Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
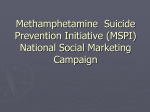
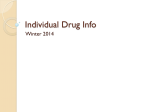
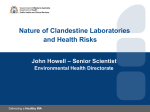
Drug and Alcohol Dependence 75 (2004) 37–45 Buprenorphine versus methadone for opioid dependence: predictor variables for treatment outcome G. Gerra a,∗ , F. Borella a , A. Zaimovic a , G. Moi a , M. Bussandri a , C Bubici a , S. Bertacca b a Addiction Research Center, Servizio Tossicodipendenze, Azienda Unità Sanitaria Locale, Parma, Via Spalato 2, 43100 Parma, Italy b Servizio Tossicodipendenze, Azienda Unità Sanitaria Locale, Parma, Italy Received 23 May 2003; received in revised form 17 November 2003; accepted 25 November 2003 Abstract The present study compared in a clinical non-experimental setting the efficacy of buprenorphine (BUP) and methadone (METH) in the treatment of opioid dependence: all the subjects included in the study showed severe long-lasting heroin addiction. Participants (154) were applicants to a 12 weeks treatment program, who were assigned to either METH (78) (mean doses 81.5 ± 36.4 mg) or BUP (76) (mean doses 9.2 ± 3.4 mg) treatment. Aim of the study was to evaluate patient/treatment variables possibly influencing retention rate, abstinence from illicit drugs and mood changes. METH patients showed a higher retention rate at week 4 (78.2 versus 65.8) (P < 0.05), but BUP and METH were equally effective in sustaining retention in treatment and compliance with medication at week 12 (61.5 versus 59.2). Retention rate was influenced by dose, psychosocial functioning and not by psychiatric comorbidity in METH patients. In contrast, BUP maintained patients who completed the observational period showed a significantly higher rate of depression than those who dropped out (P < 0.01) and the intention to treat sample (P < 0.05). No relationship between retention and dose, or retention and psychosocial functioning was evidenced for BUP patients. The risk of positive urine testing was similar between METH and BUP, as expression of illicit drug use in general. At week 12, the patients treated with METH showed more risk of illicit opioid use than those treated with BUP (32.1% versus 25.6%) (P < 0.05). Negative urines were associated with higher doses in both METH and BUP patients. As evidenced for retention, substance abuse history and psychosocial functioning appear unable to influence urinalyses results in BUP patients. Buprenorphine maintained patients who showed negative urines presented a significantly higher rate of depression than those with positive urines (P < 0.05). Alternatively, psychiatric comorbidity was found unrelated to urinalyses results in METH patients. Our data need to be interpreted with caution because of the observational clinical methodology and non-random procedure. The present findings provide further support for the utility of BUP in the treatment of opioid dependency and demonstrate efficacy equivalent to that of METH during a clinical procedure. BUP seems to be more effective than METH in patients affected by depressive traits and dysphoria, probably due to antagonist action on -opioid receptors. Psychosocial functioning and addiction severity cannot be used as valuable predictors of BUP treatment outcome. High doses appear to predict a better outcome, in term of negative urines, for both METH and BUP, but not in term of retention for BUP patients. © 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Buprenorphine; Methadone; Heroin; Depression; Psychosocial functioning; Treatment 1. Introduction A review of clinical research including randomized, controlled trials has shown buprenorphine (BUP) to be equal in effectiveness to methadone (METH) in the maintenance treatment for opioid dependence (Raisch et al., 2002). Ac∗ Corresponding author. Present address: Dipartimento Nazionale Politiche Antidroga, Via Quintino Sella 69, 00187 Roma, Italy. Tel.: +39-06-42454251. E-mail address: [email protected] (G. Gerra). cordingly, BUP and METH did not show any significant difference, with regard to urinalyses and retention, in a multi-center study in our country (Pani et al., 2000) and previous findings demonstrated BUP efficacy comparable to METH in the therapy of heroin dependent patients (Johnson et al., 2000; Strain et al., 1994). Higher daily BUP and METH maintenance doses versus lower doses appear to be more effective for reducing illicit opioid use, when evaluated in a random double blind trial (Schottenfeld et al., 1997). To this purpose, Ling findings indicate BUP maintenance at 8 mg per day to be less than 0376-8716/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.drugalcdep.2003.11.017 38 G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 optimally efficacious (Ling et al., 1996) and, accordingly, Eder suggests that lower retention in BUP patients may be attributable to low doses BUP limit, particularly for those subjects with high levels of dependence (Eder et al., 1998). The number of days that a patient remained in treatment in a randomized trial was reported significantly higher for those receiving 16–32 mg of BUP three times a week and daily high-dose METH (60–100 mg) than for those receiving low-dose METH, without significant differences between BUP and METH. Nevertheless, both the drugs were found to substantially reduce the use of illicit opioids with similar rates of negative urines (Johnson et al., 2000). In agreement with these findings, a meta-analysis of controlled clinical trials confirmed that the effectiveness of high doses of BUP seems to be similar to high doses of METH for both retention rates and illicit opioid use (Farre et al., 2002). On the other hand, the difficulty to begin treatment with BUP in comparison with METH in high dependent patients, as reported by Uehlinger et al. (1998), and lower