Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
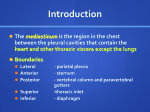
RADIOLOGICAL EXAMINATION OF THE MEDIASTINUM AND DIAPHRAGM. DEPARTMENT OF ONCOLOGY AND RADIOLOGY PREPARED BY I.M.LESKIV • Abnormalities can be seen on either plain films or CT. Metastatic disease to the chest may involve one or more of the following: lungs; pleura; lymph nodes; local invasion; bony skeleton. • Lymph nodes • CT is accurate in the detection of enlarged hilar and mediastinal lymph nodes. (CT will detect nodes I cm in size and smaller, but nodes < I cm are less likely to be metastatic.) • Lymphangitis carcinomatosa — secondary deposits in central lymph nodes may produce lymphatic congestion with a linear pulmonary pattern radiating outwards from the hilar glands, septal lines and pleural effusions. • Local invasion • Pericardium to give malignant pericardial effusion; superior vena cava compression or obstruction; phrenic nerve paralysis; Pancoast's tumour. •Diaphragm • The diaphragm consists of a thin sheet of muscle with a smooth upward convexity, the right usually lying in a higher position than the left. On a chest film, the inferior surface of the diaphragm is not visualized as it blends with the surfaces‘ of the liver and spleen. • CAUSES OF A UNILATERAL ELEVATED DIAPHRAGM • Above diaphragm: phrenic nerve palsy; infiltration from bronchial carcinoma or mediastinal tumour. • Diaphragm: eventration, more common on the left and results from deficiency or atrophy of muscle. • Below diaphragm: right diaphragm elevation; liver or subphrenic abscess, liver secondary deposits. • CAUSES OF BILATERAL ELEVATED DIAPHRAGMS • Obesity. • Hepatosplenomegaly. Within the abdomen: ascites, pregnancy, abdominal masses. • A congenital defect in the diaphragm, more common on the left, allows bowel protrusion into the thoracic cavity and usually results in respiratory distress. Herniation may occur at three sites though those causing neonatal respiratory distress are usually of the Bochdalek type. • • Foramen of Bochdalek: posterior diaphragm. • • Foramen of Morgagni: anterior diaphragm. • • Oesophageal hiatus. • RADIOLOGICAL FEATURES • Antenatal ultrasound examination often detects the herniation. A chest X-ray illustrates either cyst-like changes or the typical appearance of multiple bowel loops in the thorax. Mediastinal shift is away from the affected side. Abdominal films may show absence or paucity of bowel loops. • TREATMENT • Surgical repair of the diaphragm, but pulmonary hypoplasia and pulmonary hypertension cause a significant mortality. • A mediastinal mass due to a hiatus hernia is usually easy to diagnose on plain films because it often contains air and may have a fluid level, best seen on the lateral view. A film taken after a mouthful of barium has been swallowed will easily confirm or exclude the diagnosis of hiatus hernia. Hiatus hernia, (a) Lateral and (b) PA chest films show the characteristic retrocardiac density containing an air-fluid level (arrows). Masses in the right cardiophrenic angle anteriorly are virtually never of clinical significance. They are nearly all either large fat pads, benign pericardial cysts or hernias through the foramen of Morgagni Fat pads in both cardiophrenic angles. Note the loss of clarity of the adjacent cardiac outline - an example of the silhouette sign. The anterior location was confirmed on the lateral view • Paralysis of a hemidiaphragm. This results from disorders of the phrenic nerves, e.g. invasion by carcinoma of the bronchus. The signs are elevation of one hemidiaphragm which on fluoroscopy or ultrasound shows paradoxical movement, i.e. it moves upward on inspiration Carcinoma of the bronchus at the left hilum causing collapse of the left upper lobe and paralysis of the left phrenic nerve. The elevated left hemidiaphragm is too high to be due to the lobar collapse; it is due to phrenic nerve involvement by the tumour at the left hilum. Eventration of the diaphragm. This is a congenital condition in which the diaphragm lacks muscle and Localized eventration of the diaphragm. There is becomes a thin membranous a smooth localized elevation of the medial half of sheet. Except in the neonatal the right hemidiaphragm (arrows). On the lateral period it is almost always an view the eventration involved the anterior half of incidental finding and does not the right hemidiaphragm. cause symptoms. When the whole of one hemidiaphragm is involved, almost invariably the left, that hemidiaphragm is markedly elevated. On fluoroscopy or ultrasound, the hemidiaphragm may remain fixed during inspiration and expiration, but when more severely involved it moves paradoxically and cannot be distinguished from paralysis. The eventration may only involve part of one hemidiaphragm, resulting in a smooth 'hump MEDIASTINAL MASS • The mediastinum is that part of the chest bounded by the sternum at the front, thoracic spine at the back and laterally by the medial surfaces of visceral pleura. It can be divided into: anterior mediastinum: anterior to the pericardium; middle mediastinum: the heart, aortic root and pulmonary vessels; posterior mediastinum: behind the posterior pericardial surface. Mediastinal compartments. Although the mediastinum is categorized into compartments, masses may freely cross from one part to another. • RADIOLOGICAL FEATURES • Usually, a mediastinal mass is suspected on a plain chest film; a lateral film may be helpful; further evaluation is