Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
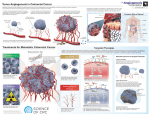
Vol. 9, 3219 –3221, August 15, 2003 Clinical Cancer Research 3219 Editorial The Importance of Platelet Counts and Their Contents in Cancer Henk M. W. Verheul and Herbert M. Pinedo1 Department of Internal Medicine, University Medical Center Utrecht, 3508 GA Utrecht [H. M. W. V.], and VU Medical Center-Cancer Center-Amsterdam, Amsterdam 1007 MB [H. M. P.], the Netherlands VEGF,2 a potent angiogenic growth factor, plays an important role in several pathophysiological processes including tumorigenesis. It is presumably involved in the angiogenic switch from the initial avascular phase of a microscopic tumor into a progressively, rapidly growing and metastasizing tumor by stimulation of new vessel formation. Because of this important role, many investigators have been studying whether circulating VEGF can be used as a prognostic marker in patients with different cancer types, including breast cancer. These kind of studies have been performed since the beginning of the 90s, reviewed by Hormbrey et al. (1). In this review, the differences between the methods that were used for obtaining and measuring plasma and serum VEGF in these studies were compared, and they proposed a standardized way to collect and measure VEGF in blood samples of cancer patients. After initial reports that serum VEGF is increased in cancer patients, we published in this journal in 1997 that serum VEGF concentrations in breast cancer patients were determined by platelet counts and not by tumor burden (Fig. 1). We found that platelets release VEGF on activation. Therefore, we predicted that plasma VEGF instead of serum VEGF concentrations should be studied as a marker for tumor progression (2). In addition, we found evidence that platelets may be involved in tumor-induced angiogenesis because of their release of angiogenic growth factors on activation by angiogenic endothelium (3). Apart from VEGF, platelets contain several other angiogenic growth factors and inhibitors that are released on activation, including platelet-derived endothelial cell growth factor, transforming growth factor-, hepatocyte growth factor, thrombospondin, and even endostatin (4). In addition, other studies report an increased VEGF content of platelets from cancer patients compared with healthy volunteers (5, 6). Now, 6 years later, the dispute is still ongoing whether serum VEGF or plasma VEGF should be used as a marker of tumor progression or prognosis. Some studies show that platelet-poor plasma reflect more accurate tumor progression (7), Accepted 8/15/03. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 To whom requests for reprints should be addressed, at VUMC-Cancer Center-Amsterdam, P. O. Box 7057, 1007 MB Amsterdam, the Netherlands. E-mail: [email protected]. 2 The abbreviations used are: VEGF, vascular endothelial growth factor; TPO, thrombopoietin. whereas others found that serum VEGF gives a better indication of tumor progression (6). Heer et al. (8) published earlier in this journal that serum VEGF detects breast cancer preoperatively with a sensitivity of 62.1%. In addition, they show a relation with the estrogen positivity of the tumors and VEGF levels. In this issue of Clinical Cancer Research, Murphy et al. (9) question again whether these measurements of serum-VEGF are meaningful, because they published earlier that plasma VEGF but not serum VEGF is elevated in breast cancer patients when these levels were compared with healthy volunteers (10; see Letters to the Editor in this issue). Taken the different studies together, the question remains whether serum-VEGF or plasma-VEGF should be determined. When taking these different opinions and findings together, what do they tell us about tumor biology? Is it possible that tumors stimulate the megakaryocytes in the bone marrow to generate increasing amounts of platelets that contain more VEGF? If so, which tumor-released factor is