Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
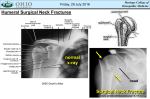
Brachial Plexus injuries (Obstetric) Dr Kannan K Kumar Consultant Hand and Brachial Plexus surgeon Hosmat hospital • Dr Paul Brand fellow in Hand surgery and brachial plexus, Christian medical college, Vellore • Kleinert fellow in hand and microsurgery, University of Louisville, Kentucky, USA • Fellow in brachial plexus surgery, OGDH, Yamaguchi, Japan CONTENTS • • • • • Anatomy Origin and formation of brachial plexus Obstetric Brachial Plexus injuries Treatment Salvage procedures ANATOMY Ventral rami, of the lower cervical and upper thoracic nerve roots Components of brachial plexus It includes – From above the fifth cervical vertebra to underneath the first thoracic vertebra(C5T1). • The trunks pass laterally and lies around the subclavian artery • Behind the clavicle, each trunk splits into anterior and posterior divisions. FORMATION OF THE BRACHIAL PLEXUS Cadaver • FORMATION OF THE BRACHIAL PLEXUS • Roots • The ventral rami of spinal nerves C5 to T1 are referred to as the roots of the plexus. • Trunks • Shortly after emerging from the intervertebral foramina , these 5 roots unite to form three trunks. –The ventral rami of C5 & C6 unite to form the Upper Trunk. –The ventral ramus of C 7 continues as the Middle Trunk. –The ventral rami of C 8 & T 1 unite to form the Lower Trunk. • Divisions Each trunk splits into an anterior division and a posterior division. • Cords • – Upper and Middle trunks - lateral cord. • – Lower trunk - medial cord. • – Posterior divisions posterior cord. • – Position relative to the axillary artery • III. BRANCHES : • From the Roots • Dorsal Scapular nerve Derived from C5 root Motor nerve to the Rhomboideus major and minor muscles • Long Thoracic nerve Derived from C 5,6,7 Innervates the serratus anterior muscle FORMATION OF THE BRACHIAL PLEXUS • From the Upper Trunk • Nerve to subclavius muscle • Suprascapular nerve • From the Lateral Cord • Lateral Pectoral nerve Innervates the clavicular head of the pectoralis major muscle • From the Medial Cord • Medial Pectoral nerve Innervates the sternocostal head of the pectoralis major muscle Innervates the pectoralis minor muscle FORMATION OF THE BRACHIAL PLEXUS Cutaneous distribution ANATOMIC VARIATIONS • The plexus may include ventral rami from C4 or T2 and these are designated as • Pre fixed- C4 added • Post fixed- T2 added. OBSTETRIC BRACHIAL PLEXUS PALSY HISTORY • • • • • • • Early days – congenital deformity. Smillie [1768] – Obstetric origin Danyau [1851] – Autopsy – lesion Duchenne [1861]- traction injury, OBPI ERB [1875]- pointed lesion at upper trunk Kennedy [1903]- early surgical repair Narakas [1981]- microsurgical results. • Incidence: 0.13 - 4/1000 live births • Spectrum • Difficult to diagnose early on – Pseudoparalysis Erb’s palsy • Erb's palsy (Erb-Duchenne Palsy) is a paralysis of the arm caused by injury to the upper trunk C5-C6. • Signs of Erb's Palsy • Deltoid, biceps, and brachialis muscles. • The arm hangs by the side and is rotated medially; the forearm is extended and pronated. commonly called "waiter's tip hand." • Erb’s Palsy – Nerves Affected Left Erb’s point Klumpke s palsy • Variant involving the lower roots. • C8 and T1 nerves. • Affects, principally, the intrinsic muscles of the hand and the flexors of the wrist and fingers. • The classic presentation of Klumpke's palsy is the “claw hand” where the forearm is supinated and the wrist and fingers are hyperextended with flexion at interphalangeal and metatarso phalangeal joints. MECHANISM • Stretching • Overweight babies with cephalic presentations • Underweight babies with breech • Forceful widening of angle between the neck & shoulder. • Vacuum pump • Forceps Associated injuries • • • • • • • C-spine fracture Torticollis Clavicle fracture Shoulder dislocation Humerus fracture Facial nerve palsy Phrenic nerve palsy PATHOLOGY • Lesions range from degree I[neuropraxia] – V [neurotmesis or root avulsions]. • Upper trunk –1st affected, most vulnerable part. • Upper trunk – mostly stretched • Lower trunks – mostly ruptured Clinical assessment • Limb is flail & dangling • Arm is held in IR, adduction, active abd not possible, elbow extended, forearm pronated, thumb flexed. • Complete paralysis- vasomotor impairment, pale & marble like color • Horner’s sign • Associated # [clavicle,humerus,] Prognosis • Complete Recovery (80%) • Partial recovery • No improvement. EMG • Performed at 3-4 wks- confirm neuropraxia or axonotmesis (difficult to perform) • At 2 months, signs of re-innervation. • Fluoroscopy- phrenic nerve injury. • Lumbar puncture- xanthochromic CSF- in root avulsions. • C.T myelogram • Fast spin Echo MRI: preganglionic nerve root injuries. (only if necessary) • Large diverticulae and meningoceles are indicative of root avulsions DD • Fracture of clavicle or humerus shaft or physeal separation • Septic arthritis / osteomyelitis • Congenital malformation of plexus • Postinfectious [varicella] plexopathy of muscles • • • • Prognostic signs Nature of injury Lower plexus paralysis, Global involvement, Persistence of Horner’s and phrenic nerve palsy • Presence of Torticollis Treatment • Physiotherapy • ROM ex, facilitation of active movt, promotion of sensory awareness. • Avoid abduction & posterior projection of shoulder. Limb to be supported when holding baby • Goals: minimizing bony deformities, Jt contractues. • Weight bearing activity-skeletal growth SURGICAL Early nerve repair • Indications: 1. Failure of recovery of biceps or deltoid at 3 months 2. Group III& IV lesions 3. Presence of Horners sign. Cookie sign • Failure to flex the elbow, so as to take the hand to the mouth. • 3-6months. Advantages of nerve repair • Diminishing potential for axon regeneration with age • Cross innervation & muscle imbalance aborted • Provide better condition for tendon transfer • Nerve repair is superior to spontaneous recovery. Timing of surgery • 1. 2. 3. 4. 5. 5 months – 1 year TYPE OF SURGERY Neurolysis Direct repair Nerve grafting Nerve transfers Free functioning muscle transfers Neurolysis Direct Repair Direct Repair Direct Repair Nerve Grafting Nerve grafting Free functioning muscle transfer Common donors • • • • Spinal accessory (XIth) nerve. Intercostal nerves (commonly 3rd to 6th) Fascicles of the median and ulnar nerves Opposite C7. Common recipient nerves Order of priority of restoration of function • Elbow flexion(Musculocutaneous nerve) • Shoulder stability (suprascapular nerve and axillary nerve) • Hand prehension Late OBPP • Nerve regeneration: some muscles recover earlier, others paretic muscle imbalance • Recovery results from misdirection of regenerated axons cross innervation Cross innervation • Co-contraction of synergestic & antagonistic muscles • Diminishing functional recovery • Muscle contracture deformity HAND DEFORMITY • In flaccid paralysis of complete lesion • Difficult to manage & difficult to rehabilitate • If no active wrist extension & no possible transfers – W. fusion with comb intermetacarpal arthrodesis. Take home points • Obstetric brachial plexus injuries may be avoidable if timely C-section is performed. • Early referral to a brachial plexus surgeon once the diagnosis is made. • All is not lost – Nerve surgery or other secondary procedures can improve function drastically. Thank you [email protected]