Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
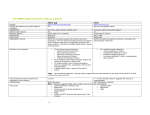
Support Care Cancer (2014) 22:2941–2955 DOI 10.1007/s00520-014-2250-z ORIGINAL ARTICLE Measuring symptoms in gastrointestinal cancer: a systematic review of assessment instruments Rachelle Pullmer & Wolfgang Linden & Katerina Rnic & Andrea Vodermaier Received: 8 September 2013 / Accepted: 9 April 2014 / Published online: 28 May 2014 # Springer-Verlag Berlin Heidelberg 2014 Abstract Purpose It is critical for gastrointestinal cancer researchers and clinicians to have access to comprehensive, sensitive and simple-to-use symptom measures that allow them to understand and quantify the subjective patient experience. Development and validation of such scales requires training in psychometrics and occasionally uses technical jargon that can be difficult to penetrate. This review evaluates existing measures of gastrointestinal cancer symptoms, provides tool descriptions, and uses predefined, objective quality criteria to rate psychometric quality and facilitate tool choices for researchers and clinicians. Methods MEDLINE, EMBASE, CINAHL, and PsycINFO databases were systematically reviewed for scales assessing gastrointestinal cancer and gastrointestinal cancer site-specific symptoms. Evaluation criteria were the following: breadth of domain coverage (content validity), high internal consistency (α≥ .80), sensitivity to change, and extent of validation. Results In n=36 validation studies, 26 gastrointestinal cancer symptom measures were identified. Of these, n=13 tools met criteria for recommendation, and six in particular showed strong psychometric properties. The Functional Assessment of Cancer Therapy-Colorectal (FACT-C), European Organization for Research and Treatment of Cancer (EORTC) gastric cancer module (QLQ-STO22), FACT-Hepatobiliary (FACT-Hep), and EORTC oesophagus, oesophago-gastric junction and stomach module (QLQ OG-25) were identified as the most comprehensive and best validated scales for each of the major gastrointestinal cancer sites. The FACT-Colorectal Symptom Index (FCSI9) and the National Comprehensive Cancer Network (NCCN) FACT-Hepatobiliary Symptom Index (FHSI-18) were specifically validated in patients with advanced colorectal and liver cancer and also demonstrated superior psychometric properties. Conclusions Several comprehensive, well-validated scales exist to adequately assess gastrointestinal cancer site-specific symptoms. Specifically, gastrointestinal cancer submodules of the FACT quality of life questionnaire represent adequate tool choices in most instances and overall, were better validated than the respective EORTC tools. Further improvement of existing, highly rated measures is recommended. Electronic supplementary material The online version of this article (doi:10.1007/s00520-014-2250-z) contains supplementary material, which is available to authorized users. Keywords Symptoms . Gastrointestinal neoplasms . Measures . Psychometrics . Reliability . Validity R. Pullmer (*) : W. Linden : A. Vodermaier Department of Psychology, University of British Columbia, 2136 West Mall, Vancouver, BC V6T 1Z4, Canada e-mail: [email protected] W. Linden BC Cancer Agency, Vancouver, BC, Canada K. Rnic Department of Psychology, University of Western Ontario, London, Ontario, Canada A. Vodermaier Department of Obstetrics and Gynecology—Campus Grosshadern, University of Munich, Munich, Germany Introduction While incidence of several gastrointestinal (GI) cancers continue to rise, mortality rates are generally declining, leading to an increase in survivors who must cope with symptoms arising from the disease and its treatment [1]. Given the debilitating symptoms associated with GI cancer, assessment and tracking of sequelae are pertinent to patients and care providers. Self-report is typically used to tap into patients’ subjective illness experience and symptoms. Patients’ quality of life (QoL), as well as decisions regarding when to seek 2942 professional help, are primarily driven by presence of such symptoms [2, 3]. Generic symptom and QoL measures may be of some use, but given the diversity of GI cancers and related symptoms, generic measures are considered inferior to the more sensitive measurement of disease-specific changes in symptoms [3]. A tool that measures symptoms specific to a particular cohort of patients can provide essential information regarding patients’ QoL and the efficacy of cancer therapy [3]. Hence, it is critical that researchers and clinicians have access to assessment tools that (1) measure the symptoms that are specific to each GI tumour site and (2) possess sound psychometrics [3]. Over the past two decades, several GI cancer-specific symptom measures have been developed and validated. Currently, an abundance of QoL and symptom measures assessing a variety of patient-reported outcomes exist. This can be overwhelming for researchers and clinicians who wish to select an adequate tool with sound psychometric properties, but who are not specifically trained in psychometrics. A limited set of GI cancer site-specific symptom measures have previously been reviewed. Fan and colleagues [4], as well as Parameswaran and colleages [5] describe four health-related QoL liver and oesophageal cancer measures respectively. However, Fan and colleagues [4] do not provide information on the psychometric properties of the liver cancer measures included in the review, and neither reviews use explicit criteria to recommend certain tools for clinical use in GI cancer patients. To guide researchers and clinicians in their choice of assessment tool, we reviewed all obtainable GI cancer sitespecific symptom measures, describe their domain coverage (i.e. content validity), and report on their reliability and other types of validity. To achieve our goal of providing a relevant, comprehensive, and detailed review, we focus primarily on GI cancers with the highest incidence rates. Measures for these four cancers (colorectal, stomach, liver, and oesophageal) are described separately and presented below from highest to lowest according to their incidence rates. Despite high incidence rates, pancreatic cancer measures were not compared here due to the fact that only two validated symptom measures exist. Methods Study selection The data extraction process was performed according to the guidelines for systematic reviews of diagnostic tests in cancer [6]. MEDLINE (1946 to May 2012) and EMBASE (1980 to May 2012) databases were searched using the OVID interface; CINAHL (1982 to May 2012), and PsycINFO (1972 to Support Care Cancer (2014) 22:2941–2955 May 2012) databases were