responsible for this, and secondly, what is the effect on tumor progression? It is well known that tumors can stimulate the bone marrow; for example, it has been shown that tumors promote the mobilization of progenitor endothelial cells from the bone marrow, and presumably VEGF plays an important role in this pathway (11). In addition, it has been shown that tumors initiate intratumoral activation of the coagulation cascade including platelet activation (disseminated intravascular coagulation; Ref. 12). Furthermore, platelets have been shown to contain TPO and release it on activation. TPO is the specific cytokine that stimulates megakaryocytes in the bone marrow to generate platelets. Folman et al. (13) suggested a self-regulatory vicious circle of platelet counts and the bone marrow controlled by TPO. In response to an injury of the vessel wall or any other local thrombogenic process, platelets attach to the vessel wall and subsequently become activated and release their contents, including TPO. On its turn, this platelet-released TPO stimulates the bone marrow to generate new platelets into the circulation. We hypothesize that activated platelets in the tumor vasculature release TPO, and thereby stimulate bone marrow generation of platelets (Fig. 2). As a consequence of our hypothesis, an increased number of platelets will reach the circulation as we often see in cancer patients. On the basis of this hypothesis both plasma VEGF and serum VEGF may be important to indicate tumor activity. Plasma VEGF may be increased because of direct tumor release of VEGF, and by tumor-induced intravascular platelet activation and subsequent VEGF release. On the other hand, elevated serum VEGF may be the consequence of increased platelet numbers in cancer patients caused by intratumoral platelet activation and subsequent release of TPO. In conclusion, as mentioned before, we strongly recommend in any study regarding circulating VEGF to include plasma and serum levels, and platelet counts. Hopefully we will come to a better understanding of what role circulating growth factors and platelets play in tumor biology. In the end, it might well be that just a simple platelet count is a better prognostic Downloaded from clincancerres.aacrjournals.org on May 15, 2017. © 2003 American Association for Cancer Research. 3220 Platelet Counts and Their Contents in Cancer Fig. 1 VEGF concentrations and platelet counts during treatment with chemotherapy plus granulocyte macrophage colony-stimulating factor in breast cancer patients. The chemotherapy administration is given every 3 weeks. Fig. 2 In the tumor vasculature, tumor produced growth factors (GF), including VEGF, activate the endothelium into a prothrombotic state causing subsequent platelet activation with TPO and VEGF release. This release of growth factors and cytokines by platelets on its turn stimulate bone marrow generation of platelets and progenitor endothelial cells (CECs). Subsequently, these bone marrowderived cells are thought to play an important role in the angiogenic process in the tumor. factor compared with plasma or serum VEGF concentrations in cancer patients (14, 15). References 1. Hormbrey, E., Gillespie, P., Turner, K., Han, C., Roberts, A., McGrouther, D., and Harris, A. L. A critical review of vascular endothelial growth factor (VEGF) analysis in peripheral blood: is the current literature meaningful? Clin. Exp. Metastasis, 19: 651– 663, 2002. 2. Verheul, H. M., Hoekman, K., Luykx-de Bakker, S., Eekman, C. A., Folman, C. C., Broxterman, H. J., and Pinedo, H. M. Platelet: transporter of vascular endothelial growth factor. Clin. Cancer Res., 3: 2187–2190, 1997. 3. Verheul, H. M., Jorna, A. S., Hoekman, K., Broxterman, H. J., Gebbink, M. F., and Pinedo, H. M. Vascular endothelial growth factorstimulated endothelial cells promote adhesion and activation of platelets. Blood, 96: 4216 – 4221, 2000. 