Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Glossary of psychiatry wikipedia , lookup
Abnormal psychology wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Emil Kraepelin wikipedia , lookup
Mental status examination wikipedia , lookup
Parkinson's disease wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Antipsychotic wikipedia , lookup
Alzheimer's disease wikipedia , lookup
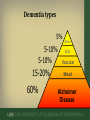
Dementia: Clinical Challenges Outline • • • • Background Dementia medications Nutrition Agitation Background Dementia is frequently overlooked • Early symptoms attributed to normal aging • Physicians don’t detect early changes • Physicians do detect changes but don’t document them because – – – – Not confident in dementia care? Don’t consider it a true medical problem? Not enough time to deal with it? Want to avoid stigmatizing patients? Sternberg SA et al. JAGS, 2000; Boustani M. et al. JGIM, 2005 Dementia Defined • Decline in cognitive function from baseline Epidemiology • In the US population Over 65: Over 85: 5-10% 30-50% Gauthier S et al. Lancet 2006. 376: 1262-1270. Kennedy, GJ. Geriatric Medicine, 4th Ed. Cassel et al, Eds. 2003, p.1079 Screening • Mini Mental State Examination • St. Louis University Mental State Examination • Montreal Cognitive Assessment tool • MiniCog Diagnostic criteria Decline in 2 of the following 5 domains: 1. Memory 2. Language 3. Visuospatial skills 4. Handling complex tasks 5. Judgment/reasoning Rule out delirium, psychiatric disorders Symptoms represent a decline from baseline Symptoms result in a decline in function Knopman DS. Mayo Clin Proc. Feb 2006; 81(2):223-230. Workup • History & physical examination with a complete neurologic exam • Comprehensive Metabolic Panel, Complete Blood Count, Vitamin B12, Thyroid Function Tests, possibly also Vitamin D, Rapid Plasma Reagin and HIV • Brain imaging if appropriate • Neuropsychological testing if appropriate Dementia types 5% 5-10% 5-10% 15-20% 60% Other DLB Vascular Mixed Alzheimer Disease Mild Cognitive Impairment (MCI) • Subjective change in cognition • Objective findings of impairment in one or more cognitive domains • Minimal interference with function • In the US population over 65: 3-19% Albert MS et al. Alzheimer’s & Dementia 2011; Gauthier S et al. Lancet 2006 Alzheimer Disease • New diagnostic criteria published in 2011 – Clinical criteria • • • • Insidious onset of months to years Progression of cognitive decline Amnestic or nonamnestic cognitive impairment No obvious symptoms/signs of alternative type of dementia – Biomarkers • Accumulation of amyloid beta (CSF amyloid beta 42, PET amyloid imaging) • Neuronal injury (CSF tau, FDG PET, Functional MRI) McKhann GM et al. Alzheimer Dement 2011 Mixed dementia AD Mixed Knopman DS. Mayo Clin Proc. Feb 2006; 81(2):223-230. VaD Vascular Dementia • Diagnosis – Currently no consensus on what location or size infarct correlates with pathologic diagnosis of vascular dementia – Look for a suggestive history, physical exam with 23 focal signs, and brain imaging that shows ischemic disease Knopman DS. Dementia and Cerebrovascular disease. Mayo Clin Proc. Feb 2006; 81(2):223-230. Dementia with Lewy Bodies • Characteristics – Prominent visual hallucinations – Parkinsonism (gait, balance, rigidity, bradykinesia- rest tremor less common) – Falls or gait difficulties – Fluctuations in cognition – Sensitivity to antipsychotics (extrapyramidal side effects) • Also – REM sleep behavior disorder Knopman DS. Mayo Clin Proc, 2006; Blass DM, Rabins PV. Annals Int Med, 2008 Understand prognosis • Life expectancy from the time of diagnosis: – Alzheimer Disease 5-10 years – Vascular Dementia 4 years – Dementia with Lewy Bodies 4 years Is my patient on the right dementia drugs? Dementia Drugs: