Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
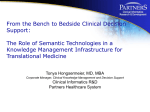
Prescriber Fax Form MediGold Tarceva (erlotinib) (Coverage Determination) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed forms to CVS/Caremark at 1-855-633-7673. Please contact CVS/Caremark at 1-866-785-5714 with questions regarding the prior authorization process. When conditions are met, we will authorize the coverage of Tarceva (erlotinib) (Coverage Determination). Drug Name (select from list of drugs shown): Tarceva (erlotinib) Patient Information Patient Name: Patient ID: Patient Group No.: Patient DOB: Patient Phone: Prescribing Physician Physician Name: Physician Phone: Physician Fax: Physician Address: City, State, Zip: Diagnosis: ICD Code: Please circle the appropriate answer for each question. 1. Does the patient have a diagnosis of non-small cell lung cancer? [If no, skip to question #10.] Yes No 2. Is the disease locally advanced, recurrent, or metastatic? [If no, no further questions.] Yes No 3. Will Tarceva be used as first-line treatment? [If no, skip to question #6.] Yes No 4. Has EGFR mutation testing been performed? [If no, no further questions.] Yes No 5. Does the patient have either exon 19 deletion or exon 21 (L858R) substitution mutation? [No further questions.] Yes No 6. Will Tarceva be used maintenance treatment? Yes No [If no, skip to question #8.] 7. Did the patient respond to or remain stable after first-line chemotherapy? [If yes, skip to question #9.] [If no, no further questions.] Yes No 8. Will Tarceva be used as second- or third-line treatment? [If no, no further questions.] Yes No 9. Will Tarceva be used as a single agent? [No further questions.] Yes No 10. Does the patient have a diagnosis of pancreatic cancer? [If no, skip to question #12.] Yes No 11. Does the patient meet ALL of the following criteria: Locally advanced, unresectable, or metastatic pancreatic cancer Tarceva will be used in combination with gemcitabine [No further questions.] Yes No 12. Does the patient have a diagnosis of chordoma? [If no, no further questions.] Yes No 13. Does the patient meet ALL of the following criteria: Chordoma is recurrent Tarceva will be used as monotherapy or in combination with Erbitux (cetuximab) Yes No Comments: I affirm that the information given on this form is true and accurate as of this date. Prescriber (Or Authorized) Signature and Date