searched using the EBSCO interface for studies conducted with GI cancer patients. A search template was created in MEDLINE using MeSH and keyword headings (see Appendix 1) and adapted for other databases. The Cochrane Library, as well as the Patient-Reported Outcome and QoL Instruments Database (PROQOLID) were searched for additional publications. After eliminating duplicate studies, the titles, abstracts and full-length articles of identified studies were reviewed independently by two authors (R.P. and K.R.; Fig. 1). Uncertainty about whether or not studies met inclusion criteria was resolved by seeking input from another author (W.L.). Additional validation studies were identified via hand searches of the reference section of already identified papers. Study inclusion and evaluation criteria Only studies of instruments labeled ‘validation studies’, administered by an interview or standardized self-report, and designed or adapted specifically for GI cancer patients were included. We considered measures in all languages, obtained full texts and consulted native speakers when necessary to ensure correct classification and interpretation of relevant studies. We excluded translations of relevant questionnaires into other languages unless they had been systematically revalidated following translation, as merely translating a measure does not lead to new information about the psychometric properties of a particular instrument. Given the considerable complexity and effort required to establish a tools’ reliability and validity, it is critical that reviews use a transparent consensus approach in the adoption of criteria for making value judgements and recommendations. Of particular use for our review was the COSMIN consensus on tool quality for patient-reported outcomes [7, 8], which offers a list of tool properties that reviewers should extract. The COSMIN checklist is particularly useful for the development of new tools that use item response theory (IRT). It could therefore only be partially applied for our review because none of the tools we identified are based on IRT and the full COSMIN checklist asks for details that are available to developers of a new test but are not typically contained in published manuscripts. To maximize the utility of this review, we applied a set of three clearly defined criteria to make transparent and replicable judgments about the perceived quality of a given scale. Using the COSMIN approach [7, 8], as well as research conducted by Streiner and Norman as a guide [8], the three criteria were defined as follows: (1) content validity, operationally defined as relative comprehensiveness of symptom coverage (i.e. a full-scale comprehensiveness score of 4 or above; the detailed rating process is described below), (2) internal consistency (the key index of reliability, scored as poor if < 0.70; adequate if 0.70–0.79, Support Care Cancer (2014) 22:2941–2955 2943 Fig. 1 Literature review flow chart and excellent if ≥ 0.80) [9] and (3) extent of validation (rated on a 1–3 scale, depending on whether one or more samples had been tested and/or whether or not different validation strategies were used). Two authors (R.P. and K.R.) independently rated each scale based on these criteria. Any discrepancies were resolved by re-consulting the relevant article. Details for each measure are offered in Tables 1, 2 and 3 [2, 10–45], which are organized by GI cancer sub-type. It is important to note that these tables list any validation efforts and describe subsequent claims made by the authors regarding the resulting validity of a particular measure. However, due to the variability in quality of validation work performed, the success of each study in adequately validating a measure is assessed in this review using the aforementioned defined criteria, which are outlined in Table 4. Comprehensiveness of symptom coverage To adequately assess comprehensiveness of symptom coverage, four studies were identified that collected relevant data for content validity [2, 10, 16, 28] and that pre-existed resulting publications of the measures themselves. In all of 9 - stomach pain; weight loss; bowel control; digestion; diarrhea; appetite; physical appearance; presence of ostomy 18 - bowel function after sphincter-preserving surgery 14 - lifestyle; coping/behaviour; depression/self-perception; embarassment 9 - energy; pain; weight loss; nausea; diarrhea; swelling or cramps in stomach; appetite; ability to enjoy life; overall QoL Functional Assessment of Cancer Therapy—Colorectal Cancer Subscale (FACT-C) [22] MSKCC Bowel Function Instrument [23] Modified Fecal Incontinence Quality of Life Scale [24] NCCN FACT Colorectal Cancer Symptom Index (FCSI-9) [10] [21] EORTC Colorectal Quality of Life Questionnaire (QLQ-CR29) [20] 29 - micturition problems; abdominal and pelvic pain; defecation problems; fecal incontinence; anxiety; body image; stoma-related problems; sexual items; single items 23 - stomach pain/discomfort; pain in and around anus; change in bowel habits; bowel urgency; incomplete bowel evacuation; mucus in bowel motions; blood from anus; fatigue; weight loss; lump in stomach or anus; low blood count 5 - bowel incontinence; bowel urgency; bowel frequency Adelstein Symptom Scale [18] Bowel Function Questionnaire [19] Number of items - domains covered Scale Table 1 Colorectal cancer symptom measures N=152 patients who had undergone intersphincteric resection for very low rectal cancer with transanal coloanal anastomosis No patient sample N=60 colorectal cancer patients with advanced disease N=156 English and Spanish speaking colorectal cancer patients from the Bilingual Intercultural Oncology Quality of Life project N=127 patients undergoing sphincter-preserving surgery N=351 colorectal cancer patients ICC=0.68 (7–14 days) Not reported r=0.84 (7–14 days) Not reported Range of α from 0.69 to 0.84 for respective subscales Range of α from 0.85 to 0.91 for respective subscales Range of α from 0.75 to 0.79 for respective subscales α=0.95 Not reported Not reported Not reported Not reported Not reported* Not reported Test–retest reliability Not reported Not reported N=263 patients likely to have a colonoscopy N=961 patients recently undergone low anterior resection for rectal cancer N=120 colorectal cancer patients Internal consistency Sample Not reported Concurrent Correlation with MOS SF36, HADS, and WCG Construct Factor analysis Correlation with relevant constructs of the EORTC QLQ-C30, CRC38 and FIQL Criterion Discriminates known groups Construct Correlation with relevant constructs of the FLIC, BPOMS and POMS-SF Criterion Discriminates known groups; responsiveness to clinical