Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
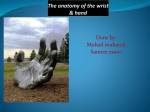
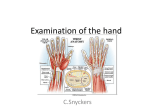
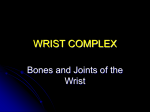
HAND ANATOMY A. HAND FUNCTIONS 1. Touch 2. Precision handling: rotation, translation 3. Power grip: squeeze, hook, spherical grip 4. Pinch: pulp, pincer, key, chuck 5. Expression: writing, signalling, shaking hands, caressing B. HAND ANATOMY LAYERS OF THE PALM: 1. Skin 2. Palmar aponeurosis 3. Superficial palmar arch 4. Thenar and hypothenar muscles 5. Long flexor tendons 6. Adductor pollicis 7. Metacarpals and interossei 1. SKIN A. Dorsum Thin,soft and pliable skin with hair follicles. Loose areolar tissue anchors skin to deeper layer, but very little fat is present. Major venous and lymphatic channels run dorsally. B. Palmar Thick dermal layer with heavily cornified epidermal layer. Skin held tightly to thick fibrous palmar fascia by vertical fibres of palmar fascia Very little laxity. Stability of palmar skin is critical to hand function. High concentration of specialised sense organs and sweat glands. Reacts very poorly to scarring. THE NAIL Part of volar skin. Functions: 1. protection 2. stabilisation Rate of growth: The whole nail bed is responsible for nail growth. + 0.1 mm per day. 2. SUPERFICIAL PALMAR FASCIA (APONEUROSIS): Resistant fibrous tissue arranged longitudinally, transversely, obliquely and vertically. Originates at the wrist, usually as a triangular extension of PL tendon if present (80-85%). The fascia fans out distally to form pretendinous bands in the palm. The pretendinous bands bifurcate at MPJ level and spread at the base of each digit to send the bulk of fibres distally into the fingers to make up the fibrous flexor sheaths. Together with the natatory ligaments, the pre-tendinous bands form the digital fascias of Cleland and Grayson which are attached to the skin. The natatory ligaments lie in the web spaces and prevent them from excessive abduction. Grayson’s ligaments run between the fibrous flexor sheath and the dermis along the length of the finger. Cleland’s ligaments run between the bone and the dermis, dorsal to Grayson’s ligaments, along the length of the finger. The digital nv bundles lie between the two. In the mid-palm, transverse fibres are found = Transverse Palmar Ligament (Skoog) or superficial transverse fascia. These fibres lie deep to the longitudinal fibres and are inseparable from them. This transverse fascial layer has a free distal edge, beyond which lies a space containing the neuro-vascular bundle (lying in fat) and which is bounded laterally by the pretendinous bands and distally by the natatory ligament. These spaces bulge when the fingers are hyperexteded. The fascia is also inseparable from the vertical septae that run downwards to form divisions between the longitudinally orientated structures in the hand. The transverse fibres thus form the roof of 8 tunnels that convey the flexor tendons (in 4 tunnels) and the neurovascular bundles and lumbrical muscles (in 4 other tunnels). They act as pulleys for the flexor tendons proximal to the digits. Indistinct longitudinal fibres pass to the thumb which blend with the deep fascia overlying thenar muscles. On the ulna aspect, palmar fascia blends with the hypothenar fascia. Palmar fascia also attaches to: 1. palmar plate, 2. intermetacarpal ligaments. 3. TENDONS The flexor tendons, at the level of the MCP joint, enter a fibro-osseous tunnel, the flexor sheath. The functions of the flexor sheath are: 1. to stabilise the tendons closely against the bone, 2. to facilitate efficient excursion of the tendons, 3. to provide for tendon nutrition. Tenosynovium lines the inner aspect of the sheath, as well as the tendons themselves. At specific sites the sheath is thickened to form pulleys. Annular pulleys (A1 - A5) Cruciate pulleys (C1 - C3) The A2 and A4 pulleys are the most important in maintaining finger flexion. Without these two the tip of the finger cannot be brought to the distal palmar crease. ZONES I Distal to FDS insertion. II No man's land - From FDS insertion distally to lumbrical insertion proximally. III Mid palm - From lumbrical insertion to carpal tunnel. IV Within the carpal tunnel. V Wrist VI Forearm. STRUCTURES CROSSING THE FLEXOR RETINACULUM: ULNAR SIDE Ulnar nerve CENTRALLY RADIAL SIDE Palmaris longus tendon Palmar br of median n Ulnar artery Superf palmar br of radial a 4. BONES 27 Bones, divided into 3 groups: 1. the carpus 2. the metacarpals 3. the phalanges THE 4 ELEMENTS OF THE HAND SKELETON (In ascending order of specialisation) 1. The fixed unit of the