Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
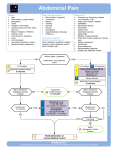
1 Educational Strategies to Promote Clinical Reasoning October 2014 Illness Script EXAMPLE Disease: Adult Community Acquired Pneumonia Epidemiology Time Course Clinical Features (1) History (2) Exam (3) Labs (4) Imaging/Advanced Studies Pathophysiology Treatment Typical illness course Smoking, alcohol, immunosuppression, chronic lung diseases Acute to subacute (1) Fever, cough, dyspnea (2) Fever, hypoxia, rales, egophany (3) Leukocytosis (4) Chest x-ray: infiltrate Microbes establish infection in alveoli Doxycycline >> Levofloxacin Usually patients improve after 2-3 days of antibiotics; may take weeks to fully resolve cough, dyspnea. Memorable cases / anecdotes Last year my patient died because MRSA pneumonia was not covered soon enough. When I was a resident, Dr. Smith thought of legionella in very sick young man in ICU with pneumonia and saved his life. Recent reading / studies Do not have to be afebrile x 24 hours for discharge. Shorten duration of treatment to 5-7 days. Areas of ambiguity (in the field) Value of sputum gram stain and culture. Areas of ambiguity (for you) Is decreased O2 saturation important if only with exertion but not at rest? Clinical “pearls” Always ask “Could this be tuberculosis?” Aspiration is a pneumonitis not pneumonia. 2 The brain has to define a problem before it can solve it - that’s the purpose of problem representation… A 19 year old woman is brought to the emergency department because of unresponsiveness. HPI: 4 days ago she developed cough, sore throat, and rhinorrhea. Yesterday she slept until 12 noon and upon awakening complained of a diffuse headache and mild neck pain. She went about her usual activities. Fever, increasing headache, and vomiting developed that night; no abdominal pain or diarrhea. She denied chest pain, dyspnea, cough, and urinary symptoms. The roommate was unable to arouse the patient the next morning. PMH: none Meds: none HRB: social alcohol, does not smoke, no drugs now, marijuana in the past; sexually active with boyfriend Soc Hx: 2nd year college student T 39.2°C BP 100/55 P 118 RR 14 Sat 97% RA Somnolent, arousable to physical stimuli but unable to follow commands for exam. Pupils are 3mm sluggish. Oropharynx: clear. Neck: Limited range of motion. No lymphadenopathy. Lungs: Clear Heart: RRR, no murmur Abdomen: soft, not tender No peripheral edema or rash Moves all four extremities without focality. Babinski reflex negative bilaterally. Develop your PROBLEM REPRESENTATION for this case. (i.e., what is the concise one liner that contains all the high yield information you would want your trainee to present to you?) 3 Reasoning Dx/Rx Case Studies: Group Exercise Your MS3 in clinic sees a 69 year old man with difficulty initiating urinary stream for past three weeks. He reports the following: “Middle aged man here who is having trouble urinating. The urine just dribbles out and he has a hard time getting the urine stream started. It happens up to three times per day. No blood. He denies abdominal pain, but does have a cough. I asked him about a stone, but he doesn’t think he has one. His heart, lung, and abdominal exam are normal. There’s no murmur. The triage nurse asked if we needed labs, so I got a CBC that shows a little anemia; the creatinine is normal, so it’s not a kidney problem. It still could be a kidney stone but I’m also worried about bladder cancer.” Correct diagnosis is benign prostatic hypertrophy. Elements of Diagnostic Reasoning 1. Data Collection ? 2. Problem Representation ? 3. Illness Script ? 4. Script Selection ? 4 Scenario 1 You are the emergency room physician listening to a case from an EM intern, who reports: Correct diagnosis is septic pre-patellar bursitis (infection of fluid pocket anterior to the patella/knee cap), which can be challenging to distinguish from septic joint. 42 year old man with left knee pain. Over last 2 days he’s had had progressive left knee swelling with increasing pain and limitation of movement. Today he developed a fever of 38.9C. He had never had knee or joint problems before. No previous trauma. He was installing his living room carpet last week and was playing on the floor this weekend with his 16 month old niece. He thinks perhaps he strained his knee playing with her. He otherwise feels well. No past medical history or medications. Temp is 38.4C. General exam is normal [he tells you all relevant components]. Left knee is red and swollen, although it’s swollen in front of the knee rather than within the joint, but it’s difficult to say for sure because of the swelling. He is most tender in front of the knee. He can move the joint through a full ROM, but it hurts. Serum white blood cell count is 13,000. In summary, he is a healthy man with fever and the acute onset of a single sustained episode of severe pain and swelling in the left knee, more in the front of the joint. I know it is