Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
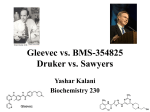
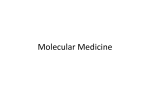
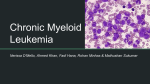
REUTERS / Jagadeesh N. V. Spotlight On... Chronic Myeloid Leukemia A PHARMA MATTERS REPORT. A REVIEW OF JANUARY-MARCH 2012. PUBLISHED APRIL 2012. Expert therapy area review of the key market players and deals highlights for leading areas of industry investment and development. These insightful reviews are based on the strategic data and insights from Thomson Reuters Cortellis™. ABSTRACT With the advent of targeted therapy, chronic myeloid leukemia (CML) has undergone a major transformation from a terminal disease to an essentially manageable chronic condition. Despite significantly improved survival rates, there still remains room for improvement in efficacy, tolerability, and resistance potential. Though the tyrosine kinase inhibitor Gleevec is regarded as the poster child for rational drug design, more efficacious secondgeneration agents are starting to gain acceptance in first-line use; however, in the absence of mature survival data, their longterm benefit over Gleevec remains to be seen. As patients remain on therapy for increasing periods of time, management of toxicity and cost are likely to be significant drivers of treatment choice. The CML pipeline is primarily focused on therapies to overcome resistance, which is particularly problematic following failure of first-line agents and an unmet need still exists for third-line options. For patients responding well to treatment with tyrosine kinase inhibitors, the ultimate question is whether such therapy can lead to a cure. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA SECTION I INTRODUCTION Chronic myeloid leukemia, also known as chronic myelogenous leukemia (CML), is an acquired clonal myeloproliferative disorder of the hematopoietic stem cell, accounting for 15 percent of all leukemias and 20 percent of adult leukemias. Although observed in all age groups, CML is typically a disease of later life, with a median age of onset of 67 years. Unlike most other cancers, CML is associated with a single oncogene product that is critical to the pathology of the disease. The vast majority of CML cases are caused by a reciprocal translocation between chromosomes 9 and 22 resulting in the formation of the Philadelphia (Ph) chromosome, which is consequently used in the cytogenetic diagnosis of CML. CML is believed to develop when a single pluripotent hematopoietic stem cell acquires a Ph chromosome; the Ph chromosome confers a survival advantage to the cell and the Phpositive lineage eventually displaces normal hematopoietic cells, leading to a loss of hematopoietic function. The Ph chromosome contains an oncogene consisting of the breakpoint cluster region (BCR) gene and the Abelson murine leukemia (ABL) gene. The product of the BCR-ABL fusion gene is the p210BCR-ABL tyrosine kinase, which contains the N-terminal domain of BCR and the C-terminal domain of ABL. The chimeric protein is constitutively active and has elevated kinase activity compared with the normal ABL protein. The tyrosine kinase activity of the p210BCR-ABL protein is associated with increased proliferation and decreased apoptotic responses, leading to overproduction of myeloid cells and premature release of undifferentiated myeloid cells into the circulation. DNA repair is also dysregulated, which leads to genetic instability associated with disease progression. CML is a triphasic disease, typically progressing from a chronic phase through a transient accelerated phase to the rapidly fatal blast crisis or blastic phase. The chronic phase is characterized by the overproduction of myeloid cells that retain their ability to differentiate and function normally. If untreated, chronic-phase CML generally progresses to advanced disease in approximately three to five years. Disease progression is associated with clonal evolution due to the accumulation of additional chromosomal abnormalities that decrease the ability of the leukemic cells to differentiate. The blastic phase resembles an acute leukemia, and is typified by poor prognosis and a survival time of only 3 to 6 months due to the rapid accumulation of undifferentiated blast cells. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA CML THERAPY: FROM THE DARK AGES TO THE GLEEVEC ERA Currently, the only curative treatment option for CML is an allogeneic hematopoietic stem cell transplant (HSCT); however, this procedure is not feasible for the majority of CML patients. Issues include age, lack of a suitable donor, and the morbidity and mortality associated with the procedure and its associated complications such as opportunistic infections and graft-versushost disease. Since HSCT carries a mortality rate of 15 to 40 percent, non-curative options are more frequently utilized to delay disease progression from the chronic to the blastic phase. CML was historically treated with cytotoxic chemotherapeutic agents such as busulfan and hydroxyurea, which controlled clinical manifestations of the disease but did not eliminate the Ph-positive malignant cells. The introduction of interferon (IFN)-alfa significantly improved survival and resulted in durable cytogenetic responses in 10 to 30 percent of patients, but at the cost of significant toxicity. Nevertheless, IFN-alfa was formerly regarded as the treatment of choice for CML. Further improvements in response were observed with the combination of IFN-alfa and chemotherapy, but side effects remained problematic. Historically, the survival time from diagnosis was just five years. GLEEVEC: AN ARCHETYPE OF RATIONAL DRUG DESIGN The BCR-ABL fusion gene was the first genetic abnormality to be associated with a specific malignancy and enabled the development of the BCR-ABL tyrosine kinase inhibitor (TKI) Gleevec/Glivec (imatinib) by Novartis. Due to its targeted mechanism of action, Gleevec has a negligible effect on other cellular tyrosine kinases and consequently fewer side effects compared with more traditional, non-targeted cytotoxic oncology drugs. The success of Gleevec is considered a huge victory for rational drug discovery. In the US, Gleevec received accelerated approval in May 2001 for the treatment of CML patients in any phase of the disease who had failed to respond to IFN-alfa therapy, based on the unprecedented improvements in response observed in phase II studies. The drug’s label was expanded soon after