Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
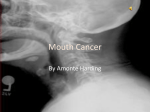
Case Report Int J Clin Prev Dent 2015;11(1):51-54ㆍhttp://dx.doi.org/10.15236/ijcpd.2015.11.1.51 ISSN (Print) 1738-8546ㆍISSN (Online) 2287-6197 Oral Manifestation and the Treatment of Self-Injurious Behaviors Associated with a Preterm Infant: A Case Report Su-Hyun Shim1, Byeng-Ken Cho2, Ja-Won Cho2 1 Department of Dental Hygiene, Kyungbok University, Namyangju, 2Department of Preventive Dentistry, College of Dentistry, Dankook University, Cheonan, Korea Behavioral problems could be easily observed in patients with various mental disorders. Self-injurious behavior (SIB) can be defined as deliberated harm to one’s own body without conscious suicidal intent. It usually occurs as head banging or hitting, body hitting, skin cutting, or finger biting. Also it frequently involves oral tissue’s damage in pediatric patients, such as lip, cheek and tongue biting. Various articles have described prostheses used to prevent SIB-related injuries to the oral tissues of patients who have developmental or medical problems, such as psychological problems, congenital syndromes or mental retardation. But reports of oral SIB in individuals unaffected by the above conditions are scarce. The case presented in this report discusses oral SIB in a premature baby. We found an optimal way that would prevent SIB-related injuries and also protect the causative teeth. These days, dentists should be able to manage those patients with several treatment modalities, furthermore, to prevent SIB according to the causative disorders. Keywords: preterm birth, self injurious behavior, self mutilation Introduction such as bipolar disorder and depression, those with conditions that result in indifference to pain, such as familial dysautonomia, and others with a variety of developmental disabilities [2]. The prevalence of SIB in the general population has not been established, but it is estimated that such problems could affect about 750 out of every one million individuals [3]. Prevalence is higher among females [4]. The origin of SIB is complex, and theories exist of both biological and functional origins. Medina et al. [4] list biological causes such as Lesch-Nyhan syndrome, Cornelia de Lange syndrome, Tourette syndrome and XYY syndrome, as well as other conditions including mental retardation, encephalitis, congenital malformations, coma and epilepsy. The typical cause of such behaviors in children is Lesch-Nyhan syndrome, followed by mental deficiency and infectious diseases such as encephalitis. However, reports of oral SIB in individuals unaffected by the Self-injurious behavior (SIB) is defined as deliberated damage of one’s own body without suicidal intent [1]. It could vary from a trifling injury to damages that could lead to further disabilities. And diverse populations have been known to exhibit SIB. These include individuals with psychiatric diagnoses Corresponding author Ja-Won Cho Department of Preventive Dentistry, Dankook University College of Dentistry, 119 Dandae-ro, Dongnam-gu, Cheonan 330-714, Korea. Tel: +82-41-550-1953, Fax: +82-41553-6582, E-mail: [email protected] Received March 6, 2015, Revised March 17, 2015, Accepted March 18, 2015 Copyright ⓒ 2015. Korean Academy of Preventive Dentistry. All rights reserved. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/ by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. 51 International Journal of Clinical Preventive Dentistry above conditions are rare. So this report presents oral SIB case associated only with preterm infant. Case Report A 10-month old infant who was hospitalized for a pre-term birth was consulted from his pediatrician because of traumatic ulcer of tongue (Figure 1). His pediatrician told that his tongue thrusting habit began with the eruption of mandibular primary incisor. The doctor added that the frequency and severity of the tongue biting was proportional to the eruption. An oral examination showed trauma was induced by his tongue thrusting and biting habit. But there were no anchorage in his mouth as he was just 10-month infant. A typical removable prosthesis could not be applicable. So we tried to apply stainless steel crown to his unerupted #81 tooth first (Figure 2). Ten days after delivery of stainless steel crown, he was referred from his medical doctor again. Althoug the size of ulcer was decreased, it still remained (Figure 3). After dressing and oral examination, we soon noticed that the patient still had tongue biting habit with #71 tooth. But #71 tooth was erupted less than the half of its crown height. His parents and pediatrician allow us to extract the tooth. In order to avoid the extraction, we applied stainless steel crown to the #71 tooth lastly. One month later, we recalled the patient. Traumatic ulcer of tongue was successfully treated (Figure 4). Four month after delivery, the patient was referred from his pediatrician due to a traumatic ulcer of tongue again. After oral examination, we found that this ulcer was owing to the eruption Figure 3. Ten days after delivery. Figure 1. Traumatic ulcer of tongue. Figure 2. Delivery of stainless steel crown in #81 tooth. 