Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
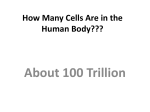
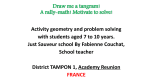
Reference Values for and Determinants of Right Atrial Area in Healthy Adults by 2-Dimensional Echocardiography Ekkehard Grünig, MD*; Philipp Henn*; Antonello D’Andrea, MD*; Martin Claussen, MD; Nicola Ehlken, BSc; Felicitas Maier; Robert Naeije, MD, PhD; Christian Nagel, MD; Felix Prange; Johannes Weidenhammer; Christine Fischer, PhD*; Eduardo Bossone, MD* Background—Right atrial (RA) size is important in screening, diagnosis, and follow-up assessment in patients with pulmonary Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 hypertension. The objective of this study was to define normal reference values for RA area by echocardiography in a large population of athletic versus sedentary healthy subjects. Methods and Results—In the first part of the study, 880 healthy adult subjects (mean age, 28±6 years; 38% women; 395 top-level endurance athletes, 255 strength athletes, and 230 nonathletes) were prospectively assessed. In the second part, we performed a pooled analysis of all studies published between 1976 and 2011 describing RA area in healthy subjects (n=624). Statistical analysis included the calculation of 95% quantiles for defining cutoff values. Mean RA area in the 880 subjects was significantly larger in endurance athletes compared with the strength athletes and nonathletes. RA area correlated significantly with age, sex, body surface, and endurance training. In a synopsis of both data sets, 95% quantiles for RA area in strength atheletes and nonathletes were 15.2 cm2 (95% confidence interval, 14.7–15.7) in women and 16.2 cm2 (95% confidence interval, 15.8–16.6) in men. Conclusions—To the best of our knowledge, this is the largest data set to describe RA size in adult healthy subjects (age <50 years). Cutoff values for RA area were significantly different in women (15 cm2) and men (16 cm2). Age, sex, body surface area, and high-level endurance training were determinants of RA area. (Circ Cardiovasc Imaging. 2013;6:117-124.) Key Words: echocardiography ◼ pulmonary hypertension ◼ reference values ◼ right atrium ◼ risk factors R ight atrial (RA) size is of clinical importance because it reflects right ventricular (RV) function and is strongly associated with clinical outcomes in many conditions such as pulmonary hypertension.1–3 The normal RA is a thin, oval structure influencing RV function as a passive conduit to the RV in early diastole. When the tricuspid valve is open, it acts as a reservoir for systemic venous return and fills the RV by active contraction during late diastole.4 RA contraction is responsible for up to 30% of normal RV output.5 In healthy subjects, short elevations of RV pressure lead to stretching and enlargement of the RA, resulting in more reservoir volume. This mechanism has been identified to compensate for short-term RV overload.6 Chronic pulmonary hypertension is followed by enlargement and remodeling of the RA with hypertrophy and reduced contractility.7,8 assessments in several diseases affecting the right side of the heart such as cardiomyopathy and pulmonary hypertension.9–11 For echocardiographic evaluation of the RA size, the RA area is easy to obtain and seems to be more reliable assessing RA diameters or volume.11,12 Volumetric quantification of the right atrium is challenging because many assumptions are required11 and it is more difficult to perform in the daily clinical practice. However, there are limited data on the normal size of the RV and RA.3,11,13 Furthermore, echocardiographic views required for optimal evaluation of the right heart are less well standardized, leading to inconsistent measurements of RV and RA size. The reference value given for mean RA area in the recommendations of the American Society of Echocardiography of 18 cm2 is not sex specific and is based on few studies including only 293 healthy subjects. Therefore, the