4. Ma, L., Elliott, S. N., Cirino, G., Buret, A., Ignarro, L. J., and Wallace, J. L. Platelets modulate gastric ulcer healing: role of endostatin and vascular endothelial growth factor release. Proc. Natl. Acad. Sci. USA, 98: 6470 – 6475, 2001. 5. Salven, P., Orpana, A., and Joensuu, H. Leukocytes and platelets of patients with cancer contain high levels of vascular endothelial growth factor. Clin. Cancer Res., 5: 487– 491, 1999. 6. Lee, J. K., Hong, Y. J., Han, C. J., Hwang, D. Y., and Hong, S. I. Clinical usefulness of serum and plasma vascular endothelial growth factor in cancer patients: which is the optimal specimen? Int. J. Oncol., 17: 149 –152, 2000. 7. Wynendaele, W., Derua, R., Hoylaerts, M. F., Pawinski, A., Waelkens, E., de Bruijn, E. A., Paridaens, R., Merlevede, W., and Van Oosterom, A. T. Vascular endothelial growth factor measured in platelet poor plasma allows optimal separation between cancer patients and volunteers: a key to study an angiogenic marker in vivo? Ann. Oncol., 10: 965–971, 1999. 8. Heer, K., Kumar, H., Read, J. R., Fox, J. N., Monson, J. R., and Kerin, M. J. Serum vascular endothelial growth factor in breast cancer: its relation with cancer type and estrogen receptor status. Clin. Cancer Res., 7: 3491–3494, 2001. 9. Murphy, C. E., Lansdown, M. R. J., Speirs, V., and Carder, P. J. Correspondence re: K. Heer et al., Serum vascular endothelial growth factor in breast cancer: its relation with cancer type and estrogen receptor status. Clin. Cancer Res., 9: 3514, 2003. 10. Adams, J., Carder, P. J., Downey, S., Forbes, M. A., MacLennan, K., Allgar, V., Kaufman, S., Hallam, S., Bicknell, R., Walker, J. J., Cairnduff, F., Selby, P. J., Perren, T. J., Lansdown, M., and Banks, R. E. Vascular endothelial growth factor (VEGF) in breast cancer: comparison of plasma, serum, and tissue VEGF and microvessel density and effects of tamoxifen. Cancer Res., 60: 2898 –2905, 2000. Downloaded from clincancerres.aacrjournals.org on May 15, 2017. © 2003 American Association for Cancer Research. Clinical Cancer Research 3221 11. Lyden, D., Hattori, K., Dias, S., Costa, C., Blaikie, P., Butros, L., Chadburn, A., Heissig, B., Marks, W., Witte, L., Wu, Y., Hicklin, D., Zhu, Z., Hackett, N. R., Crystal, R. G., Moore, M. A., Hajjar, K. A., Manova, K., Benezra, R., and Rafii, S. Impaired recruitment of bone-marrow-derived endothelial and hematopoietic precursor cells blocks tumor angiogenesis and growth. Nat. Med., 7: 1194 –1201, 2001. 12. Verheul, H. M., Hoekman, K., Lupu, F., Broxterman, H. J., van, d., V, Kakkar, A. K., and Pinedo, H. M. Platelet and coagulation activation with vascular endothelial growth factor generation in soft tissue sarcomas. Clin. Cancer Res., 6: 166 –171, 2000. 13. Folman, C. C., Linthorst, G. E., van Mourik, J., van Willigen, G., de Jonge, E., Levi, M., de Haas, M., and dem Borne, A. E. Platelets release thrombopoietin (Tpo) upon activation: another regulatory loop in thrombocytopoiesis? Thromb. Haemost., 83: 923–930, 2000. 14. Ikeda, M., Furukawa, H., Imamura, H., Shimizu, J., Ishida, H., Masutani, S., Tatsuta, M., and Satomi, T. Poor prognosis associated with thrombocytosis in patients with gastric cancer. Ann. Surg. Oncol., 9: 287–291, 2002. 15. Pedersen, L. M., and Milman, N. Prognostic significance of thrombocytosis in patients with primary lung cancer. Eur. Respir. J., 9: 1826 –1830, 1996. Downloaded from clincancerres.aacrjournals.org on May 15, 2017. © 2003 American Association for Cancer Research. The Importance of Platelet Counts and Their Contents in Cancer Henk M. W. Verheul and Herbert M. Pinedo Clin Cancer Res 2003;9:3219-3221. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://clincancerres.aacrjournals.org/content/9/9/3219 This article cites 15 articles, 10 of which you can access for free at: http://clincancerres.aacrjournals.org/content/9/9/3219.full.html#ref-list-1 This article has been cited by 4 HighWire-hosted articles. Access the articles at: /content/9/9/3219.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on May 15, 2017. © 2003 American Association for Cancer Research.