retention rate in BUP patients evidenced by Mattick et al. (2003) have suggested the need to induct patients more rapidly onto BUP than METH, and start treatment at a higher BUP dose, but also the opportunity to investigate other variables possibly influencing the effects of BUP in particular subsets of addicts was not excluded. Accordingly, a meta-analytic evaluation of five randomized clinical trials comparing BUP to METH, with better outcome for METH patients in term of retention and negative urinalyses, has indicated the need of further research to determine if BUP treatment is more effective than METH in particular settings or in particular subgroups of patients (Barnett et al., 2001). The hypothesis that a specific subtype of addicted individuals may be benefiting from BUP was also formulated by Fischer et al. (1999a,b), who reported better retention rate in the METH maintained group, and significantly lower rates of illicit opiate consumption in BUP patients. The pronostic factors able to characterize patients-subtypes and to predict BUP outcome, in comparison with METH, are still unclear and confused. Administration of BUP has been proposed to be reserved for patients addicted to opiates for less than 10 years, non-depressive and with low disinhibition on Zukerman’s scale (Laqueille et al., 2001). Levels of psychosocial functioning and global assessments of functioning were significantly higher for BUP responders than non-responders (Resnick et al., 1991) and patients who dropped out from BUP treatment were reported to differ significantly from those who stayed, in terms of a higher level of psychopathological symptoms, and a lower level of social integration (Pani et al., 2000). Finally, also gender differences have been evidenced among the antecedents of a positive outcome, being female gender with lifetime sedative dependence associated with significantly better retention (Schottenfeld et al., 1998). For these reasons, in the present naturalistic observational study we investigated the effectiveness of BUP, in rela- tionship with different patient variables, particularly with personality and behavioral traits, psychiatric comorbidity, heroin addiction and previous treatment history, in comparison with METH maintenance treatment. Aim of the study was to evaluate the possible factors affecting the endpoints of retention rate, reduction of illicit drug use and psychiatric symptoms improvement, during BUP and METH treatment. The hypothesis was that BUP treatment may differently influence outcome variables, respect to METH, not only in relationship with addiction severity or dose levels, but also with individuals personality traits and comorbid disorders, due to its specific -receptors agonist/-antagonist profile. The study was conducted to determine the responses to BUP (76) and METH (78) of heroin dependent patients, in the first 12 weeks of a maintenance treatment period, measuring treatment and patient variables capacity to affect retention rates, changes in psychometric measures, craving scores and positive urine rates. 2. Materials and methods 2.1. Study population Heroin-dependent subjects were selected from among patients participating in Parma Addiction Service Program (Servizio Tossicodipendenze) of the public health system. Addiction Services in Italy provide outpatients treatment programs, with different therapeutic and rehabilitative strategies: METH, BUP and naltrexone are administered in association with possible psychosocial intervention, such as psychotherapy, family therapy, group therapy, social support and medication for dually diagnosed patients. Most of the patients in Italian Addiction Services are seeking treatment for heroin dependence, although the same Services offer rehabilitative programs also for cocaine and alcohol addiction. No exclusion criteria are applied to select patients in the public health system. All the patients have been evaluated using a self-report and observer-rated questionnaire, a psychometric test, and a psychiatric diagnostic screening. Data describing a detailed history of the patients were also obtained from the drug addiction center records. To be eligible for the study, patients had to enter in METH or BUP maintenance treatment during the 12 months of 2002. After we obtained informed consent, 78 METH patients (60 men and 18 women, mean age: 33 years) and 76 BUP patients (55 men and 21 women, mean age: 32 years) were included in the study. The 12 weeks clinical evaluation was conducted as an observational, non-randomized, study that did not influence treatment choice decision, dosage, psychosocial intervention and diagnostic assessment. Participants were heroin-dependent from at least 7 years (mean: 10.1 ± 3.2). Daily intake of heroin ranged from 1.5 to 3.0 g of street heroin. Previous consumption of other drugs of G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 Table 1 Buprenorphine Heroin dependence years Mean daily heroin dose (g) Previous cocaine use (%) Good interpersonal relationship (%) Unemployed (%) Legal problems (%) Alcohol problems (%) Previous methadone treatment (%) Previous residential treatment (%) Without psychiatric comorbidity (%) Depression (%) Methadone Significance 10.7 ± 3.5 2.3 ± 0.6 n.s. n.s. 12.5 37.7 11.9 36.8 n.s. n.s. 48.4 43.6 16.5 51 50.5 45.2 18.6 59 n.s. n.s. n.s. n.s. 38 40.4 n.s. 53.8 52.5 n.s. 19.7 17.9 n.s. 9.5 ± 2.8 2.1 ± 0.9 abuse and psychotropic agents or excessive alcohol intake was recorded. No significant difference in heroin exposure extent (years and dosage), or other psychotropic drugs use (11.9 and 12.5% of cocaine; 9.2 and 8.8% of ecstasy and 28.1 and 26.4% for benzodiazepines, respectively for METH and BUP), was evidenced between BUP and METH patients. Among the patients selected for the study, 56% had been submitted to previous METH