Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
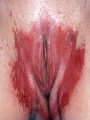
Papule/nodule A wide spectrum of benign, premalignant, and malignant lesions may involve the vulva NEOPLASIA Vulvar intraepithelial neoplasia Most vulvar intraepithelial neoplasia lesions are multifocal and located in the nonhairbearing parts of the vulva cancer: Most patients with vulvar cancer present with a unifocal vulvar plaque, ulcer, or mass (fleshy, nodular, or warty) on the labia. Lichen sclerosus and erosive lichen planus may vulvar to predispose cancers Squamous cell cancer and lichen sclerosus FLESH COLORED PAPULE/NODULE Vestibular papillae discrete, small papules located symmetrically around the edge of vestibule benign and usually asymptomatic do not require treatment confused with condyloma acuminata except condyloma tend to fuse together and are not confined to the vestibule. P Acroc hordon : (skin tag, fibroepithelial polyp, soft fibroma) a benign outgrowth of normal skin appear as pedunculated lesions on narrow stalks and tend to be more numerous in patients with diabetes or obesity and in areas of chronic friction. Removal is indicated when the patient is symptomatic Cysts : Bartholin gland ,pilonidal, epidermoid ,dermoid, Gartner, and mucous cysts are benign lesions, but can be associated with bothersome symptoms treatment is often requested by the patient. Genital warts (condyloma acuminata) Genital warts, caused by (HPV), may be of flat, filliform, verrucous, pedunculated, or giant morphology. They may be flesh colored or pigmented. Lesions of secondary syphilis may have a wart-like appearance, but are not true warts. Molluscum contagiosum : umbilicated translucent or pearly papules due to infection from a member of the poxvirus family. in healthy adult woman may indicate an underlying immunosuppressive disorder. Treatment : destructive (eg, cantharidin, cryotherapy) or immunomodulating (eg, imiquimod) Syringoma : benign neoplasms of the eccrine sweat glands. multiple, 1 to 2 mm, flesh-colored to yellow papules arranged symmetrically on the labia majora., heat and sweating, menstruation, or pregnancy may provoke pruritus in vulvar syringomas. Excision or ablation is curative. In some patients, topical atropin or tretinoin WHITE PATCH/PLAQUE Hyperkeratosis or lichen simplex chronicus : Raised white or dark colored plaques on the vulva are associated with hyperkeratosis secondary to chronic rubbing or scratching. Erosions and/or excoriations may also be evident.. Biopsy of affected skin may be indicated if the underlying disorder is uncertain. Lichen sclerosus (white, finely wrink& atrophic patches ) May develop with minor trauma, hemorrhage may be present. Vulvar itching and have typical clinical findings that suggest the diagnosis. A biopsy may be indicated to exclude malignancy if unresponsive to therapy or if lesional skin demonstrates morphologic changes. Be treated medically with a potent topical corticosteroid ointment, such as clobetasol 0.05 percent ointment and followed closely Papule/nodule Dermatofibroma usually present as firm, hyperpigmented papules that invaginate (dimple sign) with lateral pressure. It is hypothesized that they arise after trauma. Ectopic breast Present as a hyperpigmented nodule on the vulva on the milk line, which extends from the axilla to the groin. Symptoms may develop with pregnancy or menstruation' Kaposi's sarcoma Consists of dusky erythematous to violaceous papules that may ulcerate and become painful. Extra-genital skin, in particular the oral mucosa, should be examined (HIV)infection should be ruled out Compound melanocytic nevi: Darker than intradermal nevi; both are often well circumscribed, dark-colored, soft papules. Definitive diagnosis is made with a biopsy Fox-Fordyce: Disease is an extremely pruritic, monotonous eruption of minute, dark papules involving apocrine glands Red macule/patch/plaque Dermatitis : Atopic, irritant, and allergic dermatitis, and neurodermatitis of the vulva erythematous lesions. Long-standing dermatitis hyperpigmentation and thickening of the skin with lichenification. Avoidance of offending agents is the mainstay of treatment of contact and allergic dermatitis. Psoriasis : Psoriasis is characterized by erythematous plaques with micaceous scale on the scalp, elbow, knees, palms, and soles. It is often associated with nail changes Lichen planus violaceous, flat-topped papules with lacy, white scales the characteristic lesions. Involved areas of the vestibule or vagina often appear as erythematous erosions and patients may develop shortening and narrowing of the vagina. Atrophic vulvitis Is a manifestation of hypoestrogenism; although the vagina is much more sensitive to estrogen deprivation than the vulva. Infection : The differential diagnosis of erythematous vulvar lesions should also include infections. Candida infection presents as moist erythema with satellite lesions Excessive vaginal discharge from bacterial vaginosis or trichomoniasis may contribute to erythema and maceration of vulvar skin. Cherry angioma : Discrete benign red papules; they are often present on the trunk and rarely occur on the vulva Treatment by destructive modalities (eg surgery, cautery) Urethral lesions : A midline polypoid lesion may be a urethral caruncle or urethral prolapse. Satisfactory treatment may be achieved with topical estrogen cream alone. Endometriosis : Develops after vulvar implantation of endometrial tissue following a surgical procedure. PUSTULES, VESICLES, AND EROSION Folliculitis: Develop in any hair-bearing surface; Staphylococcus aureus can be cultured from the skin lesions. Furunculosis : Furunculosis and carbuncles may develop with long-standing, severe folliculitis. Hidradenitis suppurativa : Manifests with pruritus, erythema, and local hyperhidrosis. As the area heals, it becomes fibrotic and new nodules develop inflammatory masses. Hyperpigmentation, scars, and pitting are seen on the skin. Candida Herpes simplex virus (HSV) : Multiple, painful vesicles or ulcerating lesions It also often appears as grouped (herpetiform distribution( Evident due to the moisture and friction in this area. Fever, malaise, and lymphadenopathy Scabies and insect bites Fixed drug reaction : Usually demonstrate discrete, hyperpigmented bullae or erosions that recur in the exact same Location with repeat medication administration Herbal supplements, phenolphthalein, tetracycline,NSAIDS, and sulfonamides Improvement should occur within two weeks of stopping the causative drug. ULCER/FISSURE Infection HSV Syphilitic chancre Chancroid ulcer Lymphogranuloma venereum Granuloma inguinale Malignancy Systemic disease Drug TREATMENT: Vulvar skin care Soaks Lubricants Topical analgesics and oral antihistamines Estrogen Antimicrobial drugs Antiinflammatory agents (oral or topical) Combination topical antimicrobial and anti-inflammatory agents Surgery Geriatric vulvar lesions in postmenopausal women are atrophy due to hypoestrogenemia and cancer. These lesions can be asymptomatic or have nonspecific symptoms such as itching. ".) Immunocompromise at risk for severe manifestations of common infections, as well as atypical infections prone to development of certain types of premalignant and malignant disease.