Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
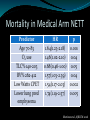
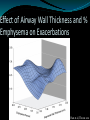
Nathaniel Marchetti, DO Temple University Philadelphia, PA The National Emphysema Treatment Trial (NETT) NETT Productivity >75 peer reviewed publications using NETT data Who should and should not have LVRS? What did we learn about emphysema? Pathobiology of emphysema Genetics Role of hyperinflation Hemodynamics in advanced emphysema Measurements of lung function in severe empysema Racial differences in severe emphysema Mortality in emphysema Medical therapy in severe emphysema Oxygen use in severe emphysema Criner et al, AJRCCM, 2011 NETT Design 17 clinical centers Randomized 1,218 patients to medical therapy or medical therapy plus LVRS Screened 3,777 Pulmonary function FEV1 15% to 45% TLC >105% RV > 150% No significant cardiac disease or pulmonary HTN No other pulmonary diseases present Bilateral emphysema amenable to LVRS Upper lobe predominant Diffuse NETT Research Group Chest, 1999 NETT Design Pulmonary rehab 16-20 sessions pre-randomization 10 sessions post-randomization Long term maintenance Aggressive bronchodilator therapy Surgical therapy Bilateral stapled resection of 25-30% of lung Median sternotomy at 8 centers VATS at 3 centers 6 centers randomized to MS vs VATS NETT Research Group Chest, 1999 NETT Design Anesthesia Intra-operative care standardized Median sternotomy patient has epidural catheters Extubation within 2 hours Physical therapy started on 1st post-op day NETT Research Group Chest, 1999 Outcomes Primary Survival 10 W improvement on CPET Secondary Quality of life Cost effectiveness Pulmonary function CT scans and nuclear perfusion scans Oxygen requirement 6 minute walk distance Cardiovascular measures (echo) NETT Research Group Chest, 1999 Survival Surgical 90-day mortality = 7.9% Medical 90-day mortality = 1.3% NETT Research Group NEJM, 2003 Survival High risk group FEV1 < 20% predicted + Either DLCO < 20% or homogeneous emphysema Surgical 30-day mortality = 16% Medical 30-day mortality = 0% NETT Research Group NEJM, 2003 Survival excluding high risk Surgical 30-day mortality = 2.2% Medical 30-day mortality = 0.2% NETT Research Group NEJM, 2003 Survival UL and low exercise = YES UL and high exercise = NO NETT Research Group NEJM, 2003 Survival Non-UL and low exercise = NO Non-UL and high exercise = NO NETT Research Group NEJM, 2003 Exercise performance all patients Months 6 12 24 10 watt improvement LVRS Medical Rx 28% 4% 22% 5% 15% 3% p value <0.001 <0.001 <0.001 NETT Research Group NEJM, 2003 Durability of LVRS High risk patients excluded Naunheim et al, Ann Thorac Surg 2006 Durability of LVRS UL/Low Exercise UL/high Exercise Naunheim et al, Ann Thorac Surg 2006 Durability of Exercise UL/Low UL/High Naunheim et al, Ann Thorac Surg 2006 Quality of Life Durability MCID for SGRQ is -4 but a priori was -8 for NETT Naunheim et al, Ann Thorac Surg 2006 PaO2 Following LVRS Snyder et al, AJRCCM 2008 O2 needs following LVRS Snyder et al, AJRCCM 2008 LVRS Enhances CO2 Elimination During Exercise Sub-study CPET with a-line (n=47) Criner et al, Chest 2009 LVRS Improves f/VT Index Criner et al, Chest 2009 LVRS Reduces Exacerbations Surgical 0.27 exacerbations/patient-year Medical 0.37 exacerbations/patient-year 30% reduction (13-48%, p=0.0005) Washko et al, AJRCCM 2008 Most important lessons from NETT? LVRS works!! Interventions to improve survival Smoking cessation Oxygen LVRS LVRS improves Oxygenation and oxygen requirements Favorable alters breathing patterns Reduces exacerbations Who should not get surgery? NETT Research Group NEJM, 2001 Who should not have LVRS? Criner et al, PATS 2008 Durability of non-UL/high exercise Naunheim et al, Ann Thorac