keratocytes, sera and cartilage (5). 5 Figure 5. Macular corneal dystrophy A. Slit lamp photo of macular corneal dystrophy. B. Note the haze between the corneal stromal deposits C. H&E of cornea with macular dystrophy. Note anterior stromal deposits and Bowman’s layer disruption D. Mucopolysaccharide deposits within keratocytes highlighted with Alcian Blue stain SCHNYDER CORNEAL CRYSTALLINE DYSTROPHY (SCCD) SCCD is an autosomal dominant, bilateral corneal stromal dystrophy linked to a genetic mutation on chromosome 1. The resulting metabolic defect of corneal keratocytes leads to crystalline lipid deposition. Clinically the disease presents with a ring-shaped accumulation of fine needle shaped polychromatic crystal deposits within Bowman's layer and the anterior stroma, and is often associated with a presenile peripheral lipid arcus (See Figure 6A and 6B). The disease typically presents in the first decade of life, and typically does not cause vision loss until past middle age. However, most patients by the seventh decade may require surgical treatment including corneal transplantation or PTK. Recurrences in grafts can occur. The disease has been linked with hyperlipidemia and genu valgum in some patients (4, 7). Histopathologically, birefringent cholesterol crystals composed of phospholipids and cholesterol deposit within keratocytes, in Bowman's layer, and between stromal lamellae. These lipid deposits stain red with Oil-Red-O stain. 6 Figure 6. Schnyder corneal crystalline dystrophy A. Slit lamp photo of Schnyder Corneal Crystalline Dystrophy. B. Centrally located crystalline deposits C. H&E of cornea with SCCD D. Oil Red O stain highlights cholesterol crystals which appear red. OVERVIEW: CORNEAL STROMAL DYSTROPHIES EPIDEMIOLOGY • Autosomal Dominant disease o Granular corneal dystrophy (GCD) o Lattice corneal dystrophy (LCD) o Schnyder’s crystalline corneal dystrophy (SCCD) • Autosomal Recessive o Macular corneal dystrophy (MCD) • Present in 1st - 3rd decade of life SIGNS • Recurrent erosions • Bilateral corneal stromal deposits in various patterns o Crumb-like deposits for GCD o Lattice lines for LCD o Diffuse haze and stromal deposits for MCD o Central crystalline deposits with surrounding Arcus for SCCD SYMPTOMS • Initially none • Bilateral recurrent erosions causing pain, tearing, and foreign body sensation • Over time can have decreased vision TREATMENT • Observation o Early in course o Lubrication o Manage recurrent erosions with bandage contact lens and topical antibiotic (erythromycin ointment or 3rd-4th generation fluoroquinolone) • Phototherapeutic Keratectomy • Corneal Transplantation o If recurrent erosions severe or if decreased vision o Recurs in grafts 7 REFERENCES 1. Keefe KS, Milman T, Rodrigues MM, Hidayat AA. Conjunctival and Corneal Pathology. Albert and Jakobiec's Principles and Practice of Ophthalmology, 3rd edition. Saunders. 2008: 3592-3595. 2. Poulaki V, Colby K. Genetics of anterior and stromal corneal dystrophies. Seminars in Ophthalmology, 2008; 23: 1,9-17 3. Stone EM, et al. Three autosomal dominant corneal dystrophies map to chromosome 5q. Nature genet. 1994; 6: 47-51. 4. Bron AJ. Genetics of the Corneal Dystrophies: What we have learned in the past twenty five years. Cornea 2000; 19(5): 699-711. 5. Al-Swailem SA, Al-Rajhi AA, Wagoner MD. Penetrating Keratoplasty for Macular Corneal Dystrophy. Ophthalmology 2005;112: 220-224. 6. Badr IA, Wagoner MD. Phototherapeutic Keratectomy for Macular Corneal Dystrophy. J Refract Surg 1999;15:481-484. 7. Shearman AM, Hudson TJ, Andresen JM, et al. The gene for Schnyder's crystalline corneal dystrophy maps to human chromosome 1p34.1p36. Hum Mol Genet 1996;5:1667-72. suggested citation format: Birkholz ES, Syed NA, Wagoner, MD. Corneal Stromal Dystrophies: A Clinicopathologic Review. EyeRounds.org. August 4, 2009 [cited --insert today's date here -- ]; Available from: http://www.eyerounds.org/cases/43-corneal-stromal-dystrophies.pdf 8