authors of the current American guidelines for echocardiography stated that their text has to be viewed as an incentive to refine the normal values of the right heart.11 Today, there are no reference values given for RA area/size indexed for body surface area (BSA), age, physical training status, or sex in any guidelines.11 Clinical Perspective on p 124 Echocardiography has become the most clinically relevant noninvasive diagnostic technique evaluating the right heart.9 It can be used for screening, diagnosis, and follow-up Received June 19, 2012; accepted November 15, 2012. From the Centre for Pulmonary Hypertension at Thoraxclinic Heidelberg, Heidelberg, Germany (E.G., P.H., N.E., F.M., C.N., F.P., J.W.); Second University of Naples, Monaldi Hospital, Naples, Italy (A.D.); Department of Pneumology, Clinic Grosshansdorf, Grosshansdorf, Germany (M.C.); Erasme University Hospital Free University of Brussels, Brussels, Belgium (R.N.); Department of Human Genetics, University of Heidelberg, Heidelberg, Germany (C.F.); and Cardiology Division, “Cava de’ Tirreni and Amalfi Coast” Hospital, Heart Department, University of Salerno–Italy, and Cardiac Surgery Department, IRCCS Policlinico San Donato, Milan, Italy (E.B.). *Drs Grunig, Henn, and D’Andrea contributed equally to this work. Correspondence to Ekkehard Grünig, MD, Centre for Pulmonary Hypertension Thoraxclinic, University Hospital Heidelberg, Amalienstrasse 5, 69126 Heidelberg, Germany. E-mail [email protected] © 2012 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org 117 DOI: 10.1161/CIRCIMAGING.112.978031 118 Circ Cardiovasc Imaging January 2013 The aim of this study was to analyze the dimensions of RA area first in a large prospectively assessed population of healthy adults and second in a pooled analysis of all previously reported studies, including those that have not been taken into account in the current guidelines. Thus, we aimed to confirm reference values for RA area using prospectively obtained data and analyzing previously reported data. Furthermore, we wanted to identify determinants of RA size such as sex, age, BSA, and exercise training status. Methods Study Population Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 From June 2008 to March 2009, 880 healthy athletic and nonathletic subjects were prospectively and consecutively studied by 2-dimensional echocardiography at Monaldi Hospital, Naples, Italy, as previously described.14 The athletes were employed by professional sports associations and had been trained intensively 15 to 20 h/wk for >4 years. The subjects were referred for cardiovascular preparticipation screening. Volunteer control subjects were all recruited in Naples (Italy), selected from the Department of Cardiology, and investigated for work eligibility. None of the control subjects had cardiovascular structural or functional abnormalities or received any medication. All subjects underwent a detailed history, physical examination, BSA, ECG, chest radiography, exercise test, and comprehensive transthoracic echocardiography, including Doppler studies, as described previously.14 Subjects with cardiopulmonary diseases such as coronary artery disease, systemic arterial hypertension, valvular or congenital heart disease, bicuspid aortic valve, congestive heart failure, cardiomyopathies, and diabetes mellitus were excluded. Additional exclusion criteria were sinus tachycardia and inadequate echocardiographic image quality. Use of anabolic steroids or other illicit drugs was ruled out by medical history and patient interview. According to these criteria, 10 subjects were excluded (3 for bicuspid aortic valve, 1 for hypertrophic cardiomyopathy, 4 for use of anabolic steroids, and 2 for inadequate echocardiographic image quality). The final study population consisted of 880 subjects. Although results for healthy nonathletes have not been analyzed yet, some data on the function of the right side of the heart in athletes have been reported