treatment, respectively 59% in METH group and 51% in BUP group. Other characteristic of the patients are included in Table 1: no significant differences between BUP and METH groups have been evidenced at baseline. Previous residential treatment was reported in 39.1% of the sample prior to their beginning the study (respectively 40.4 and 38.0% for METH and BUP). Benzodiazepines were prescribed to 10.2% of the MMT patients and 11.8% of the BMT patients; 6.4% of the METH patients and 5.2% of the BUP patients were prescribed antidepressant agents and 2.4 and 3.3% neuroleptic agents, in association respectively to METH and BUP treatment. METH or BUP treatment was integrated with psychosocial support, including weekly individual counseling and money vouchers, for all the patients. Counseling sessions followed cognitive–behavioral methodology and the vouchers for a small amount of money were used as positive reinforce to obtain negative urines. Patients with significant psychiatric comorbidity were also referred to a weekly meeting with the psychiatrist and possible psychotropic medication. The procedures followed were in accord the Helsinki declaration of 1975. Following the criteria of the program of Parma, no patient was discharged because of consecutive positive urine test results. 39 METH or BUP was reached on the first week of treatment: the patients treated with BUP received a first dose of 2 mg, 8 h after the last injection of heroin, or 24 h after the last METH administration; then they received other 2 or 4 mg of BUP, when did not present withdrawal symptoms, during the first day. Adjunctive BUP doses were administered to rapidly reach high doses: in some cases, first day BUP was limited to 2 mg because withdrawal symptoms were clearly BUP-induced. METH patients received 40 mg on the first day, in refracted doses of 20 mg. Other changes in METH or BUP doses have been permitted on the first week of the treatment: then stable doses were administered for 12 weeks. Flexible dosing schedule was applied in the first week of treatment, but rarely in the following 3 months (5–10 mg of METH or 2 mg of BUP in two and three patients respectively), for clinical reasons: after obtaining an agreement about appropriate doses with the patients, they were asked to evaluate their behavioral reaction to stable doses for at least 3 months, without focusing continuously on medication. METH was administered daily in the outpatient center for 64% of the subjects; 36% of the patients were permitted to bring their METH home three times a week. BUP was administered daily in the outpatient center for 61% of the patients and three times a week for 39% of the patients. Weekly take home METH or BUP was not permitted in the first three months of treatment. The “three times a week” schedule was not used as a behavioral privilege, but independently from negative urines. All the patients were submitted to self-report and observer-rated questionnaire, Symptoms Check List 90 (SCL-90), craving 100 mm Visual Analog Scale (VAS), DSM IV clinical psychiatric assessment and Minnesota Multiphasic Personality Inventory (MMPI 2) (Hathaway and McKinley, 1989) on week 1. Retention rates, SCL-90 scores, VAS craving scores were measured again on week 4 and week 12, at the end of the study. The main measure available for assessing illicit drug use was urinalysis. The week immediately before and during the three month of the study, urine samples were screened twice a week on random days for amphetamines, methamphetamines, morphine, METH, cannabis, cocaine, barbiturates, benzodiazepines and alcohol. Urinalyses were performed with immunoenzymatic methodology (polyclonal antibodies with glucose-6-phosphate dehydrogenase: EMIT, Syva, Italy) and positive results were confirmed by thin layer chromatography, using commercial kits (Toxi-lab; ANSYS Technologies, Lake Forest, CA). A total of 26 urine samples (2 before admission and 24 during the 12 weeks) have been collected for each patient: missing urinalyses have been counted positive. 2.3. Data collection strategy 2.2. Study design All the patients were evaluated for 12 weeks after the beginning of the opioid substitution therapy. Stable dosage of The data collection strategy consisted of a seven-page form for BUP and METH maintenance program counselors to complete for each patient in the outpatient program who 40 G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 entered substitution treatment during 2002. The patient survey form requested the following information: treatment identification (BMT or MMT); patient identification; previous treatment; employment status; highest school grade completed; quality of interpersonal relationships; marital status; legal problems; commitments; time in prison; number of arrests; number of violent crimes; perception of alcohol as a current problem. New selective psychopharmacological treatment associated with METH or BUP was also recorded. The quality of interpersonal relationships was defined as bad (no affective relationship with family members or friends), good (close affective relationships with family members or friends), or maintained with difficulties (visual analog score of 100 mm: good = more than 70; bad = less than 30; maintained with difficulties = between 31 and 70). Employment status was defined as unemployed, stable job (the same company during the year, regularly paying taxes), or unstable job (different short-term jobs during the last 12 months). Alcohol-correlated problems were defined as having been drunk frequently during the last month (weekly or more frequently), behavioral changes, health consequences, or automobile accidents related to ethanol consumption. Alcohol levels in urines were also utilized to screen severe alcohol abusers, being urines positive in the morning interpreted