change Construct Multitrait Scaling Analysis Developed from previously validated scale Criterion Discriminates known groups; responsiveness to clinical change Not reported Incompletely reported Not reported Validity 2944 Support Care Cancer (2014) 22:2941–2955 a 46 - basic physiological function; sexual function; independence function; emotion; recognition; social support and safety; effect of life and economics 19 - Energy; pain; weight loss; nausea; diarrhea; constipation; swelling or cramps in stomach; numbness/ tingling; appetite; trouble meeting needs of family; sleep; worry; hair loss–bother; bowel control; ability to enjoy life; overall QoL 5 - self-generated items: assess quality of life and extent to which the expectations of patients suffering from rectal cancer are matched by reality Number of items - domains covered Index reported is the wrong estimate for test–retest reliability Quality of Life Instruments for Cancer Patients: Colorectal Cancer (QLICP-CR) [27] Patient Generated Index (PGI) [26] NCCN FACT Colorectal Cancer Symptom Index (NCCN FACT FCSI-19) [2] [25] Scale Table 1 (continued) Not reported N=50 colorectal cancer patients N=11 colorectal cancer patient N=33 rectal cancer patients ICC=0.76 (4 weeks) Range of α from 0.75 to 0.84 for respective subscales N=391 metastatic colorectal cancer patients Not reported r=0.83 (not specified) Not reported Range of α from 0.31 to 0.89 for respective subscales Not reported Test–retest reliability Internal consistency Sample Concurrent Correlation with Chinese version of FACT-C, FACT-G and GLICP-GM Construct Correlation with relevant constructs of the SF-36, QLQ-C30 and QLQ-CR38 Criterion Discriminates known groups; responsiveness to clinical change Not reported Construct Correlation with relevant constructs of the EQ-5D Criterion Discriminates known groups; responsiveness to clinical change Validity Support Care Cancer (2014) 22:2941–2955 2945 Not reported Not reported ICC=0.60 to >0.70 (3–5 days) α=0.90 Not reported N=662 postoperative gastric cancer patients N=221 post-operative esophageal cancer patients N=114 gastric cancer patients 20 - gastroesophageal reflux; deglutition dysfunction; limited activity due to decreased food; diarrhea symptoms; dumping syndrome symptoms; transfer dysfunction; hypoglycemic symptoms 22 - dysphagia; eating restriction; pain; reflux; anxiety; single items Dysfunction after Upper Gastrointestinal Surgery Scale (DAUGS 20) [12-14] Not reported Not reported r=0.73 to 0.89 (1 week) Range of α from 0.72 to 0.80 for respective subscales Not reported Range of α from 0.67 to 0.87 for respective subscales Not reported N=219 gastric cancer patients N=491 esophageal cancer patients N=300 esophageal, gastric, and esophago-gastric junction cancer patients N=65 oesophagus and oesophago-gastric junction cancer patients 18 - dysphagia; deglutition; eating related items; reflux; pain; anxiety 25 - dysphagia; eating restrictions; reflux; odynophagia; pain; anxiety 15 - physical function; activities of daily living; emotional function; social function; symptoms [39] EORTC Oesophageal Cancer Module (QLQ-OES18) [16-17] EORTC Oesophagus, Oesophago-Gastric Junction and Stomach Module (QLQ-OG25) [30] Esophageal Quality of Life Questionnaire (EQOL) [31] EORTC Gastric Cancer Module (QLQ-STO22) [28] Test–retest reliability Internal consistency Sample Number of items - domains covered Scale Table 2 Oesophageal and gastric cancer measures Construct Based on EORTC QLQ-C30 Concurrent Correlates with MOS SF-36 Criterion Responsiveness to clinical change Construct Developed from EORTC QLQ-OES18 and EORTC QLQ-STO22 Correlation analysis with core questionnaire (QLQ-C30) Criterion Discriminates known groups Construct Multitrait scaling analysis: repeated item deletion Developed from EORTC QLQ-OES24 Correlation analysis with core questionnaire (QLQ-C30) Criterion Discriminates known groups Construct Multitrait Scaling Analysis: refined module Correlations with QLQ-C30 Criterion Discriminates known groups; responsiveness to change Not reported Construct Factor analysis Criterion Discriminates known groups Validity 2946 Support Care Cancer (2014) 22:2941–2955 r=0.98 (2–3 days) α=0.91 N=86 stomach cancer patients 39 - disease-specific quality of life Quality of Life Instrument for Patients with Stomach Cancer (QLICP-ST) [36] Attempted but poor validation work ICC=0.88 (2 weeks) α=0.89 N=140 Postoperative gastric cancer patients 17 - physical well-being; mental well-being; digestion; defecation Gastrointestinal Quality of Life Index (C-GIQLI) [35] a ICC=0.88 (2 weeks) Not reported Not reported Not reported α=0.86 19 - physical, functional, emotional and social well-being, and additional concerns (gastric-cancer specific) FACT Gastric cancer subscale (FACT-Ga) [33] Not reported α>0.80 N=83 Oesophageal cancer patients N=82 gastric cancer patients 17 - eating; appetite; swallowing; pain; talking/communicating; mouth dryness; breathing difficulty; coughing; weight loss FACT Esophageal Cancer Subscale (FACT-E) [32] Test–retest reliability Internal consistency Sample [34] Number of items - domains covered Scale Table 2 (continued) Construct Factor analysis Item-own correlation Criterion Responsiveness to clinical change Constructa Factor analysis Correlations with WHOQOL-BREF-HK Construct Correlations with anxiety and depression measures Criterion Discriminates known groups; responsiveness to clinical change Not reported Construct Correlation with relevant EORTC QLQ-30 subscales Criterion Discriminates known groups; responsiveness to clinical change Validity Support Care Cancer (2014) 22:2941–2955 2947 NCCN FACT Hepatobiliary Cancer Symptom Index (NCCN FACT FHSI-18) [2] [10] 18 - energy; pain; weight loss; fatigue; jaundice–bother; ill feelings; nausea; abdominal discomfort; meeting familial needs; appetite; sleep quality; worry; sadness; treatment side effects–bother; ability to do usual activities; overall QoL N=50 hepatobiliary cancer patients Not reported Not reported Not reported r=0.77–0.86 (3–7 days) α=0.79 N=51 hepatobiliary cancer patients NCCN FACT Hepatobiliary Symptom Index (NCCN FACT FHSI-8) [44] 75 - symptoms of liver disease; effects of liver disease; concentration; memory; quality of social interaction; health distress; sleep; loneliness; hopelessness; stigma; sexual functioning/problems 8 - Hepatobiliary specific symptoms and issues (pain; fatigue; nausea; weight loss; jaundice) Not reported Not reported Range of α from 0.63 to 0.91 for respective subscales N=200 patients awaiting liver transplantation Liver Disease Quality of Life Questionnaire (LDQOL 1.0) [43] No patient sample Not reported Range of α from 