previously.14 The study was approved by the local Ethics Committee. All subjects enrolled in the study gave informed consent. Echocardiographic Assessment Doppler and 2-dimensional echocardiographic recordings were performed with 2.5-MHz Duplex probes and conventional equipment (Vivid 7, GE Healthcare, Milwaukee, WI) by experienced cardiac sonographers. RA measurements were assessed in the apical 4-chamber view. RA area was estimated by planimetry at the end of ventricular systole (largest volume), tracing from the lateral aspect of the tricuspid annulus to the septal aspect, excluding the area between the leaflets and annulus, after the RA endocardium (Figure 1). All studies were reviewed and analyzed offline by 2 independent observers blinded to the clinical characteristics of the study population. As an example, Figure 1 shows a normal and an enlarged RA area measured by echocardiography and describes the technique. For exclusion of pulmonary hypertension or any heart diseases possibly affecting the size of the right side of the heart such as congenital heart defects, a complete echocardiographic assessment, including assessment of pulmonary artery pressures, was performed in all subjects.15 For all calculations, the mean value from at least 3 to 5 measurements was used. RA pressure was estimated from characteristics of the inferior vena cava.16 Patients with suspected heart diseases or elevated pulmonary systolic artery pressures (>35 mm Hg) and elevated estimated RA pressure (diameter of inferior vena cava >20 mm) were excluded. Figure 1. Echocardiographic measurement of the right atrial (RA) area in the apical 4-chamber view. The figure shows schematically and echocardiographically how RA area measurements have been performed in the apical 4-chamber view. Left, The RA area is of normal size. Right, An enlarged RA area in a patient with pulmonary arterial hypertension. reference values in humans. Our approach was to search by Medical Subheadings or key words related to RA size, diameters, volume, and area. In addition, reference lists of relevant studies, practice guidelines, and reviews were screened to identify further studies not detected by the electronic search. All studies in English, German, and Italian were screened. We selected studies that described RA size/ area in healthy adults without cardiovascular diseases using standardized echocardiographic views. We excluded studies with unclear echocardiographic techniques or status of subjects. Statistical Methods All analyses were performed by a statistician (C.F.). Determination of RA Area and RA Area Indexed for BSA In the prospective analysis, all reported values of RA area represent the mean of at least 3 measurements. To calculate RA area indexed for BSA in the prospective study, we used the following formula: RA area indexed for BSA (cm2/m2)=RA area absolute (cm2)/BSA (m2) for each individual measurement. BSA was calculated using this formula: BSA=weight (kg) 0.425×height (cm)×71.84×10–4.17 If only RA area absolute or RA area indexed was given in the literature, we calculated the other value using the mean BSA if possible (see Table 1). Literature Search Prospective Analysis RA areas are presented as means and standard deviations. As upper cutoff values for normal RA areas for women and men, we used 95% quantiles and their 95% confidence intervals (CIs). The values were calculated with and without assuming a normal distribution using SAS version 9.2 (SAS Institute Inc, Cary, NC). The calculation assuming nonnormally distributed values led to nearly identical quantiles and CIs; therefore, we present the results assuming normality. The comparison of 95% quantiles between men and women and between groups with different exercise training status was performed with the SAS QUANTREG procedure. We performed a systematic literature search using Medline and the Cochrane Database for studies published between January 1966 and October 2011 reporting echocardiographic RA measurements in healthy subjects. This encompassed studies reporting normal Analysis of Determinants We calculated correlation coefficients to describe determinants of RA area. Additionally, groups with different exercise Grünig et al Reference Values of Right Atrial Area 119 Table 1. Characteristics of Pooled Analysis of Selected Studies on Right Atrial Area by 2-Dimensional Echocardiography Author Year n Retrospective Study Design Ref. 22 1979 25 X 44 Ref. 23 1983 11 X 27 X Ref. 19 1984 30 ? 