Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
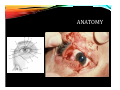
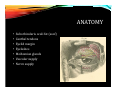
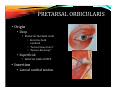
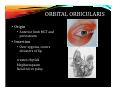
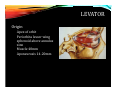
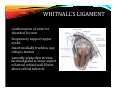
GREENVILLE HEALTH SYSTEM G H S C l i n i c a l U n i v e r s i t y P a r t n e r s EYELID ANATOMY AND SURGICAL APPLICATIONS John D. Siddens, D.O. Ophthalmic Plastic & Reconstructive Surgery GHS Plastic & Aesthetic Surgery Greenville Hospital System University Medical Group Greenville, South Carolina 2014 Mid‐Year Seminar AOCOO‐HNS/F Detroit, Michigan October 11, 2014 Associate Clinical Professor of Ophthalmology University of South Carolina School of Medicine Department of Ophthalmology Columbia, South Carolina Associate Clinical Professor of Ophthalmology and Surgery University of South Carolina School of Medicine - Greenville Greenville, South Carolina ANATOMY • Anatomy • Skin/subcutaneous • Protractors • Orbicularis mm • Orbital septum • Orbital fat • Retractors • Upper eyelid • Levator • Muller’s • Tarsus • Conjunctiva ANATOMY • Suborbicularis oculi fat (soof) • Canthal tendons • Eyelid margin • Eyelashes • Meibomian glands • Vascular supply • Nerve supply SKIN • Eyelid skin – thinnest skin in the body • NO subcutaneous fat • Horizontal 30 mm • Vertical palpebral fissure averages 10 mm • Lateral canthal angle 2 mm higher than medial • Potential space between pretarsal/preseptal tissue PROTRACTORS • Orbicularis • CN VII • Palpebral (involuntary) • Pretarsal/preseptal • blink • Orbital (voluntary) • Orbital orbicularis • forced closure, wink PRETARSAL ORBICULARIS • Origin • Deep • Posterior lacrimal crest • Encircles both caniliculi • “horner tensor tarsi” • “horner‐duverney” • Superficial • Anterior limb of MCT • Insertion • Lateral canthal tendon Lacrimal pump ORBITAL ORBICULARIS • Origin • Anterior limb MCT and periosteum • Insertion • Over zygoma, covers elevators of lip creates rhytids blepharospasm facial nerve palsy ORBITAL SEPTUM Thin fibrous membrane Origin Periosteum orbital rim at arcus marginalis “suborbicularis fascia” Loose areolar tissue separates preseptal from postseptal space ORBITAL SEPTUM • Insertion • Medially • Posterior/anterior lacrimal crest • Isolates lacrimal sac from orbit and eyelid • Lateral • Anterior to lateral canthal lig • Whitnall’s tubercle ORBITAL SEPTUM Insertion Upper lid 2‐4mm above superior border tarsus with levator aponeurosis Lower lid 4‐5mm below inferior border tarsus with inferior tarsal muscle, to inferior tarsus SURGICAL SUTURING OF SEPTUM RESULTS IN RETRACTION OF EYELID Posterior to septum Anterior to levator and CPF 3 pads lower eyelid 2 pads upper “fat is your friend” – for locating levator in ptosis repair watch for IO in lower lid bleph ORBIT FAT RETRACTORS • Upper lid • Levator • Muller’s (superior tarsal mm) • Lower lid • Capsulopalpebral fascia (CPF) • Inferior tarsal mm LEVATOR Origin Apex of orbit Periorbita lesser wing sphenoid above annulus zinn Muscle 40mm Aponeurosis 14‐20mm LEVATOR Insertion Anterior Fine strands between pretarsal orbic mm bundle Crease results from superior most attachment Posterior Ant surface lower ½ tarsus Firm 3mm above margin Loose sup 2‐3mm tarsus Collagen elastic fibers LEVATOR Lateral horn Strong Divides orbital lobe from palpebral lobe of lacrimal gland Inserts at lateral orbital tubercle LEVATOR Medial horn Delicate Loose connective tissue Inserts posterior aspect MCT and posterior lacrimal crest the strong insertions at the medial and lateral horn is what creates ‘levator function’ WHITNALL’S LIGAMENT Condensation of anterior sheath of lev mm Suspensory support upper eyelid Insert medially trochlea, sup oblique tendon Laterally septa thru stroma lacrimal gland to inner aspect of lateral orbital wall 10mm above orbital tubercle