0.76 to 0.97 for respective subscales N=158 hepatobiliary cancer patients [42] ICC=0.82 (3–7 days) α=0.85 N=51 hepatobiliary cancer patients 18 - abdominal discomfort; weight loss; bowel control; digestion; diarrhea; appetite; physical appearance; back pain; fatigue; constipation; daily activities; jaundice–bother; fevers; itching; change in food taste; chills; dry mouth FACT—Hepatobiliary (FACT-Hep) [41] Not reported Not reported Not reported Range of α from 0.69 to 0.93 for respective subscales ICC=0.64 to 0.87 (1 week) N=158 hepatocellular cancer patients Not reported Not reported Test–retest reliability Range of α from 0.34 to 0.72 for respective subscales 18 - fatigue; body image; jaundice; nutrition; pain; fevers; sexual interest; abdominal swelling and body image EORTC Hepatocellular Carcinoma Module (QLQ-HCC18) [39] N=102 colorectal cancer patients with hepatic metastases N=356 colorectal cancer patients with hepatic metastases Internal consistency N=272 hepatocellular cancer patients 21 - eating; pain; fatigue; relationships; psychosocial; single items EORTC Liver Metastases Colorectal Module (QLQ-LMC21) [37] [38] Sample [40] Number of items - domains covered Scale Table 3 Liver cancer symptom measures Not reported Not reported Construct Significant, negative correlations with POMS. Significant positive correlations with FACTG, and FACT-Hep Criterion Discriminates known groups Construct Relevant scales correlated with PCS and MCS of SF-36 Criterion Discriminates known groups Criterion Discriminates known groups; responsiveness to clinical change Construct Strong negative correlations with POMS, correlation with relevant subscale of ISEL, diverged with MCSDS Criterion Discriminates known groups Construct Multitrait Scaling Analysis Correlation with relevant subscales of QLQ-C30 Criteriona Discriminates known groups; responsiveness to clinical change Not reported Construct Multitrait Scaling Analysis Criterion Discriminates known groups; responsiveness to clinical change Not reported Validity 2948 Support Care Cancer (2014) 22:2941–2955 Table 4 Objectively defined quality criteria Construct Items within each domain converged with one another, and diverged with items of other domains Correlation with relevant domains of the FLIC Criterion Discriminates known groups; responsiveness to clinical change Concurrent Correlation with FACT-G and FACT-Hep Criterion Discriminates known groups Criteria Labels Definition Comprehensiveness Limited Total comprehensiveness score of 3 or below Moderate Total comprehensiveness score of 4 or 5 Internal consistency r=0.71–0.86 (1–2 days) Range of σ from 0.68 to 0.81 for respective subscales N=105 liver cancer patients Total comprehensiveness score of 6 Poor α<0.70 Acceptable α between 0.70 and 0.80 High α>0.80 Limited One sample, one type of validity Moderate One sample, multiple validities Extensive Multiple samples, multiple validities Attempted but poor validation work Reliability a Quality of Life for Patients with Liver Cancer (QOL-LC) [45] [11] Extensive these studies, systematic and comprehensive literature reviews were conducted on symptom prevalence. Further, since ratings of symptom severity and prevalence often vary depending on the source, both patients and health care professionals were consulted [10]. The most important symptoms for each GI cancer subtype were extracted from these studies, and placed into broad symptom classes (Table 5). Given that it is important for a measure to include an adequate amount of broad symptom classes in addition to more specific items, these two criteria were rated separately. When rating broad symptom classes, a score of 3 was given to measures that included ≥ 80% of classes, a score of 2 was given to those that included > 50% (but less than 80%), and a score of 1 was given to those that included ≤ 50%. The same criteria were applied when rating specific items (i.e. a score of 3 to measures that included ≥ 80% of items, a score of 2 to those that included > 50% and a score of 1 to those that included ≤ 50%). After rating each measure on these two criteria, the two scores were aggregated to create a total comprehensiveness score ranging from limited (aggregate score of 3 or less) to extensive (aggregate score of 6) (Table 4). To rate measures that assessed gastric and oesophageal cancer symptoms simultaneously [15, 30], the relevant broad symptom classes and specific items for both of these cancers were amalgamated due to their high overlap. 22 - physical function; psychological function; social function; symptoms/side effects α=0.89 N=50 hepatobiliary cancer patients (stage III and IV) Not reported Internal consistency Number of items - domains covered Scale Table 3 (continued) 2949 Validity Sample Test–retest reliability Validity Support Care Cancer (2014) 22:2941–2955 Reliability was defined as internal consistency, and is reported as Cronbach’s alpha for the full scale and the subscales (whenever possible). Test–retest reliability is also reported to reveal whether a given scale is sensitive to change in longitudinal research and clinical trials. Additionally, two searches were conducted on Health Canada and the US National Institutes of Health clinical trial databases to fully consider data on sensitivity to clinical change of relevant measures that may have been embedded in clinical trials. 2950 Support Care Cancer (2014) 22:2941–2955 Table 5 Relevant broad symptom classes and specific symptoms Colorectal Liver Oesophageal Gastric cancer cancer cancer cancer Bowel-related items Control of bowels X Diarrhea X Pain Abdominal pain/discomfort Abdominal swelling/cramps X X Back pain X X X X Pain/discomfort when eating X Chest pain X General pain X X X X X X Eating-/taste-related items Appetite Blockage when eating X Troublesome eating X X Trouble/change in taste X X Feeling full too quickly X X Trouble with digestion Belching X Reflux X X Heartburn X Trouble with acid/bile X X X X Fatigue Lack of energy X X Feeling fatigued X X Physical appearance Jaundice X Deglutition Being able to swallow saliva X Choking when swallowing X Dysphagia Eating solid foods X Eating soft foods X X X Drinking liquids X X Other symptoms Itching X Nausea X X Weight loss X X X X Results Thirty-six articles reporting on 26 instruments met inclusion criteria (Fig. 1). All identified instruments were self-report; none were based on interview. No disagreements on study inclusion emerged among reviewers. Detailed descriptions of instruments and validation information are listed in alphabetical order in Tables 1, 2 and 3 [2, 10–45]. Based on criteria made explicit in Table 4, we decided to recommend those scales