Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
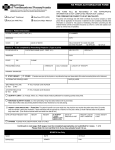
12/15/2016 Prior Authorization AETNA BETTER HEALTH OF MICHIGAN (MEDICAID) Entresto (MI88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed forms to Aetna Better Health of Michigan at 1-855-799-2551. Please contact Aetna Better Health of Michigan at 1-866-316-3784 with questions regarding the Prior Authorization process. When conditions are met, we will authorize the coverage of Entresto (MI88). Please note that all authorization requests will be reviewed as the AB rated generic (when available) unless states otherwise. Drug Name (select from list of drugs shown) Entresto (sacubitril/valsartan) Other, Please specify: ________________________________ Quantity Route of Administration Frequency Expected Length of therapy Strength Patient Information Patient Name: Patient ID: Patient Group No.: Patient DOB: Patient Phone: Prescribing Physician Physician Name: ________________________________________________________________________ Specialty: ___________________________ NPI Number: _________________________ Physician Fax: ___________________________ Physician Phone: _________________________ Physician Address: ___________________________ City, State, Zip: _________________________ Diagnosis: ICD Code: Please circle the appropriate answer for each question. Question 1. Does the patient have New York Heart Association Class 2-4 (NYHA Class II-IV) Heart Failure AND a reduced ejection fraction of less than or equal to 40 percent? Circle Yes or No Y N [If no, then no further questions] 2. Is the patient tolerating an ACEI (angiotensinconverting-enzyme inhibitor) or ARB (angiotensin receptor blocker)? [If no, then no further questions] Y N Question 3. Will the ACEI or ARB be stopped when the patient starts Entresto? Circle Yes or No Y N [If no, then no further questions] 4. Will Entresto be used with other heart failure therapies such as beta blockers, aldosterone antagonist, and/or hydralazine plus isosorbide? Y N Y N Y N Y N [If no, then no further questions] 5. Is the patient pregnant? [If yes, then no further questions] 6. Does the patient have severe hepatic impairment (Child Pugh Class C)? [If yes, then no further questions] 7. Is the patient 18 years of age or older? Comments: I affirm that the information given on this form is true and accurate as of this date. Prescriber (Or Authorized) Signature Prescriber (Or Authorized) Signature Date Date