in December 2002 to allow first-line use, also under the accelerated approval process. Gleevec was a huge success for Novartis as a result of its impressive activity and favorable tolerability, achieving sales in excess of $1 billion by its third year of launch (see FIGURE 1). PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA Gleevec SALES IN US $ MILLIONS 5000 4000 3000 2000 1000 0 11 20 10 20 09 20 08 20 07 20 06 20 05 20 04 20 03 20 02 20 01 20 00 20 YEAR Figure 1: gleevec sales Figures 2000 to 2011 (Data are DeriveD From Thomson ReuTeRs CoRTellis foR CompeTiTive inTelligenCe) The approval of Gleevec has been hailed as a defining moment for translational research; the drug has revolutionized CML by transforming a fatal cancer into a chronic, often manageable disease. With the advent of Gleevec, patients with chronic-phase CML can now hope to remain symptom-free for at least 10 years and may enjoy a normal lifespan. Median survival from diagnosis can reach 30 years, with some patients never progressing to the blastic phase. Life-long use of Gleevec is supported by long-term follow-up data from the IRIS study, which have demonstrated high durable response rates in Gleevec-treated patients. At eight years follow-up, the event-free, progression-free, and overall survival rates were estimated to be 81, 92, and 85 percent, respectively, for Gleevec-treated patients. The improved survival of CML patients as a result of therapeutic advances has led to improved methods of evaluating treatment success and failure. Response to therapy is assessed by hematologic, cytogenetic, and molecular responses, which correlate to increasing depths of response to treatment. The initial treatment milestone is a complete hematologic response, or normalization of blood cell counts, which is expected to occur 3 months after initiation of treatment and is associated with resolution of CML symptoms. The next therapeutic goal is to achieve a major cytogenetic response (MCyR; </= 35 percent Ph+ metaphases in the bone marrow or blood) by 12 months and a complete cytogenetic response (CCyR; no detectable Ph+ metaphases) by 18 months. Currently, the ultimate treatment aim is to achieve a major molecular response (MMR) or a complete molecular response (CMR), defined as a 3-log reduction in BCR-ABL transcripts and no detectable BCR-ABL transcripts, respectively, usually assessed by quantitative or nested PCR. Achieving the milestone of MMR after 12 months of therapy is associated with a very low risk of disease relapse. With the success of TKI therapy, the next conundrums to be addressed are whether a durable CMR can be considered the equivalent of a cure, and whether discontinuation of therapy is a viable option for patients achieving long-lasting molecular responses. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA LIMITATIONS OF GLEEVEC Despite the unparalleled improvements in response observed with Gleevec, the IRIS study has its limitations. In particular, questions have arisen over the high level of patient discontinuation and the censoring of data in cases of study discontinuation. Because only 55 percent of patients remained on Gleevec at the eight year follow-up, it is possible that the survival rates have been overestimated. Indeed, it has been suggested that if the calculation of event-free survival includes patients who discontinued treatment due to toxicity or inadequate cytogenetic response, the five-year event-free survival rate drops from 83 percent to 62.7 percent. With the development of a highly specific, single-target therapy for CML, it is perhaps unsurprising that drug resistance has emerged as a significant threat to continued treatment success. Resistance to Gleevec has been documented in 20 to 30 percent of patients and can be categorized as either primary or secondary. Primary hematologic resistance, defined as a failure to achieve hematologic remission within 3 to 6 months of Gleevec initiation, is relatively rare in newly diagnosed patients in chronic phase, occurring in approximately 2 percent of patients. However, primary cytogenetic resistance, defined as a failure to achieve any form of cytogenetic response at 6 months, MCyR at 12 months or CCyR at 18 months, is somewhat more common, documented in 15 to 25 percent of patients. Although the precise etiology of primary resistance has not been fully characterized, over-expression of multidrug resistance protein 1 and low expression of human organic cation transporter 1 (hOCT1) have been associated with suboptimal responses to Gleevec. Although not routinely assessed at the time of diagnosis, it has been suggested that hOCT1 may be useful as a prognostic indicator of treatment response, as pretreatment levels have been shown to be the most powerful predictor of response to Gleevec therapy. Studies have demonstrated that high pretreatment hOCT1 expression is associated with significantly superior survival outcomes. Secondary (or acquired) resistance is defined by a loss of response in patients previously responding to therapy and is associated with progression to blastic-phase disease. The most frequent cause of resistance is point mutations in the ABL kinase domain of the BCR-ABL fusion protein. Gleevec interacts with the ATP-binding site of the ABL kinase domain in the inactive, closed confirmation, preventing a conformational change to the active form of the enzyme. This rigid structural requirement for entry and binding means that a single amino acid substitution can confer resistance to Gleevec by disrupting the binding of the drug to the active site. The T315I mutation in the ABL kinase domain confers the highest resistance to Gleevec and has been associated with a poor prognosis, particularly in more advanced stages of the disease. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA Other mechanisms of secondary resistance have also been documented and include over-expression and gene amplification of BCR-ABL. Resistance is believed to be multifactorial, as data from the START-C study demonstrated that 46 percent of patients with Gleevec-resistant chronic-phase CML did not carry BCR-ABL mutations. It has been postulated that the true burden of Gleevec resistance may be underestimated. Direct comparisons of the resistance rates observed in clinical studies are difficult due to the different definitions of treatment failure used across the studies. In addition, the continued participation of only 55 percent of the original IRIS cohort and the high level of data censoring may compound the issue. Patient adherence to therapy has been highlighted as critical to the development of resistance to Gleevec. It is well recognized that lack of adherence is a major problem associated with longterm oral therapy for chronic diseases; non-adherence to Gleevec has been well documented and has a significant impact on treatment efficacy. Studies have shown that poor adherence is the most important factor contributing to treatment failure and cytogenetic relapse. Appropriate management of side effects, close monitoring and patient education may help to improve adherence and consequently prevent or delay the development of resistance. It is estimated that 5 to 10 percent of patients will discontinue Gleevec due to side effects. As patients remain on therapy for increasingly extended periods of time, management of side effects becomes critical to maintaining adherence, as well as patient quality of life and disease remission. THE SECOND GENERATION OF TKIS: TASIGNA AND SPRYCEL Although Gleevec is still considered a revolutionary therapy, resistance has necessitated the development of new therapies to provide treatment options for patients who fail to respond. Understanding the mechanisms of resistance to Gleevec has aided development of the rationally-designed second-generation TKIs Sprycel (dasatinib) and Tasigna (nilotinib). Bristol-Myers Squibb’s (BMS) Sprycel is a dual SRC/BCR-ABL kinase inhibitor, first approved for second-line use in 2006 and subsequently granted first-line approval in 2010. In contrast to Gleevec and Tasigna, Sprycel binds to both the active and inactive forms of BCR-ABL and demonstrates enhanced efficacy compared with Gleevec due to recognition of multiple forms of the protein and a greater binding affinity. Sprycel has in vitro activity against almost all Gleevec-resistant BCR-ABL mutations; however, it is ineffective in disease with the T315I mutation. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA “These drugs have dramatically changed the lives of patients with Cml.” Richard Pazdur, MD, Director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research Novartis’s BCR-ABL kinase inhibitor Tasigna was developed by modification of Gleevec, resulting in a drug that displays higher affinity for the inactive form of BCR-ABL and demonstrates greater efficacy than the parent compound. Tasigna was approved for second-line use in 2007 and first-line use in 2010. Similar to Sprycel, Tasigna has no efficacy against leukemic cells with the T315I mutation. WHICH TKI FOR FIRST-LINE THERAPY? With three TKIs approved for the first-line treatment of chronicphase CML, physicians now have a choice of therapies that can be selected according to their patients’ needs. Both Sprycel and Tasigna have demonstrated good efficacy in the first-line setting and so treatment choice will depend on physician familiarity, disease risk score, patient age, presence of comorbid conditions and the patient’s ability to tolerate therapy. Head-to-head studies of the second-generation TKIs will be crucial in determining the most appropriate therapy for first-line use. Further investigation on surrogate endpoints as predictors of survival will also be useful to determine if the higher rate of molecular responses observed with the second-generation TKIs confer prolonged survival over Gleevec. Although both second-generation TKIs have been associated with significantly higher rates of CCyR and MMR than Gleevec, the ENESTnd and DASISION studies have not yet demonstrated significant improvements in progression-free and overall survival. A summary of two-year data from the ENESTnd and DASISION studies is shown in Table 1. TRIAL FOLLOW UP (MONTHS) ENESTnd DASISION 24 24 Tasigna 300 mg bid Tasigna 400 mg bid Gleevec 400 mg qd Sprycel 100 mg qd CCyR (%) 87 MMR (%) 71 85 77 86 82 67 44 64 46 CMR (%) 26 21 10 NA NA Progression-free survival (%) 98.0 97.7 95.2 93.7 92.1 Overall survival (%) 97.4 97.8 96.3 95.3 95.2 25 22 32 19 20 Dosing Discontinued treatment (%) Gleevec 400 mg qd NA: not available table 1: comparison oF First-line tKis Further follow-up data from ENESTnd have shown that both MMR and CMR4.5 (CMR at a sensitivity of ≥ 4.5 log reduction in BCR-ABL transcripts) were significantly higher for both doses of Tasigna compared with Gleevec at three years, and significantly PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA fewer Tasigna-treated patients progressed to accelerated or blastic phase. Although there was still no significant difference in overall survival between the treatment groups at three years follow-up (95.1, 97 and 94 percent for 300 mg Tasigna, 400 mg Tasigna and Gleevec, respectively), significantly fewer Tasigna-treated patients died following disease progression to accelerated or blastic phase. The significant benefit of Tasigna in terms of delaying disease progression could boost the drug’s first-line prospects, as such a benefit has not yet been observed for Sprycel. Stratification of patients by risk group could lead to preferential prescription of second-generation TKIs over Gleevec in higherrisk patient groups, as Tasigna and Sprycel have been associated with lower rates of progression in intermediate- and highrisk patients. The National Comprehensive Cancer Network’s guidelines recommend determination of risk status as part of the initial evaluation of CML patients. The patient’s mutational status may also influence the choice of drug: Tasigna is recommended for patients with V299L, T315A, or F317L/V/I/C mutations, whereas Sprycel is indicated for patients with Y253H, E255K/V, or F359V/C/I mutations. Due to Sprycel’s potential to cause pleural effusion, Tasigna may be more suitable in patients at risk of this complication, whereas Sprycel may be a more appropriate choice for patients with a history of pancreatitis or hyperglycemia. Pleural effusion is a common side effect of Sprycel therapy, with one recent analysis of phase I and II studies documenting its occurrence in 29 percent of chronic-phase, 50 percent of accelerated-phase and 33 percent of blastic-phase patients. Dose interruptions and reductions were required in the majority of patients receiving Sprycel in these studies (83 and 71 percent of patients, respectively). Additionally, the high cost associated with management of pleural effusion may influence the choice of therapy. Tolerability and patient convenience are significant drivers of therapy choice for