that (1) were rated as at least moderately comprehensive, (2) had a mean internal consistency score of ≥ 0.70 and (3) had been rated as at least moderately well validated. As is apparent in Tables 1, 2 and 3, 22 measures were designed specifically for use in GI cancer patients, whereas 4 [24, 26, 35, 43] were originally developed in non-GI cancer populations, but subsequently validated for GI cancer. It is important to note that all EORTC and FACT questionnaires described below are designed to be administered alongside a more generic QoL questionnaire (EORTC QLQ-C30 and FACT-G, respectively) [46, 47]. Therefore, the comprehensiveness of EORTC and FACT questionnaires were rated accordingly. The following scales met all criteria for scale recommendation: EORTC colorectal module (QLQ-CR29) [20, 21], FACT-C [22], FCSI-9 [10, 25], FHSI-8 [2, 44], FHSI-18, [11, 12], FACT-Hep [41, 42], EORTC liver module (QLQ-LMC21) [37, 38], QoL Instrument for Patients with Liver Cancer (QOL-LC) [45], EORTC QLQ-STO22 [28, 29], FACT-Gastric (FACT-Ga) [33, 34], Dysfunction After Upper Gastrointestinal Surgery (DAUGS-20) [15], FACT-esophageal (FACT-E) [32] and the EORTC QLQ-OG25 [30]. Among these recommended scales, five stood out as having particularly strong psychometric properties, namely, the FACT-C, FCSI-9, FHSI18, FACT-Hep and the EORTC QLQ-STO22. No further data on sensitivity to change were found through our literature search of Health Canada and the US National Institutes of Health clinical trial databases on GI cancer clinical trials. Below, unique characteristics and applications for some of the scales are described to reveal idiosyncratic strengths weaknesses that are not contained in a quantitative evaluation alone. Validity Colorectal cancer Given the purpose and environment in which symptom measures are typically developed, the assumption was made that all symptom measures included in this review would have face validity and at least some content validity. Thus, in addition to describing domain coverage, we focused on the description and evaluation of construct, concurrent, and criterion validity for each respective measure. Ten symptom measures validated in 13 studies have been created for use amongst colorectal cancer patients. Measures relevant for all colorectal cancer patients Five measures (Table 1) have been validated in colorectal cancer patients, regardless of disease stage or treatment. The Support Care Cancer (2014) 22:2941–2955 EORTC QLQ-CR29 [20, 21] and FACT-C [22] are two of the most widely used symptom measures because of their modular approach. Although more comprehensive than the revised scale, the original version of the EORTC QLQ-CR29 was not included in the present review because it is no longer in use [48, 49]. The most recent version of the EORTC QLQ-CR29 is available in 16 languages. The FACT-C was designed for use in clinical trials and clinical practice evaluation and is available in 36 languages. Adelstein’s symptom scale [18] is a self-administered questionnaire developed to assess the presence, severity and type of lower bowel symptoms that may be indicative of colorectal cancer. This scale is designed for use in both research and clinical settings. While the Patient Generated Index (PGI), a general QoL measure, was not developed specifically for colorectal cancer patients, it has been validated in pre-operative patients with rectal cancer [26]. The PGI is unique in that it assesses patient symptomatology and QoL in three stages. In the first stage, patients are asked to list up to five areas of their lives that have been affected by cancer. In the second stage, patients are asked to rate how current health reality meets their expectations. In the third stage, patients assign a total of 14 imaginary points to areas of their life they wish they could improve. Due to the selfgenerated nature of the questionnaire, an objective assessment of its comprehensiveness could not be completed. However, comprehensiveness based on the content areas included are comparable to those of the FCSI-19 [2]. The Quality of Life Instruments for Cancer PatientsColorectal Cancer (QLICP-CR) [27] was designed to assess various aspects of QoL related to colorectal cancer. We were unable to access the full copy of the original Chinese questionnaire, which precluded adequate assessment of the scale’s comprehensiveness. However, the journal article was translated by a bilingual Chinese individual, who helped extract important information regarding relevant psychometric properties of the tool. Stage and treatment-specific measures Five measures (Table 1) have been validated in either patients with advanced disease stage or patients receiving surgery or chemotherapy for colorectal cancer. Both the NCCN FACT FCSI-9 [10, 25] and the NCCN FACT FCSI-19 [2] were designed for advanced stage colorectal patients receiving chemotherapy. The FCSI-9 is a short, very comprehensive and internally consistent scale. The more recent version of the FCSI-9, the FCSI-19, is even more comprehensive, yet no information on the scale’s internal consistency and extent of validation is currently 2951 available. In contrast to one translation of the FCSI-19, the FCSI-9 exists in 28 languages. Three measures have been developed in postoperative patients who have undergone surgery for colorectal cancer (Table 1). Among these, the Memorial Sloan–Kettering Cancer Center Bowel Function Instrument (MSKCC-BFI) [23] was designed for use in colorectal cancer patients who underwent sphincter-preserving surgery. Due, in part, to its specific application, this measure is limited with respect to comprehensiveness. Similar to the MSKCC-BFI, the Modified Fecal Incontinence Quality of Life Scale [24] was developed for use in postoperative patients who underwent intersphincteric resection. The Bowel Function Questionnaire [19] was developed to assess bowel dysfunction after surgery for rectal cancer. The scale has several weaknesses including lack of comprehensiveness, no reported internal consistency and limited validation no reported internal consistency and limited validation efforts. Gastric cancer Five symptom measures (Table 2) have been created for use amongst gastric cancer patients. Measures relevant for all gastric cancer types Three measures (Table 2) have been created for use. As with colorectal cancer measures, the EORTC QLQ-STO22 [28, 29] and the FACT-Ga [33, 34] are the most widely used measures. Both the FACT-Ga (available in 28 languages) and the EORTC QLQ-STO22 (available in 38 languages) are comprehensive measures. While the FACT-Ga has a higher overall internal consistency and includes questions about