as a sign of heavy ethanol use in the night before. Legal problems were classified with or without violence. The counselors and the psychiatrist of the program of Parma had been trained to collect research data on BUP and METH dose, administration frequency (daily in the outpatients center, or three times a week), measures of previous illicit drug use and problematic alcohol use, social status and employment condition, educational status, interpersonal relationships levels, criminal activities, health status, and possible DSM Axis I and Axis II comorbid diagnoses. Relevant data were requested, for the 6 months preceding the study, concerning substance abuse other than heroin, activities, and stressful events. Previous psychosocial treatment and previous residential treatment were also recorded on the form. 2.4. Personality assessment DSM-IV clinical evaluation and psychometric measures were performed by trained psychiatrists at baseline. Axis I and II disorders were evaluated using the Structured Clinical Interview (SCID) for Axis I disorders (Spitzer et al., 1990) (Italian version: Intervista Clinica Strutturata per il DSM-III-R, Fava et al., 1993) and the Structured Interview for DSM-IV Personality Disorders (SIDP) for Axis II disorders (Pfohl et al., 1989) (Italian version: Maggini et al., 1994). Personality was assessed with the MMPI 2 (Hathaway and McKinley, 1989). All METH and BUP patients completed the Symptom Check List 90 scale (SCL-90) for the evaluation of a broad range of psychological problems and symptoms of psychopathology. Primary symptom dimensions measured by SCL-90 included somatization, obsessive compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism (Derogatis, 1977). The patients repeated SCL-90 evaluation at week 4 and week 12. 2.5. Methadone and buprenorphine doses The patients included in the study were treated with METH average dose of 81.5 ± 35.4 mg, or BUP average dose of 9.2 ± 3.4 mg. The decision about doses was independent from the inclusion in the observational protocol. Stable doses were utilized during the first 12 weeks for both groups of patients, with minimal flexibility in relationship with patient requests. No missed doses and missed clinic visits were reported, both for METH and BUP, in the patients who remained in treatment. 2.6. Statistical analysis The variables were compared between treatment arms utilizing standard Chi-square tests. A survival analysis, on an intention-to-treat basis (Kaplan–Meier), was used to measure the efficacy of BUP and METH in term of retention. Positive urine samples for heroin were analyzed with a Chi-square test and ANOVA for repeated measures to evaluate the changes over time. SCL-90 psychometric measures were compared utilizing multiple ANOVA and t-test. Missing urine specimens were counted positive. The intention-to-treat sample (ITT-Analysis) was 78 in the METH and 76 in the BUP group (154 patients). 3. Results 3.1. Sample characteristics No significant differences in mean age (32 ± 3.8 years for BUP versus 33±5.3 years for METH), gender (males: 72.3% (55) for BUP versus 76.9% (60) for METH), daily heroin dose (2.1 ± 0.9 for BUP versus 2.3 ± 0.6 for METH), years of heroin addiction history (9.5 ± 2.8 years for BUP versus 10.7 ± 3.5 years for METH), interpersonal relationships quality, job performance, legal problems, alcohol problems and previous METH and residential treatment rates were evidenced between BUP and METH patients included in the study (Table 1). DSM-IV evaluation of the subjects revealed no comorbid diagnosis for 52.5% (41) of the subjects included in METH treatment and 53.8% (41) of the subjects included in BUP treatment. 3.2. Retention rate Survival analysis showed that the rate of BUP maintained patients who dropped out during the first four weeks were G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 41 Fig. 1. Surviving rates at the intention to treat analysis (Kaplan–Meier) in METH maintenance treatment group (MMT) and BUP maintenance treatment group (BMT). significantly higher, respect to the intention to treat sample, in comparison with METH maintained patients (Fig. 1). The risk for retention failure was similar between BUP and METH at week 12. Retention rates in BUP and METH groups at week 12 were respectively 59.2 and 61.5%, with no significant difference (45/76; 48/78) (Fig. 1). METH maintained patients who dropped out had significantly lower doses of METH than the completers (44 ± 4 versus 76 ± 12; F(d.f. = 1, 77) = 8.9, P < 0.01). No significant difference in doses was found between the intention-to-treat sample and the completers in the BUP group (8.8 ± 2.9 versus 9.4 ± 3.7). METH maintained patients who dropped out had significantly worse interpersonal relationships and employment status respect to completers (F(d.f. = 1, 77) = 4.12, P < 0.05; F(1, 77) = 8.6, P < 0.05). No significant difference in interpersonal relationships and employment status was found between the Intention-to-treat sample and the completers in the BUP group. No difference in term of comorbid depression rates was evidenced between the intention-to-treat sample and the completers in the methadone group. In contrast, response to buprenorphine treatment, in term of retention, was related to the existence of comorbid psychiatric disorders (Fig. 2a and b). Buprenorphine maintained patients who completed the observational period showed a significantly higher rate of depression than the patients who dropped out (31.1% versus 6.5%; χ(1) = 6.7, P < 0.01) and the Intention to treat sample (21.1%; χ(1) = 2.34, P < 0.05). No significant differences in age (32 ± 3.8 versus 31.2 ± 2.8 for BUP and 33 ± 5.3 versus 29.6 ± 3.4 for METH), gender (males 72,3% versus 73.3% for BUP; 76.9% versus 72.9% for METH), substance abuse history (years of addiction) (9.5 ± 2.8 versus 8.6 ± 3.6 for BUP and 10.7 ± 3.5 versus 11.3 ± 2.6 for METH), legal problems history (43.4% versus 46.67% for BUP; 44.9% versus 43.75% for METH), psychotropic medication associated to substitution treatment (23.7% versus 26.67% for BUP; 25.6% versus 22.9% for METH), previous methadone treatment (51.3% versus 48.88% for BUP; 59.00% versus 45.83% for METH) and residential treatment (38.2% versus 31.11% for BUP; 41.0% versus 31.25% Fig. 2. Surviving rates at the intention to treat analysis (KaplanMeier) in depressed and non depressed patients treated with BUP (a) (upper panel) and METH (b) (lower panel). for METH) were evidenced between the Intention-to-treat sample and the completers both in BUP and METH groups. 