diseases that require long-term therapy. Tasigna’s twice-daily dosing and fasting requirements make the drug less convenient compared with once-daily Gleevec and Sprycel, and may negatively impact patient adherence. As adherence is critical to achieving an optimal response to therapy, dosing convenience is an important consideration. However, while Sprycel can be administered once-daily with or without food, it is generally not as well tolerated as Tasigna. Healthrelated quality of life data is also notably lacking and will be useful for therapy selection. Cost-effectiveness is also a major consideration in TKI selection in the absence of a clear frontrunner in terms of efficacy. One analysis demonstrated that Tasigna-treated patients had greater adherence to therapy and incurred lower healthcare costs compared with Sprycel-treated patients. Despite the higher rate of molecular responses with second-generation TKIs, in the absence of a proven survival benefit, these newer, more PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA expensive medications are unlikely to be recommended for reimbursement if clear patient benefit over the cheaper Gleevec cannot be demonstrated. It is likely that long-term survival data will be required before widespread adoption of secondgeneration TKIs as first-line drugs of choice. As chronic-phase CML patients are likely to remain on their firstline therapy for many years, the first-line setting represents the biggest market opportunity in the CML arena. In the absence of mature survival data and head-to-head studies, much effort has been made by Tasigna and Sprycel’s respective marketeers to position their drugs as the therapy of choice over Gleevec in the first-line setting. Novartis’s presence in the hematology market with Gleevec may confer a competitive advantage to Tasigna. In addition to Novartis’s experience in CML, Tasigna appears to be associated with superior cost-effectiveness; consequently, Sprycel could see comparatively limited use in the first-line setting. Indeed, according to Consensus data from Thomson Reuters Cortellis™ for Competitive Intelligence, Tasigna is expected to edge out Sprycel, with predicted sales of $2.383 billion and $1.600 billion for the two respective agents in 2016 (see FIGURE 2). 2011 2016 Gleevec Tasigna Sprycel 0 1000 2000 3000 4000 5000 SALES IN US $ MILLIONS Figure 2: 2011 versus 2016 sales For gleevec, tasigna, anD sprycel (Data are DeriveD From Thomson ReuTeRs CoRTellis foR CompeTiTive inTelligenCe) For either second-generation drug to maintain a stronghold they will need to cement their front-line position before Gleevec goes offpatent in 2015, as the looming impact of generic Gleevec is likely to significantly change the dynamics of the first-line CML market. GENERIC GLEEVEC: IMPACT ON MARKET DYNAMICS The arrival of generic Gleevec in the US in 2015 has the potential to significantly change the CML treatment paradigm. Pressure from reimbursers may trigger a resurgence in first-line use of imatinib due to the need to reduce healthcare costs, a point of particular relevance in the CML market where branded drugs command premium prices and treatment may last decades. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA Gleevec’s favorable long-term safety and efficacy data may also drive the use of generics over Sprycel and Tasigna, which are not expected to gain traditional FDA approval for first-line use until at least 2015 when survival data is more mature. Generic Gleevec may also lead to more significant changes in treatment regimens for chronic-phase CML. Balancing the higher efficacy of the second-generation TKIs with the lower price of generics could lead to short-term “induction” use of Tasigna or Sprycel, followed by long-term “maintenance” therapy with generic imatinib. generic gleevec may significantly change the cml treatment paradigm. SECOND-LINE THERAPY AND BEYOND Whilst Sprycel appears to lose out to Tasigna as the secondgeneration TKI of choice for first-line treatment, it may come into its own as a preferred second-line agent. Sprycel has better efficacy than Tasigna in Gleevec-resistant CML, and, unlike Tasigna, is approved for use in Gleevec-resistant CML patients in the blastic phase. As CML progresses, the main therapeutic considerations shift from those of a chronic disease to an acute one. CML must be treated aggressively once a patient fails first-line therapy, and consequently tolerability becomes a less important concern. Additional therapies are still needed for patients failing on the first- and second-generation TKIs, as the duration of response to third-line agents is typically only 3 to 20 months. Many compounds are in development for the treatment of resistant CML, particularly for T315I mutations where there is a high unmet medical need. A comparison of pipeline Consensus forecast data from Cortellis for Competitive Intelligence is shown in Figure 3. Pfizer is developing bosutinib, a second-generation, dual SRC/ BCR-ABL kinase inhibitor that binds to an intermediate form of BCR-ABL. The drug is currently under review by the FDA and EMA for use in previously treated CML patients. Bosutinib is unlikely to see utilization in the first-line, following disappointing results from the BELA head-to-head study with Gleevec in newly diagnosed patients. While achievement of a CCyR was more rapid in bosutinib-treated patients than Gleevec-treated patients, no significant difference was observed in the CCyR rate between the two treatment groups and a higher rate of adverse events was documented in the bosutinib arm. It has been suggested that the failure of bosutinib to show superiority over Gleevec may be due to dose interruptions for diarrhea, which could have been managed with better supportive care. Nevertheless, tolerability is a major patient concern with first-line therapy, and the high rate of adverse events observed with bosutinib may hamper the drug’s prospects in newly diagnosed patients. As toxicity is less of a concern with subsequent lines of therapy, bosutinib may find its niche as a second- or third-line treatment, although its lack of activity against the T315I mutant may restrict its use in refractory CML patients. Consensus estimates from Cortellis for Competitive Intelligence appear relatively conservative, with the drug predicted to take sales of $140.0 million in 2016. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA The dual SRC/pan-BCR-ABL kinase inhibitor ponatinib (ARIAD Pharmaceuticals) is currently in phase III development and is predicted to be filed in the US and Europe later this year. The pivotal phase II PACE study is assessing the efficacy of ponatinib in Sprycel- or Tasigna- refractory CML patients and is expected to form the basis of the submission. Interim data certainly appear promising: 47 percent of the heavily pretreated patients achieved an MCyR, with 39 percent achieving a CCyR. Importantly, an MCyR was observed in 57 percent of patients with the T315I mutation, with CCyRs in 58 percent and MMRs in 33 percent of patients. As no effective treatment is currently available for patients with the T315I mutation, immediate adoption of ponatinib is predicted due to the high unmet need in this patient population. ARIAD is also planning a trial in newly diagnosed CML patients to compare ponatinib with Gleevec; however, ponatinib will have to compete with well-established first-line therapies in this space, and longterm safety and efficacy data will be required before adoption for first-line use. According to Consensus data from Cortellis for Competitive Intelligence, ponatinib is the clear winner among the investigational CML therapies in late-stage development, with predicted 2016 sales of $570.3 million. Other kinase inhibitors with activity against T315I-mutated ABL kinases are in earlier stages of development, and include danusertib and AT-9283. It has also been suggested that switch pocket kinase inhibitors such as DCC-2036 may show promise for the treatment of refractory CML. Looking beyond kinase inhibitors, omacetaxine mepesuccinate is a cytotoxic alkaloid derived from the evergreen tree Cephalotaxus harringtonia, which is being developed by Teva Pharmaceutical Industries (formerly Cephalon) for the potential treatment of refractory CML. Hematologic and cytogenetic responses have been observed in the CML-202 study in patients with the T315I mutation who had failed Gleevec, and in the CML-203 study in patients intolerant or resistant to two TKIs. Although previously under review in the US and Europe for Gleevec-resistant, T315I-mutated CML, a Complete Response letter from the FDA prompted ChemGenex (subsequently acquired by Cephalon) to withdraw the European filing. Teva now plans to resubmit applications for use in patients who have failed two or more TKIs. Although the planned filings encompass a larger patient population than previously targeted, regulatory setbacks and the product’s inconvenient subcutaneous dosing have resulted in relatively low near-term expectations for omacetaxine; Consensus data from Cortellis for Competitive Intelligence predict 2015 sales of just $75.0 million (see FIGURE 3). PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA Bosutinib Ponatinib Omacetaxine SALES IN US $ MILLIONS 600 480 360 240 120 0 16 20 5 1 20 4 1 20 3 1 20 2 1 20 1 1 20 16 20 5 1 20 4 1 20 3 1 20 2 1 20 1 1 20 16 20 5 1 20 4 1 20 3 1 20 2 1 20 1 1 20 YEAR Figure 3: 2011 versus 2016 For bosutinib, ponatinib anD omacetaXine (Data are DeriveD From Thomson ReuTeRs CoRTellis foR CompeTiTive inTelligenCe) WHAT NExT FOR GLEEVEC? As the CML TKI market becomes more competitive, efforts are being made to further drive Gleevec use in both the firstand second-line. As residual molecular disease is observed in most patients treated with 400 mg Gleevec, the benefit of higher starting doses in newly diagnosed patients has been investigated. The single-arm RIGHT study demonstrated favorable cytogenetic and molecular responses for 800 mg Gleevec compared with historical 400 mg data from the IRIS study. However, the randomized TOPS study designed to evaluate the two doses head-to-head failed to show a significant benefit in MMR for the higher dose, and the trial was terminated early. The higher dose was also associated with higher rates of dose interruption, reduction or discontinuation due to grade 3 or 4 adverse events. Consequently, it is likely that high-dose Gleevec will have a limited role in first-line therapy. Dose-escalation is an option for patients with cytogenetic relapse who have previously achieved a cytogenetic response with standard-dose Gleevec, and is allowed for within the drug’s label. However, the UK’s National Institute for Health and Clinical Excellence recently found high-dose Gleevec therapy is not costeffective due to the higher treatment costs and lower efficacy compared with other regimens in Gleevec-resistant chronic-phase CML patients. Dose-escalation is also unlikely to benefit patients who have never had a cytogenetic response or patients with hematologic failure; consequently, the use of high-dose Gleevec also appears to have major limitations as a second-line agent. Combination use of Gleevec with traditional chemotherapeutic agents, such as cytarabine and pegylated IFN-alfa, is also being investigated as a potential first-line regimen in a number of studies in newly diagnosed chronic-phase CML patients. The Nordic CML Study Group investigated the combination use of pegylated IFNalfa2b and Gleevec. Despite significant improvements in MMR rate in the combination arm, toxicity resulted in 61 percent of patients discontinuing IFN. Similar findings have been reported from the SPIRIT and GIMEMA studies, highlighting the need to balance tolerability with efficacy. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA FUTURE DIRECTIONS OF THERAPY Prior to the TKI era, CML was the most common indication for allogeneic HSCT worldwide. However, transplant rates have dropped dramatically following the approval of Gleevec and the excellent responses observed with TKI therapy. The use of HSCT as a first-line treatment option for chronic-phase CML is now no longer recommended and transplant is generally only considered following failure of TKI therapy. However, improvements in transplantation and the management of complications may lead to renewed interest in HSCT as a curative option. Cost also plays a major role in therapeutic decision making, particularly in more financially constrained healthcare systems. Considering the lifetime costs of TKI therapy and patient monitoring, HSCT may seem a more attractive option from a cost-effectiveness perspective. In Europe, the median cost of one year of Gleevec therapy is €30,411, compared with a median cost of €63,450 for a potentially curative HSCT. A study in Mexico calculated that the cost of a non-myeloablative allogeneic HSCT was equivalent to 180 days of Gleevec therapy. With the investigation