Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
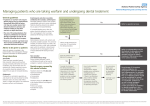
Warfarin Initiation Guidelines CONTRAINDICATIONS: o o o Active major bleeding Recent or planned epidural or dural anesthesia (see epidural-anticoagulation guidelines) Pregnancy (Check HCG if female) CAUTIONS: o o o o o o o o o Known bleeding diathesis 3 Thrombocytopenia (platelet count less than 100,000/mm ); suspected active heparin induced thrombocytopenia (HIT) Recent internal bleeding or uncontrollable active bleeding (hospital admission or transfusion in last 30 days) Recent (within the previous 2 weeks) surgery, major trauma or thrombotic stroke History of intracranial hemorrhage Acute peptic ulcer disease Alcoholism Unsupervised Dementia High risk of noncompliance Major Orthopedic Surgery INR Target Range 1.8-2.5 (Patients at high risk of bleeding) Pre-Op Dose (evening prior to surgery day): 7.5 mg (less than 75 years old); 5 mg (greater than or equal to 75 years old) Post-Op Dose (Day of Surgery): 3-4 mg as soon as tolerating PO post-operatively and hemodynamically stable INR VALUE Post-Op days 1&2 Post-Op Day 3 Post-Op Day 4* Post-Op Day ≥5* <1.4 3-4 mg 5-6 mg 6-7.5 mg 7.5-10 mg 1.4-1.7 2-3 mg 3-4 mg 3-6 mg 4-7.5 mg 1.8-2.1 1-2 mg 1-3 mg 1-5 mg 1-6 mg 2.1-2.5 Hold Dose 1-2 mg 1-3 mg 1-4 mg For INR 2.5-3: Hold x1 day (consider re-drawing INR if increased at least 1 from previous day’s INR) For INR 3.1-4: Hold x1 day, re-draw INR in 5-6 hours; consider 1.25-2.5mg PO Vitamin K x1. For INR greater than 4: CALL MD, Hold x1 day, re-draw INR in 5-6 hours; consider 1.25-5mg PO Vitamin K x1 *For those who have reached a stable INR give the lowest dose in the dosage range Major Orthopedic Surgery INR Target Range 2 - 3 Pre-Op Dose (evening prior to surgery day): 7.5 mg (less than 75 years old); 5 mg (greater than or equal to 75 years old) Post-Op Dose (Day of Surgery): 5 mg as soon as tolerating PO post-operatively and hemodynamically stable INR VALUE Post-Op days 1&2 Post-Op Day 3 Post-Op Day 4* Post-Op Day ≥5* <1.4 5 mg 5-7.5mg 7.5-10 mg 8-12 mg 1.4-1.7 4 mg 3-5 mg 5-7.5 mg 7.5-10 mg 1.8-2.1 3 mg 2-4 mg 3-5 mg 5-7.5 mg 2.1-3 1-2 mg 1-3 mg 2-4 mg 2-5 mg For INR 3-3.2: Hold x1 day (consider re-drawing INR if increased at least 1 from previous day’s INR) For INR 3.3-4: Hold x1 day, re-draw INR in 5-6 hours, consider 1.25-2.5mg PO Vitamin K x1. For INR greater than 4: CALL MD, Hold x1 day, re-draw INR in 5-6 hours; consider 1.25-5mg PO Vitamin K x1 *For those who have reached a stable INR give the lowest dose in the dosage range These are intended to be a guide to common clinical circumstances, and may not apply to certain patients and situations. The treating clinician must use judgment in application of guidelines to the care of individual patients. Page 1 JC Anticoagulation Task Force 7/16/13 Inpatient Initiation (Non-Orthopedic Indications, e.g. atrial fibrillation, mechanical valve, or venous thromboembolism) o o o o o These nomograms are useful in hospitalized patients in whom INR can be checked on a daily basis. Initiation strategies using 10 mg warfarin doses have been tested in randomized trials and are supported in published guidelines. Practitioners experienced in anticoagulation initiation may choose to use a 10mg initiation protocol in appropriately selected patients. The 10 mg initiation should only be used in relatively young and healthy patients who are likely to be insensitive to warfarin, or in patients taking concurrent medications known to induce warfarin metabolism. The 5 mg initiation dose should be used in most patients. Lower initiation doses may be considered in the presence of factors that may make patients more sensitive to warfarin: age greater than 75 years clinical congestive heart failure diarrhea drug interactions (e.g. concurrent drugs that inhibit warfarin metabolism) elevated baseline INR fever hyperthyroidism malignancy Please note that loading doses of warfarin are NOT RECOMMENDED. INR Target Range 2 - 3 Day 1 2 3 4 5 6 5 mg INITIATION INR DOSE – 5 mg < 1.5 5 mg 1.5-1.9 2.5 mg 2 – 2.5 1 - 2.5 mg > 2.5 0 < 1.5 5-10 mg 1.5-1.9 2.5 – 5 mg 2 – 2.5 0 - 2.5 mg 2.5 - 3 0 - 2.5 mg >3 0 < 1.5 10 – 12.5 mg 1.5-1.9 5 - 7.5 mg 2-3 0 – 5 mg >3 0 < 1.5 10 – 15 mg 1.5-1.9 7.5 – 10 mg 2-3 0 – 5 mg >3 0 < 1.5 10 – 15 mg 1.5-1.9 5 – 10 mg 2-3 0 - 7.5 mg >3 0 INR Target Range 2.5-3.5 Day 1 2 3 4 5 6 5 mg INITIATION INR DOSE – 5 mg < 1.7 5 mg 1.8-2.1 2.5 mg 2.2-2.9 1 - 2.5 mg > 2.9 0 < 1.7 5-10 mg 1.8-2.1 2.5 – 5 mg 2.2-2.9 0 - 2.5 mg 3 -3.4 0 - 2.5 mg > 3.4 0 < 1.7 10 – 12.5 mg 1.8-2.4 5 - 7.5 mg 2.5-3.5 0 – 5 mg > 3.5 0 < 1.7 10 – 15 mg 1.8-2.4 7.5 – 10 