unusual to have intact range of motion in septic joint, so I’m not really sure what it is. Elements of Diagnostic Reasoning 1. Data Collection 2. Problem Representation 3. Illness Script 4. Script Selection 5 Scenario 2 You are the gynecology attending on evening rounds with the second year resident. Correct diagnosis is post-operative internal bleeding following a hysterectomy. R2: Ms. Park. 67 years old. She had an uncomplicated total abdominal hysterectomy this afternoon. After she arrived on the ward she has been feeling lightheaded. Her incision looks fine but her abdomen is distended, and the hemoglobin has decreased by 4.5 grams. She is afebrile. Her blood pressure has decreased to 92/50 mm Hg and her pulse is 105. She has hypertension, diabetes, and a history of elevated liver function tests with a negative hepatitis serology. Medications are …[shows list]. I/O’s are 3 liters positive. EKG is sinus tachycardia, but no ischemic changes. Attending: What do you think is going on? R2: The post-op recovery isn’t normal. I am concerned about the abdominal distention. It could be constipation or bladder obstruction. More serious would be post-operative urinary leak or hemorrhage, or maybe some liver disease causing ascites. It is probably too early for a major post-operative ileus. Attending: What about the declining hemoglobin and abnormal vital signs? R2: She might be tachycardic because of post-operative pain. She could be withdrawing from alcohol too. I know you can see anemia and low blood pressure in end stage liver disease. I think we should do an ultrasound of the abdomen, and if there is ascites, we should do a paracentesis. Attending: If there is a lot of fluid on ultrasound, it is most likely a hemoperitoneum. That would explain the fluid in the abdomen, the low hemoglobin, the increased pulse, and the low blood pressure. R2: I’ll get the bedside ultrasound now. I will ask the nurse to administer more intravenous fluid and will check her complete blood count and coagulation studies. I’ll also inform the chief resident that we may have to return to the operating room and give the operating room personnel a heads up. Attending: Why is she bleeding now? R2: There might be a slow bleeding vessel that we did not see during the operation. Now it has to be tied off or cauterized. There was no pre-op coagulopathy or bleeding history we knew of. This type of interaction is typical of this resident, who has achieved the top score on the inservice exam for the past two years and answers all factual questions with great skill. 6 Scenario 3 The third year medical student rotating in your family medicine clinic presents the following patient: This is a challenging case of abdominal pain for which there is no definitive diagnosis made by any provider even at the conclusion of the visit. She is 39-year-old woman with abdominal pain for 3 days. She describes the pain as dull, crampy, and diffuse. She has vomited five times over the past 2 days without hematemesis. She has had one episode of loose stool. She has felt feverish without chills. No recent change in diet. No travel. No other sick contacts. Her menses have been normal and her last period ended yesterday. No dysuria or flank pain. PMH: Hepatitis C diagnosed last year. She has had an appendectomy as a child and a tubal ligation four years ago. She takes over-the-counter multivitamins, NSAIDs, and antacids. She drinks heavily at Friday happy hours, and has cocktails during the weekend. She is divorced and sexually active with 1 male partner. She works as a paralegal in a law firm in San Francisco. Thin, in moderate discomfort. T: 37.5°C, HR 110, BP 92/65, RR 18, Sat 99% RA Mental status is normal. Head/Neck/Heart/Lung/Extremities: normal No jaundice or other evidence of liver disease. Abdomen: mild distension, +epigastric tenderness; bowel sounds are diminished; no hepatosplenomegaly; well healed RLQ scar. Pelvic (bimanual): normal adnexa, no cervical motion tenderness Rectal examination for occult blood: negative. You ask the student for his assessment: I am not sure. This is a 39 year old with subacute, diffuse, progressive abdominal pain and nausea and vomiting. In a woman with abdominal pain the first thing I think about is ectopic pregnancy, but her tubes are tied and she just had her period, so that is impossible. Appendicitis is also possible, but she said her appendix was removed. I would think consider peptic ulcer disease, acute cholecystitis, pancreatitis, hepatitis, and small bowel obstruction, especially with her previous surgery. Urinary tract infection can also give non-localizing abdominal pain. She is in the proper age group for inflammatory bowel disease, but I forgot to ask for family history about that. 7 Elements of Diagnostic Reasoning 1. Data Collection 2. Problem Representation a. Key features b. Abstraction 3. Illness Script (Knowledge) 4. Illness Script Selection a. Compare/Contrast b. Prioritization c. Verify/Reject