3.3. Psychiatric comorbidity The rates of patients with Axis I diagnosis in METH and BUP groups were 25.6% (20) and 23.7% (18), respectively and the rates of patients with Axis II diagnoses were 34.6% (27) and 35.4% (27), respectively. The rate of depressed individuals was 21.1% (16) among BUP patients and 17.9% (14) in the METH group. No significant baseline difference was evidenced in Axis I and Axis II diagnoses rates between BUP and METH groups. SCL-90 data were consistent with DSM diagnoses, with a close correspondence between SCL-90 scores and Axis I and personality disorders criteria. No significant differences in baseline SCL-90 and MMPI 2 scores have been demonstrated between BUP and METH groups. The rates of psychotropic medication associated to substitution treatment did not show any difference between BUP and METH groups. BUP maintained patients who dropped out had significantly lower SCL-90 “depression” subscale scores at baseline than the completers (1.2 ± 0.4 versus 2.3 ± 0.5, P < 0.005, t = 3.50, d.f. = 1). In contrast, BUP maintained patients who dropped out had significantly higher 42 G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 SCL-90 “hostility”, “obsessive compulsive”, “paranoid ideation”, and “psychoticism” subscales scores at baseline than the completers (2.2 ± 0.3 versus 1.4 ± 0.3, P < 0.005, t = 3.48, d.f. = 1; 1.9 ± 0.5 versus 1.0 ± 0.2, P < 0.05, t = 2.14, d.f. = 1; 2.6 ± 0.7 versus 1.2 ± 0.4, P < 0.01, t = 2.45, d.f. = 1; 1.5 ± 0.2 versus 0.9 ± 0.3, P < 0.05, t = 2.16, d.f. = 1, respectively). No significant difference in SCL-90 subscales scores were found between the Intention-to-treat sample and the completers in the METH group. The same was true for baseline MMPI 2 results that showed significantly higher depression (D) subscale scores in BUP patients who completed the 12 weeks treatment (MMPI 2 “D”: 58.87 ± 3.2 versus 45.4 ± 1.4, P < 0.005, t = 3.44, d.f. = 1), in comparison with the patients who dropped out earlier. No significant difference in MMPI 2 subscales scores were found between the intention-to-treat sample and the completers in the METH group. ANOVA for repeated measures showed a significant decrease in SCL-90 depression scores in both METH and BUP patients who completed the study (F = 7.4, d.f. = 2 P < 0.01; F = 15.6, d.f. = 2 P < 0.001), with a significantly more consistent decrease in BUP completers, in comparison with METH completers. ANOVA for repeated measures showed a significant effect of time (F = 19.6, d.f. = 2, P < 0.001), group (F = 8.6, d.f. = 1, P < 0.005) and group per time (F = 6.9, d.f. = 3, P < 0.05). 3.4. Urinalysis The risk for positive urine testing was similar between BUP and METH at week 4 and week 12, as expression of illicit drug use in general. Positive urines in general in BUP and METH groups at week 4 were 40.8 and 38.4%, and at week 12 44.7 and 46.2%, respectively, with no significant difference between groups. The rates of opioid positive urines (morphine metabolites) were not significantly different at week 4 between BUP (21.5%) and METH (24.4%) groups. In contrast, patients treated with BUP showed a significantly lower rate of positive urines for morphine metabolites (25.0%), as expression of heroin use, than those treated with METH (32.1%) at week 12, in the patients who remained in treatment. ANOVA for repeated measures showed a significant effect of time (F = 9.3, d.f. = 2, P < 0.01), group (F = 6.3, d.f. = 1, P < 0.05) and group per time (F = 6.4, d.f. = 3, P < 0.05) in opioid positive urine changes (Fig. 3). Both methadone and buprenorphine maintained patients who showed morphine positive urines, and continued illicit opioid use, had significantly lower doses than the patients with negative urines (88.4 ± 25.9 versus 48.1 ± 4.4; t = 5.3, P < 0.001, d.f. = 1) (7.7 ± 0.6 versus 11.3 ± 0.5 t = 2.53, P < 0.05, d.f. = 1). High doses of METH were more effective than low doses in reducing illicit opioid use (F = 12.4, P < 0.01). Similarly, high doses of BUP were more effective than low doses in reducing illicit opioid use (F = 9.7, P < 0.05). METH maintained patients who showed positive urines for morphine metabolites had significantly worse interpersonal relationships and employment status respect to the patients with negative urines (F(76) = 4.12, P < 0.05; F(76) = 8.6, P < 0.05). No significant difference in interpersonal relationships and employment status was found between the opioid-positive and the opioid-negative urines patients in the BUP group. No significant difference in term of comorbid depression rates was evidenced between the patients with negative urines and those with opioid positive urines in the METH group. In contrast, response to BUP treatment, in term of negative urines, was related to the existence of comorbid psychiatric disorders. Buprenorphine maintained patients who showed negative urines presented a significantly higher rate of depression than those with positive urines (26.3% versus 5.3%; χ(1) = 3.8, P < 0.05) (Table 2). No significant differences in age, gender, substance abuse history (years of addiction and heroin doses), legal