functional and social/family well-being, the EORTC QLQ-STO22 contains more specific symptom-related items. The Quality of Life Instrument-Stomach Cancer (QLICPST) [36] was developed to assess aspects of QoL related to stomach cancer. Given that the original Chinese questionnaire was not retrievable, we were unable to assess the scale’s comprehensiveness. Treatment-specific measures Two measures (Table 2) were developed for patients receiving particular treatments for gastric cancer. The Chinese Gastrointestinal Quality of Life Index (CGIQLI) [35] is a culturally adapted version of the Gastrointestinal Quality of Life Index. The original scale was developed for use in patients with gastrointestinal problems; however, Yeung and colleagues [35] validated the scale in postoperative gastric cancer patients. While the measure’s 2952 internal consistency is adequate, its extent of validation and comprehensiveness is limited. The DAUGS-20 [15] was developed to assess postoperative QoL in gastric and oesophageal cancer patients who have previously undergone upper GI tract surgery. The older version of the DAUGS-20 [12–14] was not included here because it is a precursor to the current version and no longer in use. The DAUGS-20 is a comprehensive measure with high internal consistency. Liver cancer Seven symptom measures (Table 3) have been created for use amongst liver cancer patients. Both the EORTC QLQ-HCC18 [39, 40] and FACT-Hep [41, 42] are widely used measures. However, despite its use in research and clinical trials, the EORTC QLQ-HCC18 (available in 23 languages) is not comprehensive, and no extant data is available on sensitivity to change. The FACT-Hep is available in 40 languages. It is more comprehensive than the EORTC QLQ-HCC18, has excellent internal consistency and has been extensively validated. The EORTC QLQ-LMC21 [38] is the only scale specifically developed for patients with liver metastases from colorectal cancer and is available in five languages. Both the NCCN FACT FHSI-8 [2, 45] and FHSI-18 [11, 12] evaluate response to chemotherapy for patients with advanced disease. Despite the limited validation efforts for the FHSI-8, the scale is concise, comprehensive and internally consistent. The more recent version of the FHSI-8 (the FHSI-18) has a higher internal consistency and underwent careful development. Items endorsed at a greater frequency by both experts and patients were retained to create a very comprehensive symptom index. Although the FHSI-18 has not been translated, the FHSI-8 is available in 31 languages. The QOL-LC [45] is a Chinese-specific measure that takes cultural background into account. The Liver Disease Quality of Life Questionnaire (LDQOL 1.0) [43] was originally developed for use in patients with several types of liver disease. Recently, a Spanish version has been validated in patients awaiting liver transplantation. The LDQOL 1.0 has several limitations including length (mean completion time of 36 min precludes use in many settings), modest validity and poor comprehensiveness. Oesophageal cancer Four symptom measures (Table 2) have been developed for use amongst oesophageal cancer patients. Support Care Cancer (2014) 22:2941–2955 The EORTC oesophageal module (QLQ-OES18) [16, 17] EORTC QLQ-OG25 [30] and FACT-E [32] are all widely used measures. The EORTC QLQ-OES18 (available in 23 languages) is very comprehensive, but internal consistency and validity are insufficient. The EORTC QLQ-OG25 was developed for use amongst gastric, oesophageal and esophago-gastric junction patients, a n d c o m b i n e s t h e E O RT C Q L Q - O E S 1 8 a n d E O RT C Q L Q - S T O 2 2 [ 2 8 , 2 9 ] . A l t h o u g h t h e EORTC QLQ-OG25 (available in 11 languages) is very similar to the EORTC QLQ-OES18, it covers more key content than other oesophageal cancer measures [5]. It is internally consistent, and more extensively validated than the EORTC QLQ-OES18. The FACT-E (available in 16 languages) assesses symptoms of oesophageal cancer for use in clinical trials and clinical practice. While the FACT-E is slightly less comprehensive than the EORTC QLQ-OES18, its internal consistency is excellent. The Esophageal Quality of Life Questionnaire (EQOL) [31] determines QoL associated with curative treatment modalities in oesophageal cancer patients, and is meant to be used in conjunction with the EORTC QLQ-C30 [46]. Despite established validity of the scale, it is limited with respect to comprehensiveness, and no data exists on internal consistency. Other measures Another six measures validated in six studies [3, 50–54] were not extensively analyzed because the focus of this review is GI cancer subtypes with high incidence rates. Two of these measures were designed as general GI cancer symptom measures (scale name not specified [3] and the MD Anderson Symptom Inventory [51]). One measure was developed to assess health-related QoL amongst patients with cholangiocarcinoma and gallbladder cancer (EORTC QLQ-BIL21) [53]. Another measure assesses health-related QoL in patients with GI neuroendocrine tumours (EORTC QLQ-GINET21) [52]. A further two measures have been validated in pancreatic cancer patients (i.e., the EORTC QLQ-PAN26 and the GIQLI [50, 54]). Promising tools and further recommendations This systematic review identified 26 scales that met inclusion criteria. Thirteen of these scales were considered to have sufficiently good psychometric properties to permit recommendation for use, and five stood out as having the strongest psychometric properties. The respective modules of the FACT and EORTC QoL scales, (i.e., the FACT-C [22], EORTC QLQ STO-22 [28, 29], FACT-Hep [41, 42] and EORTC QLQ OG- Support Care Cancer (2014) 22:2941–2955 25 [30]), were rated as best for the major GI cancer sites investigated. Furthermore, for symptom assessment with advanced colorectal or liver cancer, the FCSI-9 [10, 25] and FHSI-18 [11, 12] are adequate tool options. All of the recommended tools were developed within the last 13 years and several represent revisions of earlier versions. With respect to colorectal cancer measures, it is important to note that both the PGI [26] and the QLICP-CR [27] were only validated in very small samples (n=33 and n=11, respectively). Thus, these measures may benefit from further validation in larger samples. With respect to hepatological cancer measures, note that despite the modular approach adopted by the EORTC QoL group, the EORTC QLQHCC18 [39, 40] should be revised and re-validated. While the C-GIQLI [35] is comprehensive, further validation is recommended in other populations due to its culturally sensitive nature. Similarly, the DAUGS-20 [15], a