Surg 2006 Who should not have LVRS? Criner et al, PATS 2008 α-1 Antitrypsin Deficiency 16 patients had severe deficiency (<80 mg/dL) 10 randomized to surgery 7 had upper lobe predominant emphysema Compared to the 6 that had medical Rx LVRS mortality was higher (20% vs 0%) Compared to normal α-1 AT levels Less improvement in exercise Less improvement in FEV1 response Stoller et al, Ann Thorac Surg 2007 What did NETT teach us about surgical techniques? LVRS and Air Leaks 580/608 patients had surgery Air leak data available on 552 90% had air leak in first 30 days Presence of air leak not effected by Surgical approach (VATS vs MS) Use of any buttressing agent (fibrin glue, etc) Stapler brand Intraoperative procedures Pleurodesis Tenting DeCamp et al, Ann Thorac Surg 2006 Duration Median 7 days DeCamp et al, Ann Thorac Surg 2006 Consequence of air leak No difference in mortality Longer hospital stay (11.8+6.5 vs 7.6+4.4 d, p=0.0005) Increased pneumonia (20% vs 7.4%) Increased ICU admission (9.3% vs 1.9%) DeCamp et al, Ann Thorac Surg 2006 Risk Factors Increased risk and duration Lower diffusion capacity (p=0.06) Upper lobe disease (p=0.04) Presence of moderate to severe adhesions (p=0.007) Increased Duration Caucasian race (p<0.0001) Use of inhaled steroid (p=0.004) Lower FEV1 (p=0.0003) DeCamp et al, Ann Thorac Surg 2006 Video Assisted Thorascopy (VATS) vs Median Sternotomy (MS) 8 centers used MS 3 used VATS 6 randomized to either Total patients: 359 MS vs 152 VATS Randomized patients: 77 MS vs 71 VATS McKenna et al, J Thorac Cardiovasc Surg, 2004 VATS vs MS 30 day mortality 2.8% MS vs 2.0% VATS (p = 0.76) 90 day mortality 5.9% MS vs 4.6% (p = 0.67) No mortality difference for randomized patients Intra-operative hypoxemia more common in VATS (0.8% vs 5.3%) No difference in days with air leak Median hospital LOS of 10 d in MS vs 9 in VATS (p=0.01) Randomized patients: 15d for MS vs 9d for VATS (p<0.001) McKenna et al, J Thorac Cardiovasc Surg, 2004 Costs of VATS Compared to MS VATS = MS for outcomes and complications Shorter hospital stay with VATS Less expensive McKenna et al, J Thorac Cardiovasc Surg, 2004 Pathologic Lessons Small Airway Disease in Emphysema? Thickened Epithelium Inflammation Subepithelial Fibrosis Smooth Muscle Hypertrophy Nature of Small Airway Obstruction in COPD 159 patients across all GOLD stages 59 GOLD III/IV patients from NETT 100 GOLD 0–III patients Measure small airway (<2mm) luminal content and the amount of inflammation in airway Correlated luminal occlusion and airway edema with FEV1 Hogg et al, NEJM 2004 Luminal Occlusion Hogg et al, NEJM 2004 FEV1 falls as lumen occludes r = -0.505, p=0.001 Hogg et al, NEJM 2004 FEV1 falls as the airway thickens r = -0.687, p<0.001 Hogg et al, NEJM 2004 More inflammatory cells with increasing GOLD stage Hogg et al, NEJM 2004 Significance of Small Airway Disease in Emphysema Airway thickening is possibly tissue remodeling Decreased mucociliary clearance leading to obstruction Increased lymphoid follicles possibly secondary to: Repeated infection Bacterial colonization Persistent inflammation may explain the decline in lung function even after smoking cessation All NETT subject non-smokers >6 months Hogg et al, NEJM 2004 Decreased Survival with Luminal Occlusion OR 3.28, 1.55-6.92; p=0.002 Hogg et al, AJRCCM 2007 Effect of ICS or Oral Steroids No effect on airway thickness or luminal occlusion r = -0.505, p=0.001 Less airway associated lymphoid follicles for those on oral steroids Represents decreased adaptive immunity Could this explain increased pneumonia? Hogg et al, AJRCCM 2007 Mortality and Emphysema Predictors of mortality in severe emphysema 609 patients in the medical arm of NETT Well characterized Severe disease with high mortality High quality long term follow up Martinez et al, AJRCCM 2006 Mortality in Medical Arm NETT Predictor Age 70-83 O2 use TLC% 140-203 RV% 262-412 Low Watts CPET Lower lung pred emphysema HR p 1.64(1.23-2.18) 0.001 1.46(1.02-2.10) 0.04 0.68(0.46-1.00) 0.05 1.57(1.03-2.39) 0.04 1.54(1.17-2.03) 0.002 1.74(1.19-2.57) 0.005 Martinez et al, AJRCCM 2006 BODE in multivariate model Predictor Age 70-83 Hb 9.1-13.3 RV% 262-412 Low Watts CPET Lower lung pred emphysema DLCO % 6-21 HR 1. 