of alternative donor sources and development of less toxic regimens, HSCT as a first-line option may see a resurgence of interest. Transplant also remains an option for patients who have not responded to or relapsed after TKI therapy, although poor survival is still associated with advanced stages of the disease. The current approach to CML therapy is sequential treatment with TKIs, with initiation of a second-line agent once failure of the first-line agent has been documented. However, it has been suggested that combination TKI therapy may be a more rational approach to induce rapid responses and combat drug resistance. Indeed, the concept of chronic use of highly active combination regimens seems feasible given the transformational success of HAART in HIV therapy. However, tolerability and cost of such regimens for CML are likely to be important considerations. Careful patient selection may identify patients at high risk of resistance who would benefit the most from combination regimens. Given the effectiveness of current TKIs, trials of combination regimens may be hindered due to patient reluctance to receive an investigational therapy when their PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA disease is adequately controlled with their current regimen. The high cost of TKIs may also be a significant barrier to combination treatment; it has been estimated that a regimen of Sprycel and Gleevec would cost approximately $78,000 per patient per year, which may be unfeasible given the chronic nature of therapy. However, significantly improved efficacy may lead to such deep and durable responses that therapy could potentially be discontinued, thus driving down treatment costs and conferring significant patient benefit. With the increasingly deep and durable responses to therapy being observed, a pertinent question is whether TKIs can eventually be discontinued in patients with consistently undetectable disease and the patient considered effectively cured. The multicenter STIM trial evaluated the possibility of stopping Gleevec treatment in patients with complete molecular remission, defined as undetectable BCR-ABL transcripts for ≥ 2 years. Although recurrence of molecular disease was observed in 61 percent of patients following discontinuation of Gleevec, all patients responded to reintroduction of therapy. The findings suggest that discontinuation might be feasible in a subset of patients along with close molecular monitoring to catch recurrence early. Further studies are required to assess the duration of “cure” and to determine whether the more potent second-generation TKIs will increase the proportion of patients for which discontinuation may be an achievable goal. CONCLUSION I The development of Gleevec as the first rationally designed, targeted oncology drug was a truly transformational event in the treatment of CML and an inspiration wider oncology field. As more efficacious therapies reach the market, the choice of firstline therapy will be increasingly driven by tolerability and costeffectiveness as patients remain on treatment for increasingly extended periods of time. Striving for even greater and deeper response rates remains a challenge for new therapies, as does the need for new treatments to overcome resistance to the first- and second-generation agents. With HSCT currently the only curative option for CML, the ultimate question is now whether cure can be effectively achieved with a small-molecule therapeutic. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA SECTION II DEALS HIGHLIGHTS Deals coverage on Cortellis for Competitive Intelligence indicates that more than 40 deals related to CML have been forged since the early 1990s. The following section reviews the licensing portfolio of a number of blockbuster CML therapeutics, as well as certain significant and promising therapeutic candidates for CML, as featured in Cortellis for Competitive Intelligence. Other notable and high-value deals are also highlighted to give an insight into the CML market. NOvARtis AND BRistOl-MyERs squiBB: MARkEt lEADERs FOR CMl thERAPEutiCs As the developer of both the blockbuster CML therapy Gleevec, which yielded sales of over $4.6 billion in 2011, and of its secondgeneration counterpart Tasigna, which generated sales of over $0.7 billion in 2011, expected to increase to more than $2.0 billion in 2016, Novartis is clearly at the forefront of this evolving therapeutic market. Novartis holds exclusive global rights to both drugs, with very little partnering activity; the only reported deal that involves Gleevec was more related to a non-CML oncology indication. Variagenics agreed in May 2002 to apply its integrated cancer pharmacogenomics platform to Novartis’s Gleevec and PKI-166, with the aim of identifying potential markers of the efficacy of the two drugs for prostate cancer. Novartis was to gain an exclusive license to any markers predictive of therapeutic response and Variagenics was to retain exclusive rights to develop any resulting DNA diagnostic tests. The financial terms of the agreement were undisclosed. “The expanded agreement also provides an opportunity for Bristol-myers squibb and otsuka to work together in oncology. We believe that sharing our collective resources will benefit the cancer patients we serve.” lamberto Andreotti, President and Chief Operating Officer, Bristol-Myers squibb PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA BMS follows Novartis as a prominent player in the field with its second-generation TKI, Sprycel. The company reported sales of the drug to be more than $0.8 billion in 2011, expected to increase to over $1.5 billion in 2016. BMS also demonstrates limited partnering activity for Sprycel, forging only a copromotion deal with Otsuka Pharmaceutical in April 2009. The companies agreed to co-promote BMS’s oncology assets, Sprycel, and Ixempra, in the US, Japan and Europe, and to share commercial expenses. BMS would pay Otsuka a collaboration fee on aggregate annual net sales, beginning in 2010 and continuing on a regressive tiering basis through 2020. By March 2011, it was reported that the agreement was to start that year for the US and Japan, and in 2012 for Europe. liCENsiNg PORtFOliO OF NOtABlE CMl thERAPEutiC CANDiDAtEs Significant and promising therapeutic candidates for CML include bosutinib, ponatinib, danusertib, AT-9283 and omacetaxine mepesuccinate, all of which are in late clinical development or the early stages of registration. The