problems history, psychotropic medication associated to substitution treatment and previous METH and residential treatment were evidenced between the negative urines patients and Fig. 3. Urinalyses positive for opioid drugs at week 4 and week 12 in patients treated with METH and BUP. G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 43 Table 2 Depression diagnosis rate in METH patients (%) Depression diagnosis rate in BUP patients (%) Opioid negative urines Opioid positive urines Significance 16.9 26.3 24.0 5.3 χ = 3.8, P < 0.05 the opioid-positive urines patients both in BUP and METH groups. BUP maintained patients who showed negative urines had significantly higher SCL-90 “depression” subscale and MMPI 2 depression (D) subscale scores at baseline than those with positive urines (SCL-90 1.9 ± 0.3 versus 0.80 ± 0.5, P < 0.005, t = 3.50, d.f. = 1) (MMPI 2 “D”: 58.87 ± 3.2 compared with 45.4 ± 1.4, P < 0.005, t = 3.44, d.f. = 1). Mean SCL-90 and MMPI 2 scores at week 1 were not found significantly different between METH patients who did not use heroin during treatment and those who continued to inject. METH maintained patients who showed positive urines for cocaine had significantly lower METH doses than those with negative urines (t(1) = 3.12, P < 0.05; t(1) = 3.25, P < 0.05). No significant difference in doses was found between the cocaine-positive and cocaine-negative urines patients in the BUP group. 4. Discussion The present study showed that BUP and METH were similar in term of retention in treatment at 12 weeks, but BUP was less effective to retain patients in the early phase. Our findings are in agreement with previous studies that evidenced no differences in retention measures between METH and BUP (West et al., 2000; Farre et al., 2002), but significantly higher retention rate in METH patients during the early phase of treatment (6 weeks) (Petitjean et al., 2001). The percentage of patients retained at 12 weeks was comparable with rates reported elsewhere for these medications (Johnson et al., 2000; Schottenfeld et al., 1997; Strain et al., 1994). In contrast, treatment retention better for METH was demonstrated by other authors, probably due to the low doses of BUP utilized in comparison with appropriate doses of METH (Kosten et al., 1993; Fischer et al., 1999a,b). Early drop out in BUP group patients in our study seems to be unrelated to dosage levels, that were not different in the subjects who let the treatment during the first weeks, respect to those who stayed, suggesting that other factors may have influenced retention. Accordingly, high dose BUP was found to suppress heroin use better than low doses, without influencing retention rate (Mattick et al., 2003). Nevertheless, BUP capacity to completely counteract heroin effects perception at high doses, evidenced in human laboratory studies (Comer et al., 2001), could have represented a fac- tor reducing compliance in the early phase of maintenance treatment. On the other side, higher retention in BUP treatment seems to be associated with depression and dysphoria, with a significant improvement of psychiatric symptoms in this subgroup of patients. The association between affective disorders and higher retention in BUP group was not unexpected. In a double blind investigation BUP induced strong antidepressant effects in patients with endogenous depression (Emrich et al., 1983) and in an open-label study, subjects with treatment-refractory, unipolar major depression showed clinical improvement in both subjective and objective measures of depression after BUP treatment (Bodkin et al., 1995). Our data are in contrast with Laqueille findings (Laqueille et al., 2001), suggesting that negative outcome of BUP treatment was related with depression. This discrepancy may be due to the difference in diagnostic methodologies, being Laqueille evidence supported by psychometric measures only, and not by clinical DSM evaluation. Better outcome in depressed patients may tentatively be attributable to the specific pharmacological profile of the drug, being BUP a partial -agonist/-antagonist: in fact, -receptors agonist, such as butorphanol and enadoline have been reported to increase dysphoria, confusion, sedation and to produce feelings of depersonalization in humans (Greenwald and Stitzer, 1998; Walsh et al., 2001), supporting the hypothesis that BUP may counteract in depressed subjects the emotional and perceptual effects of -receptors system. Accordingly, BUP capacity to control dysphoria, as a possible consequence of a dysfunction of the endogenous -opioid system, has been suggested also by combining BUP with naltrexone, theoretically leaving -antagonism as the major medication effect, and obtaining positive responses to treatment that exceeded those expected from naltrexone alone (Rothman et al., 2000). The significant reduction of SCL-90 depression-subscale scores obtained in our depressed subjects treated with BUP, and not in METH patients, again indicates a possible specific action of -agonist/-antagonist drug on affective symptoms and their relationship with addictive behavior. In agreement with these findings, depressive symptoms were reported to decrease significantly in the patients who were depressed at intake to BUP treatment (Kosten et al., 1990). Although BUP has been reported as a useful treatment for moderate dependence and more motivated subjects (Eder et al., 1998; Ling et al., 1994), the patients submitted to BUP who remained in treatment in the present observational 44 G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 study were not affected by less severe disorders, in term of addiction history (heroin dependence duration and doses), self-disruptive behavior, interpersonal relationships and social integration. In contrast, retention in METH patients was not related