hand: index and middle MC's and distal carpal row 2. The middle, ring + little fingers, (including the ring and little MC's). Functions either as: (1) A stabilising vice to grasp objects (2) With other hand units in powerful grasp 3. The index Independent ROM Acting on the index: 3 intrinsic muscles 4 extrinsic muscles 4. The thumb and it's MC Wide ROM at MCP joint. Acting on the thumb: 4 intrinsic muscles 5 extrinsic muscles 5. JOINTS: WRIST: radio-ulnar, radio-carpal (wrist), carpo-carpal CMC MCP PIP DIP NORMAL ROM WRIST: Flexion: 0 to 70-90° Extension: 0 to 70-90° Radial deviation: 0 to 20° Ulna deviation: 0 to 30° Pronation: 0 to 90° Suppination: 0 to 90° FINGERS: MCP joint: 0 to 75-95° PIP joint: 0 to 90-125° DIP joint: 0 to 70-85° THUMB: MCP joint: 0 to 30-90° IP joint: -10 to 70-90° 1. WRIST JOINT AND CARPO-CARPAL JOINTS: Ligamentous Anatomy: a) Collateral ligaments: Radial collateral ligament Ulnar collateral ligament b) Palmar ligaments: Radial 1. Radio-capitate - Supports the waist of the scaphoid 2. Radio-triquetral - Supports the lunate 3. Radio-scaphoid - Checkrein for the scaphoid Ulnar 1. Ulno-lunate 2. Ulno-triquetrum c) Dorsal: - Dorsal Radio-carpal The ulno-carpal complex consists of: the triangular fibrocartilage ulno-lunate ligament ulnar collateral ligament TESTS: The piano key test to evaluate distal radio-ulnar joint. The scaphoid shift manoeuvre for instability of scapho-lunate ligament. The luno-triquetral shear manoeuvre for luno-triquetral lig. 2. CARPO-METACARPAL JOINTS Divided into mobile, very mobile and relatively static: VERY MOBILE: Thumb CMC MOBILE: L CMC LESS MOBILE: R CMC RELATIVELY STATIC: M + I CMC Saddle joint 3. MCP JOINTS: Stabilised by collateral ligaments and volar plate. Volar plate (of both MCP + IP joints) is fibrocartilaginous. The digital flexor tendons lie just anterior to the volar plates of MCP + IP joints. MC heads are cam shaped so that the collateral ligaments tighten in flexion and slacken in extension. This permits abduction in extension. Prolonged fixed extension allows shortening of collateral ligaments resulting in a fixed extension deformity which is extremely difficult to correct. 4. IP JOINTS: Hinge joints. Bicondylar. Stabilised by volar plate and collateral ligaments. The volar plate is part of the joint capsule and prevents hyper-extension. The collateral ligaments are also part of the capsule. They prevent medial or lateral deviation at the joint. Loss of the collateral ligaments results in instability and ulnar deviation. (Also a function of the interossei). The collateral ligaments are equally tight in flexion and extension. 5. MUSCLES C5 - Deltoid C6 - Brachioradialis, Wrist extensors C7 - Triceps, Finger extensors C8 - Finger flexors T1 – Intrinsics INTEROSSEI: 3 palmar and 4 dorsal. Palmar arise from the middle finger side of MC and insert into the extensor expansion and PP. Dorsal arise from 2 MC bones and insert into the extensor expansion away from the middle finger. Action: Abduct and adduct the fingers (PAD + DAB). Test by: Paralysis results in: Flex MCP joints and extend IP joints. DAB and PAD, flexing the MCP joints with the IP joints extended. clawing of the fingers hyperextension of the MCP joints flexion of the IP joints. LUMBRICALS Arise from each of the 4 FDP tendons and pass along the radial side of the MCP joint to insert into the extensor expansion over prox phalanges. Nerve supply: Ulnar : Median Flex MCP joints and extend IP joints. Test by extending the fingers while holding active flexion at the MCP joint. 2:2. TESTS: EXTRINSIC EXTENSOR TIGHTNESS: When MCP jt is extended, one is able to passively flex the PIP jt, but, if the extrinsics are tight, one will not be able to do so when MCP jts are flexed. INTRINSIC EXTENSOR TIGHTNESS: When MCP jt is flexed, one is able to passively flex the PIP jt, but, if the intrinsics are tight, one will not be able to do so when MCP jts are extended. BOUVIERS TEST: If by preventing MCP joint hyperextension the patient is able to fully extend his or her proximal IP joints, the extensor mechanism is normal. When extension of the proximal IP joints remain incomplete despite preventing MCP joint hyperextension, the central tendon has become attenuated or adherent at the proximal IP joint or the lateral bands volarly subluxed. If by Bouvier test full extension is achieved it is not necessary to insert any tendon into the extensor mechanism. Such transfers are most safely and effectively inserted into the proximal phalanges or into the A1 or A2 pulley. Extensor tendon insertion or Littler extensor reconstruction is only indicated when Bouvier,s test fail - that is for the "complicated" claw deformity. 