following section highlights known partnering activity for these compounds. Pfizer’s acquisition of Wyeth in October 2009 resulted in Pfizer being granted worldwide rights to the dual SRC/BCR-ABL kinase inhibitor bosutinib. Wyeth had entered a research collaboration for the drug with the University of Bologna by April 2005; however, financial details were undisclosed. ARIAD Pharmaceuticals holds the global development and marketing rights to the dual SRC/pan-BCR-ABL inhibitor ponatinib. Under the Qualifying Therapeutic Discovery Project (QTDP) program, the company was awarded three US Government grants in November 2010, totaling approximately $733,000, to support development of its oncology drugs ridaforolimus, ponatinib and AP-26113. An exclusive collaboration was entered into in March 2011 with MolecularMD for the development and commercialization of a companion diagnostic test for ponatinib; the test would identify the T315I BCR-ABL mutation in patients with CML and Ph+ acute lymphoblastic leukemia (ALL). MolecularMD agreed to continue using its diagnostic test to sequence BCRABL mutations in patients enrolled in ponatinib clinical trials. Under the collaboration terms, MolecularMD would further optimize the diagnostic test and would file a Premarket Approval Application (PMA) with the FDA to support commercialization. At that time, it was expected that MolecularMD would submit the PMA at the same time as ARIAD files its ponatinib NDA in 2012. MolecularMD’s scientific founder, Dr Brian Druker of the Oregon Health & Science University, was reported to be a long-standing scientific and medical collaborator of ARIAD’s in the development of ponatinib. ARIAD was to reimburse MolecularMD for predefined expenses related to the development of the T315I diagnostic test. MolecularMD would also receive development and regulatory milestone payments. “We have been working with ARiAD throughout ponatinib’s clinical development and share in the excitement over the drug’s activity in resistant and intolerant Cml patients and those with the T315i mutation for whom current therapies are ineffective.” stephane Wong, Chief scientific Officer, MolecularMD Following its acquisition of Astex Therapeutics in July 2011, Astex Pharmaceuticals (previously known as SuperGen) is developing a program of Aurora kinase inhibitors led by AT-9283. Cancer Research UK reported in January 2012 that it was funding and managing a first-in-child study of the drug for ALL and acute myeloid leukemia (AML). The funding amount was undisclosed. Nerviano Medical Sciences’s Aurora kinase inhibitor danusertib remains unpartnered. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA hOsPiRA’s $120-MilliON DEAl tO COMMERCiAlizE ChEMgENEx’s OMACEtAxiNE AND OthER AgREEMENts FOR thE thERAPEutiC CANDiDAtE Cephalon, a wholly owned subsidiary of Teva Pharmaceutical Industries, owns global rights to omacetaxine mepesuccinate following its acquisition of ChemGenex Pharmaceuticals in March 2011. ChemGenex and Stragen Pharma entered into a worldwide collaboration to accelerate clinical development of omacetaxine in June 2005. Stragen, which was to provide GMP manufacturing, distribution and marketing expertise, had a patented manufacturing process for a semi-synthetic purified form of the active molecule (homoharringtonine) in omacetaxine and had patented a suite of its derivatives. ChemGenex exclusively licensed worldwide rights to this manufacturing process and the novel analogs. Stragen had responsibility for drug production, global supply and facilitation of European regulatory approvals. Stragen’s established European clinical network was also utilized to accelerate the drug’s development. The companies planned to market omacetaxine under the ChemGenex brand in Europe, with ChemGenex receiving 49 percent of profits and Stragen receiving 51 percent. Three years later, in June 2008, ChemGenex gained full commercial control of omacetaxine through the transfer of IP and commercial rights from Stragen. This arrangement removed the IP royalty on manufacturing, significantly reduced the cost of goods and removed the need for a European joint venture, which allowed ChemGenex to control European development and access all profits from sales in the region. Stragen would continue to supply the drug and became a significant shareholder in ChemGenex, obtaining 37,235,343 new ordinary shares. As such, the original manufacturing and commercialization agreements between the companies were concluded and a strong combined patent portfolio around homoharringtonine and related analogs would provide broader and longer market exclusivity. The acquisition allowed ChemGenex to freely pursue commercialization opportunities for omacetaxine. “We are very excited by the promise omacetaxine holds to improve outcomes for seriously ill patients who have stopped responding to other treatments available for their condition. This agreement is a further step in hospira’s strategy to build upon our strong portfolio of oncology and hematology products.” Michael kotsanis, President Europe, Middle East and Africa, hospira PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA Indeed, in December 2009, ChemGenex granted Hospira development and commercialization rights to omacetaxine for hematological malignancies, in Europe, the Middle East and certain African countries. Hospira agreed to pay €11.1 million (approximately $15.9 million) upfront, milestones of up to €74.1 million (approximately $105.9 million) and royalties. ChemGenex would register the drug in Europe for CML while the companies explored applications of the drug in further hematological malignancies. Hospira would be responsible for marketing in its territories. ChemGenex’s development of omacetaxine was supported by a US Government grant of $244,479, obtained through the QTDP program in November 2010. In February 2012, the company planned to submit an NDA to the FDA by mid 2012 for omacetaxine in CML patients who have failed two or more TKIs. NOvARtis’s $0.5-BilliON DEAl tO liCENsE sgx’s BCRABl iNhiBitORs FOR CMl Novartis’s presence in the CML therapy arena is further illustrated by its $0.5 billion deal signed in March 2006 for CML therapeutic candidates, one of the highest valued for the indication. Novartis licensed codevelopment and commercialization rights to SGx Pharmaceuticals’ BCR-ABL inhibitors for drug-resistant CML. SGx received $25 million upfront, stock purchases, up to $490 million in milestones and