gastric cancerspecific questionnaire with sound psychometrics, is in need of further cross-cultural validation, as its use is currently limited to Japanese patients. In terms of oesophageal cancer measures, our conclusions are not significantly different from Parameswaran and colleagues [5], but additional recommendations and more detailed analysis of psychometric properties are added to the literature here. When it comes to clinical practice recommendations, the focus of this review on symptom measures should not prevent researchers from adding generic measures of QoL, distress, pain, sleep problems, etc., to their study, depending on the research and/or clinical question. There is no singular gold standard with which to rate multidimensional tools; in each case, choosing a tool requires checking whether it has been validated for the intended sample and context. Several weaknesses were apparent across multiple instruments included in this review. Repeatedly, we observed that new tools were developed and applied to a clinical study with minimal, if any, validation work. Some questionnaires contained subscales with low internal consistency but no effort was made to improve on these measures with additional test development work. This criticism does not apply to the recommended measures. Importantly, 10 out of 26 measures (Tables 1, 2 and 3) were not determined as sensitive to clinical change. Thus, an area of scale improvement represents the analysis of sensitivity to change with longitudinal data. This criticism applies to three recommended measures (EORTC QLQ OG-25 [30], FHSI-18 [11, 12] and FCSI-19 [2]). However, it is likely due to the recency of tool development that no extant data on sensitivity to change is currently available for the FHSI-18 and FCSI-19. Conclusion In summary, a considerable number of GI cancer site-specific symptom measures with good psychometric properties have 2953 been identified, with submodules of the FACT being the best tool choice for most cancer types. Further improvement of already existing, promising measures is recommended. Disclosures and acknowledgments No funding was received for this manuscript. None of the authors are in any financial or personal conflict of interest regarding this work. We are very grateful for the feedback of Dr. Jessica McAlpine on an earlier draft of this manuscript. References 1. Canadian Cancer Society’s Advisory Committee on Cancer Statistics (2013) Canadian Cancer Statistics. Canadian Cancer Society. http:// www.cancer.ca/statistics 2. Cella D, Rosenbloom SK, Beaumont JL et al (2011) Development and validation of eleven symptom indexes to evaluate response to chemotherapy for advanced cancer. J Natl Compr Cancer Netw 9: 269–278 3. Wang XS, Williams LA, Eng C et al (2010) Validation and application of a module of the M. D. Anderson Symptom Inventory for measuring multiple symptoms in patients with gastrointestinal cancer (the MDASI-GI). Cancer 116:2053–2063 4. Fan S, Eiser C, Ho MC (2010) Health-related quality of life in patients with hepatocellular carcinoma: a systematic review. Clin Gastroenterol Hepatol 8:550–564 5. Parameswaran R, Clifton, JC, Blazeby JM (2010) Quality of life measures in patients with esophageal cancer. In: Handbook of disease burdens and quality of life measures. Springer, New York, pp 2796– 807 6. Mallet S, Deeks JJ, Halligan S et al (2006) Systematic reviews of diagnostic tests in cancer: reviews of methods and reporting. BMJ. doi:10.1136/bmj.38895.467130.55 7. Mokkink LB, Terwee CB, Patrick DL et al (2010) The COSMIN checklist assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res 19:539–549 8. Mokkink LB, Terwee CB, Gibbons E et al (2010) Inter-rater agreement and reliability of the COSMIN (Consensus-based standards for the selection of health status measurement instruments) Checklist. BMC Med Res Methodol 10:82 9. Streiner DL, Norman GR (2008) Health measurement scales: a practical guide to their development and use. Oxford University Press, New York 10. Cella D, Paul D, Yount S et al (2003) What are the most important symptom targets when treating advanced cancer? A survey of providers in the national comprehensive cancer network. Cancer Investig 21:526–535 11. Butt Z, Parikh ND, Beaumont JL et al (2012) Development and validation of a symptom index for advanced hepatobiliary and pancreatic cancers. Cancer. doi:10.1002/cncr.27588 12. Nakamura M, Kido Y, Yano M, Hosoya Y (2005) Reliability and validity of a new scale to assess postoperative dysfunction after resection of upper gastrointestinal carcinoma. Surg Today 35:535– 542 13. Nakamura M, Kido Y, Egawa T (2008) Development of a 32-item scale to assess postoperative dysfunction after upper gastrointestinal cancer resection. J Clin Nurs 17:1440–1449 14. Nakamura M, Hosoya Y, Yano M et al (2011) Extent of gastric resection impacts patient quality of life: the Dysfunction After Upper Gastrointestinal Surgery for Cancer (DAUGS32) scoring system. Ann Surg Oncol 18:314–320 2954 15. Nakamura M, Hosoya Y, Umeshita K et al (2011) Postoperative quality of life: development and validation of the “Dysfunction After Upper Gastrointestinal Surgery” scoring system. J Am Coll Surg 213:508–514 16. Blazeby JM, Alderson D, Winstone K et al (1996) Development of an EORTC questionnaire module to be used in quality of life assessment for patients with oesophageal cancer. The EORTC Quality of Life Study Group. Eur J Cancer 32A:1912–1917 17. Blazeby JM, Conroy T, Hammerlid E et al (2003) Clinical and psychometric validation of an EORTC questionnaire module, the EORTC QLQ-OES18, to assess quality of life in patients with oesophageal cancer. Eur J Cancer 39:1384–1394 18. Adelstein BA, Irwig L, Macaskill P et al (2008) A self administered reliable questionnaire to assess lower bowel symptoms. BMC Gastroenterol. doi:10.1186/1471-230X-8-8 19. Emmertsen KJ, Laurberg S (2012) Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg 255:922–928 20. Gujral S, Conroy T, Fleissner C et al (2007) Assessing quality of life in patients with colorectal cancer: an update of the EORTC quality of life questionnaire. Eur J Cancer 43:1564–1573 21. Whistance RN, Conroy T, Chie W et al (2009) Clinical and psychometric validation of the EORTC QLQ-CR29 questionnaire module to assess health-related quality of life in patients with colorectal cancer. Eur J Cancer 45:3017–3026 22. Ward WL, Hahn EA, Mo F et al (1999) Reliability and validity of the Functional Assessment of Cancer Therapy-Colorectal (FACT-C) quality of life instrument. Qual Life Res 8:181–195 23. Temple LK, Bacik J, Savatta SG et al (2005) The development of a validated instrument to evaluate bowel function