52 Vol. 11, No. 1, March 2015 Figure 4. One month after delivery of stainless steel crown. Su-Hyun Shim, et al:Oral Manifestation and the Treatment in Self-Injurious Behaviors of #82. However, the tooth had just erupted. We just smoothened the surface of #82 tooth and covered the tooth with glass ionomer slightly. We instructed his parents and pediatrician to wait until the tooth was erupted enough for stainless steel crown delivery. However, against our expectations, his tongue biting habit was disappeared after the fully eruption of #82 tooth. For about 2 years, we followed the patient and there was no significant sign and symptom though the primary dentition was completed. Discussion According to Medina et al. [4], among the many proposed treatment modalities for SIB, the most common include medications, behavior modification or physical restraints. Prescribed medications and behavior modification techniques may be helpful for some patients with SIB, but these approaches are labor-intensive [5]. And when we used physical restraints, we must provide the most effective protection with minimal restraint. Therefore usually, no single treatment method guarantees the eradication of SIB [4]. Few document [6] reports injuries caused by biting in patients who do not have psychological, mental or congenital disorders. When prescribing a prosthesis such as the one described in this case report for SIB treatment, it is necessary to choose a design that is appropriate for the patient’s age, general health, ability to cooperate and the severity of the oral injuries [7]. According to Hanson et al. [8], a prosthesis to prevent oral self-injury should be designed to: deflect tissues to be damaged by involuntary, mandibular movements away from the occlusal table; avoid posing further injury to the patient; permit a full range of mandibular motion; allow for daily oral care; withstand breakage and displacement over time; allow healing of traumatized oral tissue and be easily fabricated and installed without discomfort or risk to the patient. SIB usually occurs as tongue and lip biting in oral tissue. In case of tongue biting, we have to separate tongue and teeth considering the mandibular movement pattern [9]. Like this case, there is no standard method for preventing SIB. A suitable oral guard could be tried initially before employing more invasive approaches. Furthermore, after delivery of the appliance, the long term education to the patient, family and nurses is needed. These days clinicians should be well aware of the treatment modalities, and research to discover how to prevent oral SIB in dental clinic. References 1. Chen LR, Liu JF. Successful treatment of self-inflicted oral mutilation using an acrylic splint retained by a head gear. Pediatr Dent 1996;18:408-10. 2. Pies RW, Popli AP. Self-injurious behavior: pathophysiology and implications for treatment. J Clin Psychiatry 1995;56:580-8. 3. Saemundsson SR, Roberts MW. Oral self-injurious behavior in the developmentally disabled: review and a case. ASDC J Dent Child 1997;64:205-9, 228. 4. Medina AC, Sogbe R, Gómez-Rey AM, Mata M. Factitial oral lesions in an autistic paediatric patient. Int J Paediatr Dent 2003;13:130-7. 5. Romer M, Dougherty N, Fruchter M. Alternative therapies in the treatment or oral self-injurious behavior: a case report. Spec Care Dentist 1998;18:66-9. 6. Walker RS, Rogers WA. Modified maxillary occlusal splint for prevention of cheek biting: a clinical report. J Prosthet Dent 1992;67:581-2. 7. Romero M, Vicente A, Bravo LA. Prevention of habitual cheek biting: a case report. Spec Care Dentist 2005;25:214-6. 8. Hanson GE, Ogle RG, Giron L. A tongue stent for prevention of oral trauma in the comatose patient. Crit Care Med 1975; 3:200-3. 9. Pigno MA, Funk JJ. Prevention of tongue biting with a removable oral device: a clinical report. J Prosthet Dent 2000;83: 508-10. www.ijcpd.org 53