Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Severe Liver Disease
Ronald S. Walton DVM, MS
Diplomate ACVIM and ACVECC
Puget Sound Veterinary Referral Center
Tacoma, Washington USA
Does this patient have liver disease?
Does this patient have liver disease?
Does this patient have liver disease?
Does this patient have liver
disease?
Does this patient have liver
disease?
Does this patient have liver disease?
They all do
Outline
► Introduction
► Etiology
► Pathogenesis
► Diagnostic
Evaluation Plan
► Treatment
► Prognosis
► Focus
is Acute Liver Failure (ALF) and injury
Introduction
► Liver
is the metabolic center piece of normal
homeostatic mechanisms in the body
► Pivotal Roles
Protein, carbohydrate and fat metabolism
Detoxification
Formation of most coagulation factors
► Many
integral and central actions to normal
body function
no single test = liver failure
► Large
reserve capacity and remarkable
regenerative capability
Background
► Study of
50 dogs with liver failure
22 breeds
Median age was 6 years (1m-13yr)
Presenting signs
►Anorexia
►Vomiting
►Polydipsia
►Neurologic
signs initial 6/50
Progression to Hepatic Encephalopathy 21/50
►
ACVIM 2011
Background
► Common
Clinicopathologic Abnormalities
Increased bilirubin 47/48
Increased ALP 45/48
Increased ALT 42/48
Increased PT/aPTT 36/39
Decreased platelets 36/48
Decreased albumin 27/48
ACVIM 2011
Background
► Defined
etiology with hepatic biopsy16/32
Neoplasia 12/32
Infarction 2/32
Congenital PSS 1/32
Hepatic Lipidosis 1/32
► Defined
etiology with serology or history
Leptospirosis 6/50
Drug toxicity 3/50
Mushroom toxicity 1/50
ACVIM 2011
Background
► Secondary complications
Ascites (6/50)
DIC (6/50)
Renal failure (5/ 50)
PTE (2/50)
Hemoabdomen (2/50).
ACVIM 2011
Background
► Only
7 dogs survived to discharge.
ACVIM 2011
Introduction
► Acute
Liver failure (True Emergency)
rapid functional impairment
unable to perform its synthetic and excretory
homeostatic roles
Often without prior evidence or history of liver
disease
Clinical outcome of ALF often depends on rapid
and aggressive supportive care
Introduction
► Chronic
Liver Failure
associated with irreversible changes that have
accumulated over months to years
regenerative capacity is often exhausted before
clinical signs are evident
Introduction
►Basic Premis
Regardless of the etiology and pathogenesis:
►Similar supportive/symptomatic therapy is
indicated until a final diagnosis can be
reached
►The diagnosis and etiology may take several
days and require a hepatic biopsy to
determine a definitive diagnosis.
Etiology
► Infectious
Agents
Viral (CAV I, FIP)
Bacterial (Leptosporosis, Bacillus,
Clostridial)
Fungal (Histoplasmosis)
Protozoal
►(Toxoplasmosis,
Cytauxzoonosis)
Babesiosis and
Etiology
► Chemical
and pharmaceutical agents
Acetaminophen/ Diazepam – cat
Carprofen/ Thiacetarsemide-dog
►Drug
induced idiosyncratic reaction primary
cause in people
► Infiltrative
Disease
(Neoplasia , inflammatory cells or lipid)
Etiology
► Ischemia
and Hypoxic Injury
Severe shock, right-sided heart failure,
thrombosis, neoplasia, trauma and vascular
anomalies
► Metabolic
Copper storage disease and hepatic lipidosis
► Anatomic
Variants
Portosystemic shunting of blood via either
congenital or acquired vascular connection(s)
►portal
and systemic circulations
Pathogenesis
► Hepatic
response to injury
Hypoxia
Free radical exposure or generation
Membrane lipid peroxidation,
Depletion of essential intracellular compounds
Intracellular toxin production
Toxin binding to DNA and RNA
Cholestatic injury
Direct effects on hepatobiliary system
►Endotoxin,