with specific comorbid diagnoses, but with social integration, good inter-personal relationships and job stability, as previously demonstrated in a recent multi-centric study including long-term MMT patients (Gerra et al., 2003). In the present study, BUP and METH obtained similar results, in term of illegal drugs use in general, but a significantly lower rate of opioid positive urines was found in BUP patients on week 12, apparently indicating a higher effectiveness of BUP in counteracting heroin injection, in comparison with METH. Similarly, an open-label, non-randomized study evidenced, at the first 8 weeks follow up, significantly less additional consumption of opioids in the BUP-maintained group, in comparison with the METH group (Giacomuzzi et al., 2003). Because of the limitations of this observational clinical study definite conclusions are not allowed: patients included in BUP and METH groups, without a random schedule, may have been influenced by their motivational status at the beginning of the study with different intention to abstain from illicit opioids. At the present evaluation, both BUP and METH groups showed that negative urines in general and negative urines for illicit opioid drugs corresponded to higher doses treatment, as repeatedly evidenced in previous trials (Johnson et al., 2000; Ling et al., 1996; Maxwell and Shinderman, 1999; Preston and Bigelow, 2000; Strain et al., 1999). Our data increase the evidence suggesting that BUP might be as effective as METH in the treatment of heroin dependence, with lower rates of illicit opiates consumption, particularly in subjects affected by depression and mood disorders. More consistent risk of discontinuing treatment in BUP patients and more positive urine analyses evidenced by other authors (Barnett et al., 2001), in comparison with METH patients, might be attributable to the different sample of patients, possibly including non-comparable subgroups of personality traits and comorbid disorders. Different rates of dually diagnosed patients in the other studies, that did not report detailed information concerning psychiatric symptoms, could have significantly influenced the outcome, with a higher rate of opioid-positive urinalyses in BUP patients respect to METH patients (Strain et al., 1994, 1996). Cocaine-positive urines appear unrelated to low doses in BUP patients, indicating, at least in clinical conditions, BUP inability to counteract cocaine use among heroin addicts, also at high doses. Accordingly, previous experimental evaluation of BUP capacity to reduce cocaine craving in humans did not evidence encouraging results (Foltin and Fischman, 1994; Kamien and Spealman, 1991). The lack of relationships between psychosocial functioning, substance abuse history and BUP treatment outcome suggests that addiction severity, and its social consequences, cannot be used per se as valuable predictors of BUP treatment effectiveness, in contrast with previous reports (Resnick et al., 1991; Pani et al., 2000)., indicating the need of further research to define predictor variables of BUP outcome. Our findings need to be interpreted with caution because of the methodological limitations of the survey: in fact, the study used a descriptive approach, with short-term measurements, non-standard doses, in a naturalistic clinical setting, and non-random procedure that do not permit certain conclusions on BUP and METH effectiveness. In conclusion, METH seems to obtain higher retention in the early phase of treatment, with an effective action in maintaining the relationship with the patient at the beginning of the program, and worse results in term of opioid-positive urines, in comparison with BUP. BUP effectiveness was higher, both in term of retention and negative urinalyses, in depressed subjects. Continued research is needed to better investigate the possible psychobiological traits characterizing addicted individuals with better responses to BUP treatment, not necessarily associated to addiction severity and psychosocial functioning. Acknowledgements The study was supported by internal funds of Addiction Research Center of Parma (Local Public Health Unit, AUSL, Emilia-Romagna Region). No private companies were included among the sources of financial support for the present study. References Barnett, P.G., Rodgers, J.H., Bloch, D.A., 2001. A meta-analysis comparing buprenorphine to METH for treatment of opiate dependence. Addiction 96 (5), 683–690. Bodkin, J.A., Zornberg, G.L., Lukas, S.E., Cole, J.O., 1995. Buprenorphine treatment of refractory depression. J. Clin. Psychopharmacol. 15 (1), 49–57. Comer, S.D., Collins, E.D., Fischman, M.W., 2001. Buprenorphine sublingual tablets: effects on IV heroin self-administration by humans. Psychopharmacology (Berl.) 154 (1), 28–37. Derogatis, L.R., 1977. SCL-90-R: administration, scoring and procedures: manual 1. Clinical Psychometric Research, Baltimore, MD. Eder, H., Fischer, G., Gombas, W., Jagsch, R., Stuhlinger, G., Kasper, S., 1998. Comparison of buprenorphine and METH maintenance in opiate addicts. Eur. Addict. Res. 4 (Suppl 1), 3–7. Emrich, H.M., Gunther, R., Dose, M., 1983. Current perspectives in the pharmacopsychiatry of depression and mania. Neuropharmacology 22 (3 Spec No), 385–388. Farre, M., Mas, A., Torrens, M., Moreno, V., Cami, J., 2002. Retention rate and illicit opioid use during METH maintenance interventions: a meta-analysis. Drug Alcohol. Depend. 65 (3), 283–290. Fava, M., Guaraldi, G.B., Mazzi, F., Rigatelli, M., 1993. Intervista Clinica Strutturata per il DSM-III-R. Organizzazioni Speciali, Florence. Fischer, G., Gombas, W., Eder, H., Jagsch, R., Peternell, A., Stuhlinger, G., Pezawas, L., Aschauer, H.N., Kasper, S., 1999a. Buprenorphine versus METH maintenance for the treatment of opioid dependence. Addiction 94 (9), 1337–1347. G. Gerra et al. / Drug and Alcohol Dependence 75 (2004) 37–45 Fischer, G., Gombas, W., Eder, H., Jagsch, R., Stuhlinger, G., Aschauer, H.N., Kasper, S., 1999b. Buprenorphine vs. METH as maintenance treatment for opioid dependence. Nervenarzt 70 (9), 795–802. Foltin, R.W., Fischman, M.W., 1994. Effects of buprenorphine on the self-administration of cocaine by humans. Behav. Pharmacol. 