Dos, Don’ts, and Don’t knows Acetylcholinesterase Inhibitors • Donepezil (Aricept) • Galantamine (Razadyne) • Rivastigmine (Exelon) Cummings JL, NEJM, 2004 Efficacy Rogers: Neurology, 1998.136-145 NMDA antagonist Memantine (Namenda) Reisberg B et al. NEJM 2003 Drug candidates that to date have no proven efficacy • Anti-inflammatories • Cholesterol reducing agents • Estrogen • Antioxidants • Gingko biloba • Fish oil, omega-3 fatty acids • Vitamin E • Lowering homocysteine • Alcohol, especially wine • Huperzine • Curcumin • Nicotine • Insulin & insulin sensitizers, ketones How to handle nutrition in patients with dementia? Anorexia and Weight Loss • Common in patients with dementia • Especially Alzheimer disease • Possible causes – – – – – – – – Forgetting to eat Inability to prepare and eat foods Impaired olfaction and taste Behavior problems (restlessness, etc) Depression Comorbid medical illness Medications (esp cholinesterase inhibitors) Inflammatory abnormalities (causing anorexia, procatabolic state) Wang et al, J Neurol 2004, 251:314-320; Aziz NA et al, J Neurol 2008 • Controlled study of 51 AD subjects and 27 non-demented controls – AD subjects were thinner and less active – AD subjects actually ate the same or MORE than controls – Presence of AD was a risk factor for weight loss even if other factors were controlled • So maybe it’s poor absorption or metabolic changes Wang et al, J Neurol 2004, 251:314-320 • AD pts have increased serum levels of: – Glucagon – Ammonia – Lactate – Cortisol – Interleukins 1 and 6 – TNF alpha • AD pts have greater insulin resistance • All of above is similar to cancer patients Knittweis J, Medical Hypotheses, 1999 Strategies Diet- liberalize it! No special diets! Environment – Pleasant, quiet setting – Music may help Eating Schedule – AD pts ate more at breakfast than other meals – Frequent, small meals – Eat with others Tamura BK et al. Nutrition and the Institutionalized Elderly. 2007 Strategies Food Modifications – – – – – Single items, presented one at a time Contrast color of food with the dish Make food and setting look attractive Make food portable for those who are restless Sweet, hot/cold, juicy Tamura BK et al. Nutrition and the Institutionalized Elderly. 2007 Limited Data on Pharmacologic Strategies • Nutritional supplements between meals • Micronutrients (MVI) probably not needed • • • • Megestrol acetate (Megace) Dronabinol (Marinol) Methylphenidate (Ritalin) Mirtazepine (Remeron) Tamura BK et al. Nutrition and the Institutionalized Elderly. 2007 Feeding tubes When are they appropriate? Improved Survival? • Observational studies: – Study of 99 hospitalized patients with advanced dementia • survival without PEG 189 days, with PEG 195 days (P=0.9) • Mortality is high after G-tube placement – 6-28% in first 30 days – 60% mortality at 6 months, perhaps 90% at one year Murphy LM. Arch Int Med, 2003; Gillick MR. N Engl J Med. 2000; Meier DE et al, Arch Int Med 2001 Patient Comfort? • Studies of dying cancer or ALS patients with anorexia: – Little hunger or thirst • Any thirst can be treated with mouth swabs and ice chips – Sense of euphoria (endorphins) • Goes away if fed – Patients were left alone more Gillick MR. NEJM, 2000 Comfort? • Eating is pleasant! – depriving a person (who wants to eat) of the pleasure of eating does not increase comfort • Pulling out the tube – Return trips to GI or IR – Restraints • More stool and urine – Caregiver burdens high Finucane T et al. JAMA 1999 Aspiration • Aspiration of oral secretions is not reduced by feeding tubes • Aspiration of refluxed stomach contents is still also possible… and perhaps more likely given tendency towards gastric distension, low LES tone in tube-fed patients Mitchell SL. JAMA 2007 Slow hand feeding • Survival can be