72(1.31-2.26) 1.38(1.00-1.89) 1.48(1.04-2.37) 1.48(1.12-1.94) 1.74(1.19-2.57) p <0.001 0.05 0.03 0.006 0.005 1.36(1.01-1.84) 0.04 BODE 7-10 1.48(1.07-2.05) 0.02 Martinez et al, AJRCCM 2006 Not predictive FEV1 alone (i.e. not in BODE) Total % of emphysema on CT scan DL was weak in multivariate CO PaO2 was not predictive while O2 use was Oxygen increases mortality or epimarker of disease severity? LOTT Martinez et al, AJRCCM 2006 mBODE Change in COPD Predicts Mortality BODE change in medical and surgical arms NETT Divided group into BODE classes Decrease by 1 No change Increase by 1 Data missing Used to predict death Martinez et al, AJRCCM 2008 Changes in mBODE Martinez et al, AJRCCM 2008 mBODE Change in Surgical Cohort and Mortality P<0.01 Martinez et al, AJRCCM 2008 HR for Change in mBODE P<0.01 Martinez et al, AJRCCM 2008 Genetic Epidemiology of COPD (COPDGene) Study Design Multi-center (21) observational study Designed to identify genetic factors associated with COPD Genome-wide association study (GWAS) analysis to be done Will permit identification of radiographic and clinical phenotypes to be identified Regan et al, COPD 2011 COPDGene Study Population 10,000 subjects enrolled with 2/3 non-Hispanic whites and 1/3 African American Enrollment goals were met early Inclusion criteria Self identified as non-Hispanic white or African American Age 45-80 with 10 pack-years smoking history Regan et al, COPD 2011 COPDGene Study Population Exclusion criteria Pregnancy due to CT imaging Other lung disease except asthma Prior LVRS or lobectomy Active cancer Suspected lung cancer Metal in the chest Recent AECOPD requiring therapy Recent eye surgery 1st or 2nd degree relative already in study History of chest radiation therapy Regan et al, COPD 2011 Data Collected Blood for genetic and biomarker analysis Inspiratory and expiratory HRCT scans with sub- millimeter thickness Pre and post bronchodilator spirometry ATS respiratory questionnaire medical history, medications St George’s respiratory questionnaire BMI, blood pressure, oxygen saturation Six minute walk test Regan et al, COPD 2011 Analysis HRCT phenotyping Emphysema quantification Gas trapping Airway wall thickness GWAS: look for genes associated with following: COPD status defined by GOLD criteria FEV1% as a continuous variable HRCT parameters listed above Regan et al, COPD 2011 Epidemiology of COPD GOLD Undefined Subjects Data from 1st 2,500 subjects 9% of current or ex-smokers with Low FEV1 but preserved FEV1/FVC ratio GOLD-U has been described previously Stable pattern Associated with increased mortality Associated with significant symptoms COPDGene provided largest database with both clinical and radiographic data Wan et al, AJRCCM 2011 Comparison of GOLD U to Controls and COPD Cases Wan et al, AJRCCM 2011 GOLD-U Comparison GOLD-U Controls COPD Wan et al, AJRCCM 2011 GOLD-U Predictors Wan et al, AJRCCM 2011 Significance of GOLD-U Represents significant # of smokers/ex-smokers Clinical course largely unknown ?progression Are these changes related to obesity alone? BMI contributes but changes in FEV1 are > than previously reported No reduction in FRC compared to smoking controls Early Onset COPD: Differences of Race and Sex First 2,500 subjects only Early onset definition: Age <55 FEV1/FVC < 0.7 FEV1 <50% predicted Comparator group Age >64 FEV1/FVC < 0.7 FEV1 <50% predicted Foreman et al, AJRCCM 2011 Demographic & Clinical Differences Foreman et al, AJRCCM 2011 Multivariate Analysis Foreman et al, AJRCCM 2011 Significance of Findings Early onset COPD is rare African Americans and women disproportionately affected Smoked less Maternal history of COPD is important Genetic follow up studies pending Foreman et al, AJRCCM 2011 Racial Differences in Quality of Life in COPDGene African Americans smoked less, were younger but had the same lung function Han et al, Chest 2011 St George Respiratory Questionnaire African Americans had worse SGRQ scores (higher) Han et al, Chest 2011 Multivariate Analysis After adjustment for age, sex, pack-years smoking, education level, MMRC dyspnea, 6MWD, and current smoking status no difference in quality of life in those without exacerbations African Americans with history of prior exacerbation (1.887 for every exacerbation, p = 0.006) Han et al, Chest 2011 Family History as a Risk for COPD COPD >GOLD II Hersch et al, Chest 2011 Multivariate analysis Controlling for demographics, parental history of smoking, parental history of COPD, childhood ETS Parental history of COPD OR 1.73 (1.36-2.2), p = <0.001 Paternal history COPD 1.66 (1.24-2.22), p = 0.006 Maternal history COPD 1.51 (1.10-2.09), p = 0.011 Hersch et al, Chest 2011 Clinical Phenotypes COPD Chronic Bronchitc Phenotype Variable Age Smoking, pk-yr Current smoker % Men % MMRC SGRQ total TLC, L FRC, L Mean WA% CB+ (n = 290) 62.8 + 8.4 57 + 30 48 57 3 (2-4) 49.9 + 19.7 6.30 + 1.50 4.22 + 1.19 63.2 + 2.9 CB- (n = 771) 64.6 + 8.4 52 + 25 27 50 2 (1-3) 36.6 + 20 5.88 + 1.40 3.92 + 1.28 62.6 + 3.1 P .002 0.006 <0.001 0.027 <0.001 <0.001 .004 .002 .013 Kim et al, Chest 2011 Chronic Bronchitics and AECOPD Kim et al, Chest 2011 Radiographic Features of Frequent Exacerbation Phenotype Han et al, Thorax 2011 Frequent vs non-frequent exacerbators Han et al, Thorax 2011 Effect of Airway Wall Thickness and % Emphysema on Exacerbations Han et al, Thorax 2011 Multivariate Analysis Han et al, Thorax 2011 Smoking Related ILD on HRCT Ground glass or reticular abnormalities Diffuse centrilobular nodules Non-emphysematous cysts Honeycombing Traction bronchiectasis Washko et al, NEJM 2011 ILA vs No ILA Variable No ILA (n = 1361) Age 60 (52-67) BMI 27 (24-31) Pack-yr smoking 40 (29-54) GOLD > stage 2 (%) 41 Unclassified GOLD % 7 % emphysema 4.1 (1.3-12.4) TLC, L 5.7 (4.8-6.78) ILA (n = 194) 64 (56-72) 28 (25-33) 44 (31-63) 32 14 3.3 (0.9-9.7) 5.21(4.38-6.270 P <0.001 0.006 0.01 0.02 0.002 <0.001 .004 Washko et al, NEJM 2011 Multivariate Analysis Adjusted for age, sex, BMI, smoking, COPD (except for COPD model) Washko et al, NEJM 2011 ILA and lower 6MWD Doyle et al, AJRCCM in press Genetics Three genetic loci identified as being associated with COPD susceptibility 4q24 6p21 5q33 Low BMI associated with COPD Pts from Eclipse, Norway-Bergen cohort, NETT and COPDGene Found an association of low BMI in SNP at FTO gene FTO gene has been associated with obesity Castaldi et al, AJRCMB 2011 Wan et al, AJRCMB 2011 Summary NETT Most of analysis is done LVRS improves survival, exercise performance, QOL Small airway disease is important even in emphysematous phenotype Use of BODE to track response to therapy COPDGene Most of analysis not yet done Genetics Definition of phenotypes which may lead to better directed Rx Radiographic Chronic bronchitis Smoking related diseases other than COPD exist GOLD U Interstitial changes on CT Conclusion Large multi-centered studies in COPD are feasible and lead to important findings NETT COPDGene ECLIPSE TORCH Continued co-operation amongst investigators will lead to new advances in COPD