carried out by CT/MRI for anatomical localization. The presence of cystic lesions, calcification, fat and vascular structures are all more accurately assessed than by plain films. • • Anterior mediastinal masses (three Ts—thyroid, thymus and teratodermoids) Retrosternal thyroid: the mass is well defined and may be lobulated. Exten sion into the mediastinum is to a varying degree up to the carina. Thymic tumours: these may be benign or malignant and frequently associ ated with myasthenia gravis. • Teratodermoids: these tumours are usually benign but have a malignant potential. Occasionally fat, rim calcification, bone fragments and teeth may be identified. • • Middle mediastinal masses • Lymphadenopathy: lymphoma, metastases, sarcoid or tuberculosis. • • Posterior mediastinal masses • Neurogenic tumours arising from intercostal nerves and sympathetic • chain. • Neurofibromas (nerve sheath tumours). • Ganglioneuroma (sympathetic nerve cell tumours). • The anterior (A), middle (M) and posterior (P) compartments of the mediastinum. The divisions are arbitrary and do not correspond to those used by anatomists. The anterior mediastinum refers to the structures anterior to the trachea and the major bronchi. The posterior mediastinum refers to structures posterior to a line joining the anterior boundary of the vertebral bodies. ANTERIOR: 1.Thyroid tumour, Thymic tumour or cyst, Teratoma/Dermoid cyst, Lymphadenopathy, Aortic aneurysm. 2. Pericardial cyst, Fat pad, Morgagni hernia MIDDLE: 3. Thyroid tumour, Lymphadenopathy, Bronchogenic cyst, Aortic aneurysm. 4. Hiatus hernia POSTERIOR: 5. Neurogenic tumours, Soft tissue mass of vertebral infection or neoplasm, Lymphadenopathy, Aortic aneurysm Computed tomography scanning provides a much clearer idea of the position, shape and size of any mass than is possible from the plain chest radiograph; occasionally the CT density even enables a specific diagnosis to be made. Magnetic resonance imaging provides more information than CT only in highly selected cases. Intrathoracic thyroid masses (goitres) are the most frequent cause of a superior mediastinal mass. The characteristic feature is that the mass extends from the superior mediastinum into the neck and almost invariably compresses or displaces the trachea. Retrosternal goitre, (a) The plain chest film shows a large superior mediastinal mass narrowing the trachea, (b) A radionuclide scan in the same patient shows the level of the clavicles on the right, confirming that the mass is due to thyroid tissue, (c) CT scan, in another patient, showing a bilateral superior mediastinal mass that was shown on adjacent sections to be contiguous with the thyroid gland in the neck and to have the same density as thyroid tissue. Note the compression of the trachea. • Lymphadenopathy is the next most frequent cause of a mediastinal swelling. Lymphadenopathy may occur in any of the three compartments and it is often possible to diagnose enlarged lymph nodes from their lobulated outlines and the multiple locations involved Superior mediastinal lymph node enlargement. Note the bilateral lobular masses. Extensive mediastinal lymphadenopathy (caused b lymphoma) shown by CT scanning. • Hilar lymphadenopathy may cause enlargement of the hilar shadows, the lymph nodes appearing as well-defined, lobulated masses. Nodal enlargement has to be differentiated from hilar vascular prominence (as in pulmonary hypertension). Difficulty may be encountered in distinguishing between them on chest radiography, though CT with contrast or MRI accurately identifies the abnormality. • CAUSES OF BILATERAL HILAR GLAND ENLARGEMENT • Sarcoidosis: commonest cause, usually resolving spontaneously. • Lymphoma: mediastinal glands are more frequently involved than hilar. • Tuberculosis: enlargement is usually asymmetrical and often associated with mediastinal glandular involvement. • Metastases. • CAUSES OF UNILATERAL HILAR GLAND ENLARGEMENT • Bronchial carcinoma. • Lymphoma. • Tuberculosis. Bilateral hilar adenopathy. The enlarged hila are clearly lobular in outline and there is also enlargement of the right paratracheal nodes (arrow). The diagnosis in this patient was malignant lymphoma. • Neurogenic tumours are by far the commonest causes of a posterior mediastinal mass. Pressure deformity of the adjacent ribs and thoracic spine is often visible. *Certain tumours, such as dermoid cysts and thymomas, are, for practical purposes, confined to the anterior mediastinum. Thymoma, (a) CT and (b) MRI (Tl-weighted) show a lobular mass (arrows) in the left side of the thymus a b Dermoid cyst (cystic teratoma) (arrows) shown by CT to contain fat. In this cyst the fat can be seen floating in the upper third of the cyst. Note that the density of part of the cyst is the same as subcutaneous fat. • Neurofibroma in posterior mediastinum. The MRI shows the neurofibroma (arrows) lying against the spine, but not growing into the spinal canal. • Calcification occurs in many conditions but almost never in malignant lymphadenopathy. Occasionally, the calcification is characteristic in appearance, e.g. in aneurysms of the aorta Calcification in an aneurysm arising from the descending aorta. The arrows point to the distinctive curvilinear calcification within the mass, which is in intimate contact with the aorta. Aneurysm of the descending aorta. The lumen has been opacified by intravenous contrast enhancement. The unopacified component is a blood clot lining the aneurysm.