substantial despite emaciation and poor po intake • Human, nurturing, time for closeness with loved ones Finucane TE, JAMA, 1999 Dementia Taboo • Feeding tube- what is it, risks/benefits? – PEG, insert, endoscopy, interventional radiology, gastric, nutrition • Lack of efficacy of artificial nutrition – PEG, nutrient, mortality, euphoria, restraints, aspiration, palliative • Prognosis of advanced dementia – Mortality, terminal, PEG, limited life expectancy, palliative, cachexia, anorexia How can I help my patient who is agitated? Workup of agitation • Differential diagnosis for NEW agitation: – Delirium- drugs, infection, CNS process, etc – Psychiatric condition – Dementia Ballard CG et al. Nature Reviews Neurology, 2009 If no other cause is found… • Then it could be the dementia itself • Potential triggers: – PHYSICAL • Pain, constipation, hunger, thirst – EMOTIONAL • Anxiety, boredom, grief – ENVIRONMENTAL • Disruption in routine, new caregiver, life stressor, overstimulation, understimulation Lyketsos CG et al. Am J. Geriatric Psychiatry, 2006 Behavioral and Psychiatric Symptoms (BPSD) • Affects 60-98% of dementia patients • Aggression, agitation, delusions, hallucinations, repetitive vocalizations, wandering • Consequences: – – – – – increased caregiver stress unemployment loss of income NH placement increased costs of hospitalization • 30% of cost of caring for pts with dementia due to BPSD Sink KM et al, JAMA, 2005 BPSD Management • First line always nonpharmacologic • Try to analyze the behavior using A-B-C – A- antecedent – B- behavior – C- consequence • Also: – Correct sensory deficits – Create daily routine with activities – Create a structured environment – Ensure adequate sleep and eating – Provide respite and support to caregivers – Redirection and distraction Salzman C et al. J Clin Psychiatry 2008 Pharmacologic Management Pharmacologic treatment is a last resort • • • • • Antipsychotics Acetyl cholinesterase inhibitors NMDA antagonists Antidepressants Anticonvulsants/mood stabilizers Sink et al, JAMA, 2005 Antipsychotics • Haloperidol can be used if IV/IM route necessary – Mechanism: dopamine antagonist – Dosing: start at 0.5mg – Cost: $10/month • Atypical Antipsychotics are preferable due to lower rates of EPS, primarily po – Mechanism: dopamine/serotonin antagonists – Dosing: start risperidone at 0.5mg qhs, seroquel 25mg qhs – Cost: $95-300/mo Risks of Antipsychotics Extrapyramidal symptoms Sedation Prolonged QT Hyperglycemia, obesity (atypicals only) CVA – Post-hoc analyses (4% vs 2% for risperidone) • Infection (pneumonia) • Increased risk of mortality (RR 1.54) – Post-hoc analyses (2.3% vs 3.6%) – FDA black box warning • • • • • Schneider LS et al, JAMA 2005; 294:1934-43; Wang PS et al, NEJM 2005; 353:2335-41 Antipsychotics Summary • Discuss risks with patients/family prior to initiating these medications • Never use for insomnia • Doses should be low • Attempts to discontinue pharmacologic treatment should be performed early and often Dementia Summary • Dementia is common and commonly overlooked • Alzheimer disease is by far the most common type • Current medications for dementia have modest benefits but should be offered if appropriate • Feeding issues in advanced dementia are not usually solved with feeding tubes • Antipsychotics should be avoided in dementia patients with agitation Useful References • Blass EM and Rabins PV. In the clinic: Dementia. Annals of Internal Medicine 2008 • Mitchell SL. A 93 year old man with advanced dementia and eating problems. JAMA 2007;298(21):2527-2536 • Salzman C et al. Elderly patients with dementia-related symptoms of severe agitation and aggression: Consensus statement on treatment options, clinical trials methodology, and policy. Journal of Clinical Psychiatry 2008;69:889-898