mg 2.5-3.5 0 – 5 mg > 3.5 0 < 1.7 10 – 15 mg 1.8-2.4 5 – 10 mg 2.5-3.5 0 - 7.5 mg > 3.5 0 These are intended to be a guide to common clinical circumstances, and may not apply to certain patients and situations. The treating clinician must use judgment in application of guidelines to the care of individual patients. Page 2 JC Anticoagulation Task Force 7/16/13 Outpatient Initiation o o o These nomograms are useful in outpatients in whom INR checks can be performed with less frequency. Initiation strategies using 10 mg warfarin doses have been tested in randomized trials and are supported in published guidelines. Practitioners experienced in anticoagulation initiation may choose to use a 10mg initiation protocol in appropriately selected patients. The 10 mg initiation should only be used in relatively young and healthy patients who are likely to be insensitive to warfarin, or in patients taking concurrent medications known to induce warfarin metabolism. Consider using the Sensitive Patients nomogram in the following situations: age greater than 75 clinical congestive heart failure diarrhea drug interactions (e.g. concurrent drugs that inhibit warfarin metabolism) elevated baseline INR fever hyperthyroidism malignancy malnutrition or NPO greater than 3 days INR Target Range 2 - 3 Sensitive Patients Non-Sensitive Patients 2.5 mg Daily 5 mg Daily Initial Dose 3 days 3 days First INR 5 mg Daily 7.5 mg Daily < 1.5 2.5 mg Daily 5 mg Daily 1.5 - 1.9 1.25 mg Daily 2.5 mg Daily 2-3 0.5 mg Daily 1.25 mg Daily 3.1-4 Hold hold >4 2 to 3 days 2 to 3 days Next INR Cycle is repeated until in-range INR achieved on 2 measurements. INR Target Range 2.5-3.5 Sensitive Patients Non-Sensitive Patients 2.5 mg Daily 5 mg Daily Initial Dose 3 days 3 days First INR 5 mg Daily 7.5 mg Daily < 1.7 2.5 mg Daily 5 mg Daily 1.8 – 2.4 1.25 mg Daily 2.5 mg Daily 2.5-3.5 0.5 mg Daily 1.25 mg Daily 3.6-4.4 hold hold >4.4 2 to 3 days 2 to 3 days Next INR Cycle is repeated until in-range INR achieved on 2 measurements. These are intended to be a guide to common clinical circumstances, and may not apply to certain patients and situations. The treating clinician must use judgment in application of guidelines to the care of individual patients. Page 3 JC Anticoagulation Task Force 7/16/13 Post-Initiation Monitoring o o o Inpatient method: Daily through day 4, then every 3-5 days. After hospital discharge: If stable: Within 3-5 days. If unstable: Within 1-3 days. Outpatient method: Within 1 week following second in-range INR. First month of therapy: At least weekly. Thereafter use [Warfarin Maintenance Guidelines] Venous Thromboembolism – Special Considerations • • • Warfarin may be started on the first treatment day, following administration of parenteral anticoagulant (unfractionated heparin, low-molecular weight heparin, pentasaccharide) The parenteral anticoagulant should be overlapped with warfarin until: o 5 days of parenteral anticoagulant have been administered AND o INR has been > 2.0 for at least 24 hours Outpatient treatment of deep vein thrombosis should not be performed unless significant infrastructure exists to assure close follow-up of anticoagulant initiation. Atrial Fibrillation – Special Considerations • For special consideration on choosing an anticoagulant for atrial fibrillation, assessing clot and bleeding risk and other factors, please see Atrial Fibrillation Care Process Model (CPM). Patients on Chronic Warfarin – Hospital Monitoring o o o Patients on chronic warfarin therapy are often admitted to the hospital for other medical conditions. Due to changes in patient condition, diet, medications and other factors during hospitalization, frequent monitoring of warfarin during hospitalization is necessary. The following labs are recommended if the patient is admitted on warfarin and the warfarin is continued during hospitalization: On Admit: Baseline INR on admission to the hospital Continuing on Warfarin: INR every 3-5 days while in hospital If changes are made to warfarin dose, interacting medications are added, or patient status indicates, more frequent monitoring of INR (e.g. every 1-3 days) may be needed If chronic warfarin therapy is discontinued during hospitalization for surgery or procedures, follow bridging guidelines Developed by Anticoagulation Task Force - System-wide P&T Approval 9/17/08 - Updated 3/3/09 These are intended to be a guide to common clinical circumstances, and may not apply to certain patients and situations. The treating clinician must use judgment in application of guidelines to the care of individual patients. Page 4 JC Anticoagulation Task Force 7/16/13