6. NERVES Each of the 3 passes through a muscle in the forearm. Each of the 3 passes points of potential entrapment. MEDIAN NERVE Grasps an object and pulls it closer: Flexes the fingers and closes the thumb. Enters the forearm and passes between the heads of pronator teres. Directly innervates: Pronator teres, FCR, PL, FDS (while running deep to it). Innervates through anterior interosseous branch: Radial part of FDP (to I and M) FPL Pronator quadratus Anterior inerosseous innervates IP flexors and pronator quadratus. Travels down the forearm between FDS and FDP. Enters the hand through the carpal tunnel, (with FDS + FDP tendons). Gives off the palmar cutaneous br to skin of wrist and palm which is superficial to the flexor retinaculum. Divides in the hand into 3 branches: 1. Thenar br to Abd Policis Brevis, Superficial belly of FPB (variably so) and OP. 2. Lateral br to Th (digital nerves), 1st cleft, radial side of I and to 1st lumbrical. 3. Medial br to 2nd and 3rd clefts (common digital nn and their respective terminal digital branches) and to the 2nd lumbrical ULNAR NERVE Sets the stage for grasping: ie, Flexes MPs, extends IPs. Enters the forearm from behind the medial epicondyle. Passes between the 2 heads of FCU to innervate in the forearm: FCU and FDP (ulnar part). Gives off the dorsal br (with a br of the artery) about at the junction of the middle and distal 1/3s of the forearm: supplies sensation of dorsum of hand and ulnar 1 1/2 fingers proximal to the nail bed. With the artery, the main nerve enters the hand at the wrist (nerve lies on the ulnar side of the artery) by passing through Guyon’s canal: radial to the pisiform, ulnar to the hook of the hamate, deep to the volar carpal ligament, superficial to the deep transverse palmar ligament. In the hand the ulna nerve splits into superficial and deep branches. The superficial br supplies the palmaris brevis muscle and then divides into a medial (to ulnar side of hand and L finger) and lateral br (common digital n to 4th cleft). The deep br innervates the hypothenar muscles, the 7 interosseii, the lumbricals to R and L, the Add policis, and possibly all or part of FPB (usually the deep head). ANATOMICAL CROSS OVER CONNECTIONS: May mask the site of injury: ulnar n injury can still have normal intrinsics d/t innervation by the anterior interosseous n or median n (M-G); median n injury may still have thenar muscle function (R-C); median n injury may result in loss of function of all intrinsics d/t these being supplied by the crossovers. 1. Martin-Gruber Between ulna and median nerves in the forearm present in about 17% of people. 4 types: 1. Proximal ulnar median 2. Median ulnar 3. Anterior interosseous ulnar 4. Distal ulnar median 2. Riche-Cannieu Between ulna and median in the hand, present in up to 70% of people. 3 types have been described. Generally, results in variable ulnar innervation of the thenar muscles. RADIAL NERVE Reaches out: ie, Elbow extension, wrist dorsiflexion, finger extension, thumb extension and abduction. Gives off post cut nerve of the arm. Above the elbow, the radial nerve directly innervates: triceps, anconeus, BR, ECRL and, as the nerve enters the forearm, it supplies ECRB. It passes through the supinator muscle and splits into superficial sensory br and deep motor br = posterior interosseous n. The posterior interosseous n supplies: supinator ECU EDC EIP EDM EPL EPB APL To the digits To the thumb DIGITAL NERVES In the palm, the digital nerves lie dorsal to the common digital arteries. In the digit, the digital nerves lie volar to arteries Gives off a dorsal sensory branch at the level of the mid proximal phalanx which supplies the dorsal skin over the middle and distal phalanges. At the DIP, the digital nerve trifurcates to give off 3 branches: 1. perionychium br 2. branch to finger tip 3. branch to volar pulp MECHANISM OF INJURY OF PERIPHERAL NERVES Non-traumatic 1. Systemic disease eg DM 2. Neurologic disease: Myasthenia Gravis. 3. Exposure to environmental toxins: eg lead. Traumatic 1. Nerve division 2. Compartmental syndrome (Starts as sensory alteration. Last sensation lost is pain, opposite to LA). 3. Traction 4. Chronic compression (combines ischaemia and mechanical pressure). 7. CIRCULATION Allen's test 1. Compress radial and ulna arteries at the wrist. 2. Exsanguinate the hand (pt opens and closes his fist). 3. Release one artery only and note filling of hand. 4. Repeat steps 1 to 3, with the other artery. Normal filling time < 5 secs. Can do the Allen test on a single digit.