after sphincterpreserving surgery for rectal cancer. Dis Colon Rectum 48:1353– 1365 24. Hashimoto H, Shiokawa H, Funahashi K et al (2010) Development and validation of a modified fecal incontinence quality of life scale for Japanese patients after intersphincteric resection for very low rectal cancer. J Gastroenterol 45:928–935 25. Colwell HH, Mathias SD, Turner MP et al (2010) Psychometric evaluation of the FACT Colorectal Cancer Symptom Index (FCSI9): reliability, validity, responsiveness, and clinical meaningfulness. Oncologist 15:308–316 26. Camilleri-Brennan J, Ruta DA, Steele RJ (2002) Patient generated index: new instrument for measuring quality of life in patients with rectal cancer. World J Surg 26:1354–1359 27. Yang Z, Lu YB, Wan CH et al (2008) Development of the system of quality of life instruments for cancer patients: colorectal cancer (QLICP-CR). Aizheng 27:96–100 28. Vickery CW, Blazeby JM, Conroy T et al (2001) Development of an EORTC disease-specific quality of life module for use in patients with gastric cancer. Eur J Cancer 37:966–971 29. Blazeby JM, Conroy T, Bottomley A et al (2004) Clinical and psychometric validation of a questionnaire module, the EORTC QLQ-STO22, to assess quality of life in patients with gastric cancer. Eur J Cancer 40:2260–2268 30. Lagergren P, Fayers P, Conroy T et al (2007) Clinical and psychometric validation of a questionnaire module, the EORTC QLQOG25, to assess health-related quality of life in patients with cancer of the oesophagus, the oesophago-gastric junction and the stomach. Eur J Cancer 43:2066–2073 31. Clifton JC, Finley RJ, Gelfand G et al (2007) Development and validation of a disease-specific quality of life questionnaire (EQOL) for potentially curable patients with carcinoma of the esophagus. Dis Esophagus 20:191–201 32. Darling G, Eton DT, Sulman J, Casson AG, Celia D (2006) Validation of the functional assessment of cancer therapy esophageal cancer subscale. Cancer 107:854–863 Support Care Cancer (2014) 22:2941–2955 33. Eremenco SL, Cashy J, Webster K et al (2004) FACT-Gastric: a new international measure of QOL in gastric cancer. J Clin Oncol 22:8123 34. Garland SN, Pelletier G, Lawe A et al (2011) Prospective evaluation of the reliability, validity, and minimally important difference of the functional assessment of cancer therapy–gastric (FACT-Ga) qualityof-life instrument. Cancer 117:1302–1312 35. Yeung SM, Shiu AT, Martin CR, Chu KM (2006) Translation and validation of the Chinese version of the Gastrointestinal Quality of Life Index in patients with gastric tumor. J Psychosom Res 61:469– 477 36. Meng Q, Wan CH, Luo JH et al (2008) Development of the system of quality of life instruments for cancer patients: stomach cancer (QLICP-ST). Aizheng 27:1212–1216 37. Kavadas V, Blazeby JM, Conroy T et al (2003) Development of an EORTC disease-specific quality of life questionnaire for use in patients with liver metastases from colorectal cancer. Eur J Cancer 39: 1259–1263 38. Blazeby JM, Fayers P, Conroy T et al (2009) European Organization for Research Treatment of Cancer (EORTC) Quality of Life Group. Validation of the European Organization for Research and Treatment of Cancer QLQ-LMC21 questionnaire for assessment of patientreported outcomes during treatment of colorectal liver metastases. Br J Surg 96:291–298 39. Blazeby JM, Currie E, Zee BC et al (2004) Development of a questionnaire module to supplement the EORTC QLQ-C30 to assess quality of life in patients with hepatocellular carcinoma, the EORTC QLQ-HCC18. Eur J Cancer 40:2439–2444 40. Chie WC, Blazeby JM, Hsiao CF et al (2012) International crosscultural field validation of an European Organization for Research and Treatment of Cancer questionnaire module for patients with primary liver cancer, the European Organization for Research and Treatment of Cancer quality-of-life questionnaire HCC18. Hepatology 55:1122–1129 41. Heffernan N, Cella D, Webster K et al (2002) Measuring healthrelated quality of life in patients with hepatobiliary cancers: the Functional Assessment of Cancer Therapy—Hepatobiliary questionnaire. J Clin Oncol 20:2229–2239 42. Steel JL, Eton DT, Cella D, Olek MC, Carr BI (2006) Clinically meaningful changes in health-related quality of life in patients diagnosed with hepatobiliary carcinoma. Ann Oncol 17:304–312 43. Casanovas T, Jane L, Herdman M et al (2010) Assessing outcomes in liver disease patients: reliability and validity of the Spanish version of the Liver Disease Quality of Life Questionnaire (LDQOL 1.0). Value Health 13:455–462 44. Yount S, Cella D, Webster K et al (2002) Assessment of patientreported clinical outcome in pancreatic and other hepatobiliary cancer: the FACT Hepatobiliary Symptom Index. J Pain Symptom Manag 24:32–44 45. Wan C, Fang J, Yang Z et al (2010) Development and validation of a quality of life instrument for patients with liver cancer QOL-LC. Am J Clin Oncol 33:448–455 46. Aaronson NK, Ahmedzai S, Bergman B et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality of life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–376 47. Cella DF, Tulsky DS, Gray G et al (1993) The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol 11:570–579 48. Sprangers MA, te Velde A, Aaronson NK (1999) The construction and testing of the EORTC colorectal cancer-specific quality of life questionnaire module (QLQ-CR38). European Organization for Research and Treatment of Cancer Study Group on Quality of Life. Eur J Cancer 35:238–247 49. Uwer L, Rotonda C, Guillemin F et al (2011) Responsiveness of EORTC QLQ-C30, QLQ- CR38 and FACT-C quality of life Support Care Cancer (2014) 22:2941–2955 questionnaires in patients with colorectal cancer. Health Qual Life Out. doi:10.1186/1477-7525-9-70 50. Bassi C, Johnson C, Fitzsimmons D et al (1999) Quality of life assessment in pancreatic carcinoma: results of an European multicentric study. Chir Ital 51:359–366 51. Chisholm EM, De Dombal FT, Giles GR (1985) Validation of a selfadministered questionnaire to elicit gastrointestinal symptoms. Br Med J 290:1795–1796 52. Davies A, Larsson G, Ardill J et al (2006) Development of a disease-specific quality of life questionnaire module for 2955 patients with gastrointestinal neuroendocrine tumours. Eur J Cancer 42:477–484 53. Friend E, Yadegarfar G, Byrne C et al (2011) Development of a questionnaire (EORTC module) to measure quality of life in patients with cholangiocarcinoma and gallbladder cancer, the EORTC QLQBIL21. Br J Cancer 104:587–592 54. Nieveen Van Dijkum EJ, Terwee CB et al (2000) Validation of the gastrointestinal quality of life index for patients with potentially operable periampullary carcinoma. Br J Surg 87: 110–115