5 (1), 79–89. Gerra, G., Ferri, M., Polidori, E., Santoro, G., Zaimovic, A., Sternieri, E., 2003. Long-term methadone maintenance effectiveness: psychosocial and pharmacological variables. J. Subst. Abuse Treat. 25 (1), 1– 8. Giacomuzzi, S.M., Riemer, Y., Ertl, M., Kemmler, G., Rossler, H., Hinterhuber, H., Kurz, M., 2003. Buprenorphine versus methadone maintenance treatment in an ambulant setting: a health-related quality of life assessment. Addiction 98 (5), 693–702. Greenwald, M.K., Stitzer, M.L., 1998. Butorphanol agonist effects and acute physical dependence in opioid abusers: comparison with morphine. Drug Alcohol. Depend. 53 (1), 17–30. Hathaway, S.R., McKinley, J.C., 1989. Minnesota Multifasic Personality Inventory-2. Manual, University of Minnesota Minneapolis. Johnson, R.E., Chutuape, M.A., Strain, E.C., Walsh, S.L., Stitzer, M.L., Bigelow, G.E., 2000. A comparison of levomethadyl acetate, buprenorphine, and METH for opioid dependence. N. Engl. J. Med. 343 (18), 1290–1297. Kamien, J.B., Spealman, R.D., 1991. Modulation of the discriminativestimulus effects of cocaine by buprenorphine. Behav. Pharmacol. 2 (6), 517–520. Kosten, T.R., Morgan, C., Kosten, T.A., 1990. Depressive symptoms during buprenorphine treatment of opioid abusers. J. Subst. Abuse Treat. 7 (1), 51–54. Kosten, T.R., Schottenfeld, R., Ziedonis, D., Falcioni, J., 1993. Buprenorphine versus METH maintenance for opioid dependence. J. Nerv. Ment. Dis. 181 (6), 358–364. Laqueille, X., Poirier, M.F., Jalfre, V., Bourdel, M.C., Willard, D., Olie, J.P., 2001. Predictive factors of response to buprenorphine in the substitutive treatment of heroin addicts. Results of a multicenter study of 73 patients. Presse Med. 30 (32), 1581–1585. Ling, W., Rawson, R.A., Compton, M.A., 1994. Substitution pharmacotherapies for opioid addiction: from METH to LAAM and buprenorphine. J. Psychoactive Drugs 26 (2), 119–128. Ling, W., Wesson, D.R., Charuvastra, C., Klett, C.J., 1996. A controlled trial comparing buprenorphine and METH maintenance in opioid dependence. Arch. Gen. Psychiatry 53 (5), 401–407. Mattick, R.P., Kimber, J., Breen, C., Davoli, M., 2003. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst. Rev. (2), CD002207. Maxwell, S., Shinderman, M., 1999. Optimizing response to methadone maintenance treatment: use of higher-dose methadone. J. Psychoactive Drugs 31 (2), 95–102. Pani, P.P., Maremmani, I., Pirastu, R., Tagliamonte, A., Gessa, G.L., 2000. Buprenorphine: a controlled clinical trial in the treatment of opioid dependence. Drug Alcohol. Depend. 60 (1), 39–50. 45 Petitjean, S., Stohler, R., Deglon, J.J., Livoti, S., Waldvogel, D., Uehlinger, C., Ladewig, D., 2001. Double-blind randomized trial of buprenorphine and METH in opiate dependence. Drug Alcohol. Depend. 62 (1), 97– 104. Pfohl, B., Blum, N., Zimmerman, M., Stangl, D., 1989. Structured Interview for Personality Disorders, revised version. University of Iowa, Iowa City, IA. Preston, K.L., Bigelow, G.E., 2000. Effects of agonist-antagonist opioids in humans trained in a hydromorphone/not hydromorphone discrimination. J. Pharmacol. Exp. Ther. 295 (1), 114–124. Raisch, D.W., Fye, C.L., Boardman, K.D., Sather, M.R., 2002. Opioid dependence treatment, including buprenorphine/naloxone. Ann. Pharmacother. 36 (2), 312–321. Resnick, R.B., Resnick, E., Galanter, M., 1991. Buprenorphine responders: a diagnostic subgroup of heroin addicts? Prog. Neuropsychopharmacol. Biol. Psychiatry 15 (4), 531–538. Rothman, R.B., Gorelick, D.A., Heishman, S.J., Eichmiller, P.R., Hill, B.H., Norbeck, J., Liberto, J.G., 2000. An open-label study of a functional opioid kappa antagonist in the treatment of opioid dependence. J. Subst. Abuse Treat. 18 (3), 277–281. Schottenfeld, R.S., Pakes, J.R., Kosten, T.R., 1998. Prognostic factors in Buprenorphine- versus METH-maintained patients. J. Nerv. Ment. Dis. 186 (1), 35–43. Schottenfeld, R.S., Pakes, J.R., Oliveto, A., Ziedonis, D., Kosten, T.R., 1997. Buprenorphine versus methadone maintenance treatment for concurrent opioid dependence and cocaine abuse. Arch. Gen. Psychiatry 54 (8), 713–720. Spitzer, R.L., Williams, J.B.W., Gibbon, M., First, M.B., 1990. Structured Clinical Interview according to DSM-III-R. American Psychiatric Press, Washington, DC and London, England. Strain, E.C., Stitzer, M.L., Liebson, I.A., Bigelow, G.E., 1994. Comparison of buprenorphine and METH in the treatment of opioid dependence. Am. J. Psychiatry 151 (7), 1025–1030. Strain, E.C., Stitzer, M.L., Liebson, I.A., Bigelow, G.E., 1996. Buprenorphine versus METH in the treatment of opioid dependence: selfreports, urinalysis, and addiction severity index. J. Clin. Psychopharmacol. 16 (1), 58–67. Strain, E.C., Bigelow, G.E., Liebson, I.A., Stitzer, M.L., 1999. Moderateversus high-dose methadone in the treatment of opioid dependence: a randomized trial. JAMA 281 (11), 1000–1005. Uehlinger, C., Deglon, J., Livoti, S., Petitjean, S., Waldvogel, D., Ladewig, D., 1998. Comparison of buprenorphine and methadone in the treatment of opioid dependence. Swiss multicentre study. Eur. Addict. Res. 4 (Suppl. 1), 13–18. Walsh, S.L., Strain, E.C., Abreu, M.E., Bigelow, G.E., 2001. Enadoline, a selective kappa opioid agonist: comparison with butorphanol and hydromorphone in humans. Psychopharmacology (Berl.) 157 (2), 151– 162. West, S.L., O’Neal, K.K., Graham, C.W., 2000. A meta-analysis comparing the effectiveness of buprenorphine and METH. J. Subst. Abuse 12 (4), 405–414.