50 X Ref. 12 1984 67 ? ? Ref. 20 1984 54 Ref. 18 1986 43 Ref. 21 2007 160 Ref. 24 2009 15 Ref. 25 2010 219 Sum Women, % 46.3 ? BSA Sex Distinction X Index Athletes Nonathletes Men X 45 X X X 22–37 X X 31±10 X 38 X 38.4 X X X 51.2 X X 37.5 X X 54.3 Abs. Mean Age, y X 53 X Area X X X X X X X Women 28±8 37.6 X 40±14 36±14 X 24.9±4.4 22.2±4.5 X X 36±12 X X 29.7±25.2 624 Abs. indicates absolute; and BSA, body surface area. Studies are listed in chronologic order of publication year. Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 training status (ie, endurance-exercise training, strength-exercise training, or nonathletes) and sex groups were compared by ANOVA. Multivariate regression analysis was performed to take age, BSA, and sex into account simultaneously. Values of P<0.05 were considered statistically significant. For these analyses, we used IBM SPSS 20 (SPSS Statistics version 20, IBM Corp, Somers, NY). Literature Analysis Because only aggregated data, namely means, standard deviations, and sample sizes, are given in the literature, we estimated the 95% percentile assuming normally distributed data. Additionally, 95% CIs for the 95% percentile were determined by using the 97.5% CIs of the estimated mean and standard deviation of each single study. We combined the results from the literature with our data by pooling means and standard deviations for each study weighted by sample size, assuming a common underlying normal distribution. From the pooled mean and the pooled standard deviation, the 95% percentiles and their 95% CIs were estimated as described above. To analyze the influence of single studies on the pooled estimate, a sensitivity analysis was performed by leaving out 1 study at a time and calculating the pooled estimates with the remaining studies. All these analyses were performed with tailored software. Results RA Area Prospectively Obtained in Healthy Athletes/Nonathletes We prospectively assessed 880 healthy adults: 230 nonathletes, 255 strength athletes, and 395 endurance athletes (Table 1 and Figures 2 and 3). Mean age was 28.2±10.5 years (range, 18–45 years) and did not differ significantly between groups. The mean absolute and indexed RA area values with standard deviations, the 95% quantiles, and the range of CIs are shown in Table 1. The 95% quantiles that have been defined as cutoff values for normal RA area were almost identical in nonathletes and strength athletes. In nonathletes, the 95% quantiles were significantly different between men and women (P=0.0042): 15.1 cm2 (CI, 14.3–16.0) in women, 15.7 cm2 (CI, 15.1–16.5) in men, and 15.5 cm2 (CI, 15.1–15.9) in the mixedsex group (Table 1). RA area indexed for BSA in nonathletes was 8.2 cm2/m2 in women, 8.4 cm2/m2 in men, and 8.3 cm2/m2 in the mixed-sex group (Table 1). Correlation Analysis of RA Area With Age, Sex, BSA, and Exercise Training Status RA area means were significantly different among nonathletes (12.5±2.0 cm2), strength athletes (12.7±1.6 cm2), and endurance athletes (15.4±2.1 cm2; P<0.0001, ANOVA; Figure 2A) and Figure 2. Determinants of right atrial (RA) area. A, Type of training. B, Sex. A, Whisker plot illustrating the effect of endurance and strength training on RA area, prospectively evaluated. Endurance athletes had significantly larger RA areas compared with nonathletes and strength athletes. B, Significantly different RA area sizes in male and female nonathletes. The boxes represent the values of all subjects between the 25% and 75% quantiles (median line; the range from 5% to 95% quantiles is shown by the whiskers. 