royalties, plus a minimum of two years of research funding. SGx retained the option to co-commercialize the compounds in the US. The agreement was amended in September 2007; SGx acquired the right to develop and commercialize one of the compounds from the series, SGx-393, outside of the collaboration subject to Novartis’s reacquisition right that was exercisable at a future date. Novartis also assumed responsibility for the selection of future development candidates and the clinical development of additional compounds. However, following the acquisition of SGx by Eli Lilly in August 2008, no further development on the compounds has been reported by either Lilly or Novartis (see TABLE 2). DRUG LICENSING COMPANY PARTNER COMPANY DEAL START DATE DEAL VALUE (US $)* Gleevec Variagenics Novartis May 2002 undisclosed Sprycel Bristol-Myers Squibb Otsuka Pharmaceutical April 2009 undisclosed bosutinib University of Bologna Wyeth By April 2005 undisclosed ponatinib ARIAD Pharmaceuticals US Government November 2010 0.733 million ponatinib MolecularMD ARIAD Pharmaceuticals March 2011 undisclosed ponatinib Oregon Health & Science University ARIAD Pharmaceuticals By March 2011 undisclosed AT-9283 Astex Pharmaceuticals Cancer Research UK January 2012 undisclosed omacetaxine Stragen ChemGenex Pharmaceuticals June 2005 undisclosed omacetaxine ChemGenex Pharmaceuticals Hospira December 2009 <121 million + royalties omacetaxine ChemGenex Pharmaceuticals US Government November 2010 0.244 million BCR-ABL kinase inhibitors, SGx-393 SGx Pharmaceuticals Novartis March 2006 <515 million + royalties “novartis is the leader in developing novel targeted therapies to treat Cml. With their extensive experience developing and commercializing gleevec as well as development of the novel investigational compound, nilotinib/Amn107, we believe they are the ideal partner with whom to develop our series of next-generation BCRABl inhibitors.” Mike grey, President and CEO, sgx Pharmaceuticals table 2. summary oF notable agreements For chronic myeloiD leuKemia therapeutics * Approximate values based on the achievement of all milestones for the principal components included in the deal. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA CONCLUSION II On observing the deal landscape for CML, it is clear that Novartis is the leading player; the company has developed two of the top three significant blockbuster therapeutics in the market, Gleevec and Tasigna ($5.375 billion combined sales figures in 2011), and it has forged one of the highest-value deals for the indication ($0.5 billion with SGx in 2006). BMS follows on, with Sprycel sales of $0.803 billion in 2011. It is notable that there appears to be very little partnering activity for the blockbuster CML therapeutics. This trend is also reflected when studying the partnering landscape for promising CML therapeutic candidates such as bosutinib, ponatinib, danusertib, AT-9283, and omacetaxine. Deals with Otsuka (BMS’s Sprycel), MolecularMD (ARIAD’s ponatinib), and Stragen and Hospira (both for ChemGenex‘s omacetaxine) are among the few that appear significant. This could represent a gap in the market, providing potential opportunities for investment and licensing activity. As new therapeutics emerge (eg, bosutinib and ponatinib with expected sales in 2016 of $140 million and $570.3 million, respectively) and compete with more established drugs, it will be of interest to see if the CML deals landscape is at all altered. PHARMA MATTERS | SPOTLIGHT ON... CHRONIC MYELOID LEUKEMIA REUTERS / Henry Watkins & Yibran Aragon HIDDEN DRUG OPPORTUNITIES IN THE PIPELINE JUST GOT EASIER TO SPOT Find it faster with Thomson Reuters Cortellis™ for Competitive Intelligence, the new pharmaceutical pipeline database from Thomson Reuters. With industry-leading competitive intelligence, you can stay one step ahead of the competition while discovering and nurturing your company’s best opportunities for growth. For more information visit: cortellis.thomsonreuters.com Thomson REUTERS CORTELLIS. Discover the Undiscovered. cortellis.thomsonreuters.com NOTES NOTES To sign up to the Spotlight On… report and receive it on a quarterly basis, please visit: go.thomsonreuters.com/spotlight To sign up to our Pharma Matters range of publications visit: go.thomsonreuters.com/pharmamatters THE ONES TO WATCH Focuses on the latest phase changes in the pharmaceutical pipeline. MOVERS AND SHAKERS Unravels the most significant game-play in the US generics market. THE CUTTING EDGE OF CHEMISTRY Insights into the chemistry advances transforming drug discovery and development. ABOUT THOMSON REUTERS CORTELLIS FOR COMPETITIVE INTELLIGENCE Cortellis for Competitive Intelligence combines the same premier information used by the world’s leading pharmaceutical companies from products such as Thomson Reuters Pharma™ and Thomson Reuters Partnering™ (formerly IDDB). From drug discovery data to patent reports, the latest deals to partnering opportunities, Cortellis for Competitive Intelligence can give you the confidence to make the best business decisions, faster. ABOUT THOMSON REUTERS Thomson Reuters is the leading source of intelligent information for professionals around the world. Our customers are knowledge workers in key sectors of the global economy. We supply them with the intelligent information they need to succeed in fields that are vital to developed and emerging economies such as law, financial services, tax and accounting, healthcare, science and media. Our knowledge and information is essential for drug companies to discover new drugs and get them to market faster, for researchers to find relevant papers and know what’s newly published in their subject, and for businesses to optimize their intellectual property and find competitive intelligence. NOTE TO PRESS: To request further information or permission to reproduce content from this report, please contact: Laura Gaze Phone: +1 203 868 3340 Email: [email protected] For more information on Thomson Reuters Cortellis visit: cortellis.thomsonreuters.com or email [email protected] thOMsON REutERs REgiONAl OFFiCEs North America Philadelphia +1 800 336 4474 +1 215 386 0100 Latin America Brazil +55 11 8370 9845 Other countries +1 215 823 5674 Europe, Middle East and Africa London +44 20 7433 4000 Asia Pacific Singapore +65 6775 5088 Tokyo +81 3 5218 6500 For a complete office list visit: ip-science.thomsonreuters.com/ contact ls - 201204 - BD&l - sOR Copyright © 2012 Thomson Reuters