viral, parasitic, and immune complexes
Pathogenesis
► Hepatic
Dysfunction
Carbohydrate, lipid , cholesterol, nitrogen and protein
metabolism
Microsomal enzyme system (P450)
Hepatic Encephalopathy (HE) *
Cerebral Edema *
Coagulopathy *
Bilirubin metabolism and jaundice
Portal hypertension and ascites
Hepatorenal syndrome
Diagnostic Evaluation Plan
► History
Typically vague and shares a commonality with
many disease processes
Much of the reserve capacity of the liver lost
before signs or symptoms
Longstanding but, unrecognized disease process
Known hepatotoxins
Thermal or traumatic injury
Diagnostic Evaluation Plan
Clinical Signs and Physical exam
General
►
►
►
►
►
►
►
►
►
Anorexia
Depression
Weight loss
Small stature for breed
Poor hair coat
Nausea
Vomiting
Diarrhea
Dehydration
Diagnostic Evaluation Plan
More specific (not pathognomonic)
►Abdominal
enlargement
►Hepatodyna
► Jaundice
► Acholic feces
► Behavioral changes and signs of HE (circling, ataxia,
pacing, head pressing, blindness, salivation, tremors,
seizures, coma)
► Coagulopathy
► Pu/Pd
Diagnostic Evaluation Plan
► Clinpath
Findings:
Hematology (anemia, microcytosois {PSS}, target cells,
acanthocytes, leukocytosis to leukopenia, platelets
variable
Biochemical Testing:
► Liver
Enzymes * ( ALT and AST, ALKP, GGT)
► Hepatic Function Testing (SBA, and ATT)
► Other( TBili, Alb, Glob, BUN, Glucose, Chol, Lytes
Urinalysis
► Low
USG, Ammonium Biurate/Bilirubin Crystals, Bilirubin,
Urobilinogen absence
Coagulation Testing
► (PT,
APTT, ACT)
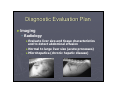
Diagnostic Evaluation Plan
► Imaging
Radiology
►Evaluate
liver size and tissue characteristics
and to detect abdominal effusion
►Normal to large liver size (acute processes)
►Microhepatica (chronic hepatic disease)
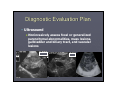
Diagnostic Evaluation Plan
Ultrasound
►Noninvasively
assess focal or generalized
parenchymal abnormalities, mass lesions,
gallbladder and biliary tract, and vascular
lesions
Diagnostic Evaluation Plan
Additional
►Abdominocentesis
►Serology
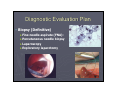
Diagnostic Evaluation Plan
Biopsy (Definitive)
►Fine
needle aspirate (FNA):
►Percutaneous needle biopsy
►Laparoscopy
►Exploratory laparotomy
Treatment
► Symptomatic
► General
Support
Major organ systems
Fluid, Electrolyte and Acid-Base Balance
Hepatoencephalopathy (HE) *
Cerebral edema *
Hemorrhage and anemia *
Ascites *
Infection and endotoxemia
Nutritional
Treatment
► Prevent
Formation and Absorption of Enteric
Toxins
Critical Patient/Hepatic Coma:
► Cleansing
enema with warm H2O until clear effluent
► Retention enemas Povidone iodine solution (1:10
dilution with water) leave in 10 minutes then flush with
water
► 30% lactulose solution (5-10ml/kg) mixed with
neomycin at 22-mg/kg leave for 20-30minutes
Treatment
► Prevent
formation and absorption of
enteric toxins
Maintenance therapy:
►Metronidazole
(7.5mg/kg q 12hr PO)
►Amoxicillin (22 mg/kg q 12hr PO)
►Neomycin (22mg/kg q 8-12 hr PO)
►Lactulose (0.25 to 0.5 ml/kg q 8-12 hr PO)
►IV Fluids (0.45% NaCl + 2.5% Dextrose)
Avoid alkalinizing solutions (esp. lactate)
Treatment
► Control
GI Hemorrhage
Treat GI Ulceration
►Famotidine
(0.5-1.0mg/kg q 12-24 hr PO
►Carafate (1g/25kg q 8 hr PO)
Correct Coagulopathy
►Vit
K1 (1.5-2 mg/kg q 12 hr SC or IM
►Fresh plasma
►Whole blood transfusion
►D/C Glucocorticoids, aspirin and
NSAIDs
Treatment
► Control
Seizures
Keppra ( levetiracetam)
► (20
mg/kg IV)
► Oral follow-up 20 mg/kg tid
Refractory seizures/status epilepticus
► use
general anesthesia with propofol
► mechanical ventilation
► maintain normal PaO2 and PaCO2.