120 Circ Cardiovasc Imaging January 2013 Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 between men and women of the nonathletic group (P=0.0042; Figure 2B). If sex, age, BSA, and training status were taken into account simultaneously, only the correlations of RA area with endurance training and BSA, but not sex, remained significant. There was a significant but weak correlation of RA area with age (r=0.17, P<0.0001) and BSA (r=0.33, P<0.0001) in nonathletes and strength athletes (n=485). In endurance athletes (n=395), a weak correlation between RA area and age (r=0.23, P<0.001) and between RA area and BSA (r=0.29, P<0.001) occurred. Only 3% of the variability of RA area could be explained by age; 11% could be explained by BSA. The different RA areas in men and women were confirmed in the pooled analysis of those previously published studies that distinguished between sexes. In all of these studies,18,19,21 we found significantly different mean RA areas in men and women, ranging from 2.6 to 3.0 cm2. In publications selected for the pooled analysis, we could not perform further correlation analysis concerning age, training status, and BSA or any other variables because only mean values for RA area were given and no analysis for determinants had been reported. RA Area Obtained by Pooled Analysis of Previously Published Studies Eleven studies were detected by screening of Medline databases and Cochrane databases for RA size. Two of the 11 studies were excluded.2,26 The second oldest of the 11 studies from Reeves et al26 identified a mean value of RA area of 16.1±3.4 cm2 in a mixed-sex cohort of 21 healthy control subjects. However, they used a sector-scan echocardiography Picker 80-C cardiac imager that was technically limited; echocardiographic 4-chamber views were different.26 The data of Raymond et al2 were not included because the RA area index was calculated from height instead of BSA. Therefore, because no mean height was provided, we were unable to calculate the absolute or indexed values for RA area. Thus, 9 studies published between 1979 and 2011 with 624 healthy subjects were used for the pooled analysis (Table 2). The assessed subjects had been classified as healthy and free of heart disease in all studies. As far as specified, most studies had performed ECGs and physical examinations to exclude any heart disease. In 1 study, catheterization of the right and left sides of the heart had been performed.26 In addition, in this study, rubber casts fashioned from the rightside chambers during necropsy had been assessed in 8 deceased subjects without clinical or anatomic evidence of heart–lung diseases to validate the echocardiographic dimensions of the heart chambers.22 Overall, the assessed subjects were between 18 and 70 years; the mean age ranged between 22.2±4.5 years21 and 45 years22 (Table 2). Most subjects were <50 years of age. The sample size ranged from 11 to 219 subjects per study. The percentage of women ranged from 27% to 54.3%, although 1 study did not mention sex distribution (Table 2). Three studies were retrospective in design; in 3 others, the study design was not completely clear; 5 studies12,18–20 were designed for reference value determination; and 4 studies21–25 used healthy subjects as the control group. Table 3 summarizes the mean values for absolute and indexed RA area, standard deviations, 95% quantiles, and Table 2. Right Atrial Area Prospectively Obtained in 880 Healthy Subjects Sex Nonathletes Strength Athletes Endurance Athletes No. (%) Men Women 137 (15.6%) 155 (17.6%) 255 (29.0%) 93 (10.6%) 100 (11.4%) 140 (15.9%) RA area, cm2 Men Mean±SD 12.5±2.0 12.7±1.6 15.4±2.1 Q-95 (CI) 15.7 (15.1–16.5) 15.3 (14.8–15.9) 19.5 (19.0–20.0) Mean±SD 11.9±1.9 12.8±1.5 15.3±2.1 Q-95 (CI) 15.1 (14.3–16.0) 15.3 (14.7–16.0) 19.5 (18.5–20.5) 15.5 (15.1–15.9) 15.5 (15.0–15.6) 19.5 (19.0–20.0) Women Mixed Q-95 (CI) RA area index, cm /m 2 2 Men Mean±SD 6.7±1.0 6.9±0.9 8.3±1.1 Q-95 (CI) 8.4 (8.1–8.8) 8.3 (8.0–8.6) 10.4 (10.1–11.0) Women Mean±SD 6.5±1.0 7.0±0.8 8.2±1.1 Q-95 (CI) 8.2 (7.7–8.6) 8.3 (8.0–8.6) 10.4 (9.9–11.1) 8.3 (8.1–8.5) 8.2 (8.1–8.5) 10.4 (10.1–10.7) Mixed Q-95 (CI) CI indicates confidence interval; Q-95, 95% quantile; and RA, right atrial. Grünig et al Reference Values of Right Atrial Area 121 Table 3. Mean Absolute and for Body Surface Area-Indexed Right Atrial Area: Pooled Values of Our Analysis and for Pooled Analysis of Selected Studies RA Area, cm2 n Mean±SD Q-95 RA Area Index, cm2/m2 Q-95 (L-CI/U-CI) n Mean Q-95 Q-95 (L-CI/U-CI) Men Nonathletes 378 13.0±1.9 16.2 15.8–16.6 378 7.0±0.9 8.6 8.4–8.8 Ref. 19 Nonathletes 15 13.6±4.7 21.3 16.9–28.2 15 7.1±1.1 8.9 7.9–10.5 Ref. 18 Nonathletes 21 14.0±2.3 17.7 15.9–20.3 21 7.4±1.2 9.4 8.4–10.8 Ref. 21 Nonathletes 50 14.9±1.7 17.7 16.8–18.9 50 8.1±1.0 9.7 9.2–10.4 This study Nonathletes 137 12.5±2.0 15.7 15.1–16.5 137 6.7±1.0 8.4 8.1–8.8 This study Strength 155 12.7±1.6 15.3 14.8–15.9 155 6.9±0.8 8.3 8.0–8.6 Men Endurance This study Endurance 255 15.4±2.1 18.9 18.4–19.5 255 8.3±1.1 10.1 9.8–10.4 Ref. 21 Endurance 50 21.2±4.0 27.8 25.6–30.5 50 10.8±0.9 13.9 12.9–15.2 Women Nonathletes 260 12.2±1.8 15.2 14.7–15.7 260 6.9±1.0 8.5 8.3–8.8 Ref. 19 Nonathletes 15 10.6±2.8 15.2 12.6–19.3 15 6.6±0.9 8.1 7.2–9.4 Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 Ref. 18 Nonathletes 22 11.4±1.6 14.0 12.8–15.9 22 7.0±1.0 8.6 7.8–9.8 Ref. 21 Nonathletes 30 12.2±2.4 16.1 14.5–18.4 30 7.5±1.6 10.1 9.0–11.6 This study Nonathletes This study Strength Women Endurance 93 11.9±1.9 15.1 14.3–16.0 93 6.5±1.0 8.2 7.7–8.6 100 12.8±1.5 15.3 14.7–16.0 100 7.0±0.8 8.3 8.0–8.6 This study Endurance 140 15.3±2.1 18.7 18.0–19.5 140 8.2±1.1 10.0 9.6–10.4 Ref. 21 Endurance 30 16.1±3.6 22.0 19.5–25.3 30 9.4±2.2 13.0 11.5–15.1 Mixed sex Nonathletes 1012 12.6±3.0 17.5 17.1–17.9 987 7.1±1.8 10.1 9.9–10.4 14.5–15.8 Ref. 22 Nonathletes 25 13.9±0.7 15.1 Ref. 23 Nonathletes 11 7.1±0.6 8.0 7.4–9.1 11 4.0±0.3 4.5 4.2–5.1 Ref. 12 Nonathletes 67 13.5±2.0 16.8 15.8–17.9 67 7.7±1.1 9.6 9.0–10.3 Ref. 20 Nonathletes 48 13.0±3.0 17.9 16.3–20.0 48 7.1±1.6 9.8 8.9–10.9 Ref. 24 Nonathletes 15 15.0±7.0 26.5 19.9–36.7 15 8.3±3.9 14.7 11.0–20.4 Ref. 25 Nonathletes 219 11.5±5.0 19.7 18.4–21.2 219 7.4±3.2 12.6 11.8–13.6 BSA indicates body surface area; L-CI/U-CI, lower and upper 95% confidence interval; Q-95, 95% quantile; and RA, right atrial. RA analysis for pooled values does not include endurance athletes. their 95% CIs for all studies used in the pooled analysis and for our study population. Furthermore, in each of the identified studies, RA values obtained in the subgroups based on sex and training status are shown. The mean absolute RA area ranged from 4 cm2 (which we considered implausible, so we excluded the values from further calculation)23 to 6.6 cm19 in female nonathletes to 21.2 cm21 in male endurance athletes. In each study, values for the 95% quantiles and CIs were calculated and compared with the values we obtained in our study population in 880 healthy subjects.14 Pooled Values for RA Area Derived From 10 Studies: Pooled Analysis of Previous Data and Prospectively Assessed Healthy Subjects In the heading lines (grey indicated) of Table 3, mean values are given for 378 men, 260 women, and 1012 unknown-sex nonathletes and strength athletes and 305 male and 170 female endurance athletes. We included nonathletes and strength athletes in the normal group because their RA distributions are very similar. The means were derived from values of the 9 studies of the pooled analysis and our own prospective data of 880 healthy subjects. Figure 3 illustrates the 95% quantiles and CIs of RA area assigned to the analyzed studies and subgroups. Overall, in strength/nonstrength athletes, the pooled mean RA area was 12.2±1.8 cm2 in women, 13.0±1.9 cm2 in men, and 12.6±3.0 cm2 in the mixed-sex group (Table 3). Pooled 