Avoid benzodiazepines
► (Flumazenil
0.02 mg/kg?)
Treatment
► Decrease
cerebral edema
Mannitol (0.5-1.0 gm/kg IV) followed by
Furosemide (1-2 mg/kg q 12 hr)
Treatment
► Nutritional
Support
Initial NPO for HE
Long term management
► Easily
digested high carbohydrate diet. Moderate
protein restriction on a dry matter basis to 18-22% for
dogs and 30-35% for cats.
► Protein source should be dairy or vegetable source
High BCAA to AAA ratio
► Sodium
restriction
► Multi-vitamin supplement, high in B-vitamins
► Soluble dietary fiber (psyllium mucolloid 1-3 tsp./day)
Treatment
► Prevent
and Control Hypoglycemia
Severe hypoglycemia
►Administer
50% dextrose IV (0.5-1.0ml/kg
diluted in sterile water to 20-25% solution
►Add dextrose to IV fluids as needed (2-5%) to
maintain adequate blood glucose levels
Directed Treatment for Acute
Hepatic Injury
► Hepatic
Ischemic Injury
Ensure adequate volume support
Ensure adequate O2 delivery
Fresh transfusion with whole blood or packed
RBC’s and supplemental oxygen as needed
Ensure eugylcemia
Glucocorticoids (hydrocortisone sodium
succinate 30-100mg/kg)
Directed Treatment for Acute
Hepatic Injury
► Hepatic Oxidative
Injury (Specific Toxin)
Acetaminophen toxicity
►N-Acetylcystine
(140mg/kg IV loading dose
and subsequent doses of 70-140 mg/kg IV or
PO q 6 hrs.)
►Cimetidine 5 mg/kg IV or PO for duration of NAcetylcystine Therapy
Directed Treatment for Acute
Hepatic Injury
► Hepatic Oxidative
Injury (Specific Toxin)
Amanita Mushroom Intoxication
►Gastric
decontamination if acute ingestion
►Dexamethasone (0.3-0.5 mg/kg q 1hr IV)
►Penicillin G 250 mg/kg day
Silymarin/Silbinin Legalon® SIL 5mg/kg loading
then CRI 20 mg/kg/day (still in clinical trials)
Directed Treatment for Acute
Hepatic Injury
► Hepatic Oxidative
Injury (General or
Suspected Toxin non-specific injury)
Cimetidine 5 mg/kg IV (only if blocking P-450
enzyme system indicated
S-Adenosyl-Methionine SAM-e Denosyl® 20
mg/kg/ day
Directed Treatment for Acute
Hepatic Injury
Silymarin/Silbinin Legalon® SIL 5mg/kg loading
then CRI 20 mg/kg/day (still in clinical trials) ??
►Oral
50-250 mg per day
Vitamin E 100-400 IU PO /day
Ursodeoxycholic acid (10-15 mg/kg q 24 hr PO)
Prognosis
► Variable
► Keys
to improvement
Rapid recognition
Aggressive therapeutic support (HE, Cerebral
Edema, Coagulopathy)
Degree of damage
Remaining regenerative ability
► Acute
presentation of CHF uniformly poor
► Biopsy is the key
Summary
►
Strategies to increase survival in ALF are
urgently needed
ACVIM 2011
Questions