95% quantiles of RA area were 15.2 cm2 in women, 16.2 cm2 in men, and 17.5 cm2 in mixed sex group (Table 3 and Figure 3). Pooled 95% quantiles of RA areas indexed for BSA were 8.5 cm2/m2 (8.3– 8.8 cm2/m2) in women, 8.6 cm2/m2 (8.4–8.8 cm2/m2) in men, and 10.1 cm2/m2 (9.9–10.4 cm2/m2) in the mixed-sex group. Sensitivity Analysis Without our prospectively obtained data, the reference values for the mixed-sex group were slightly higher, and without the values from Kelly et al,25 they were slightly lower (16.7 cm2). For women, no study had a remarkable influence. The leaveone-out estimates for the reference values for men varied between 15.9 and 18.3 cm2. Discussion To the best of our knowledge, this is the largest data set on RA size in healthy adults (n=880 our study population, n=624 pooled analysis) between 18 and 70 years of age (most of them 122 Circ Cardiovasc Imaging January 2013 Figure 3. Mean values of echocardiographically measured right atrial (RA) area in our data and a pooled analysis of selected previous studies. The figure presents the 95% quantile of the RA area and the range of 95% confidence intervals of our prospective data and previous publications selected for pooled analysis. The values are given for men and women with different training status. Bottom, The pooled values. Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 <50 years of age) up to now. The calculated reference values for RA size obtained by 2-dimensional echocardiography in the apical 4-chamber view are based on almost all prospective and retrospective studies published so far. This is the first study to provide normal reference values for RA area. The study confirms that absolute cutoff values should be determined and used sex-specifically. Absolute cutoff values for RA area in nonathletes/strength athletes were significantly different in women (15 cm2) and men (16 cm2), whereas values indexed for BSA were similar in both sexes (women, 8.5 cm2/m2; men, 8.6 cm2/m2). Age, sex, BSA, and high-level endurance exercise training were identified as determinants of RA area. Top-level endurance athletes exceeded the reference values of RA area for nonathletes and strength athletes and showed no significant differences between men and women. RA size evaluated by 2-dimen sional echocardiography correlated well with rubber casts of heart chambers obtained at autopsy,22 with hemodynamic measurements, and with assessment by magnetic resonance imaging.27 The absolute RA area obtained by echocardiography in the apical 4-chamber view is a reliable and, in most subjects, accurately measurable parameter. It can be obtained even by older echocardiography devices and is of major clinical relevance. This parameter reflects RV function5,8 and is important for follow-up assessment and risk stratification in patients with right-sided heart failure such as patients with pulmonary hypertension.9,10 Furthermore, enlarged RA area belongs to the echocardiographic parameters that might raise or reinforce suspicion of pulmonary hypertension independently of tricuspid regurgitation velocity9,10 and may be an early indicator for primary diseases of the right side of the heart. RA area distinguished healthy subjects from patients with RV volume overload or rightsided heart diseases with only minimal overlap between the groups,8,22,23,25 as long as correct cutoff values were used. Furthermore, an enlarged atrium may be an early indicator of pulmonary hypertension and primary diseases of the right side of the heart. For clinical practice, it is more convenient to measure the absolute area instead of performing the corrections for BSA. Therefore, the finding that women and men have significantly different absolute RA areas is of clinical importance and has already been observed in small cohorts of healthy subjects.18–20 Nevertheless, sex differences in RA size have not been analyzed systematically so far and have not led to different sexspecific reference values.11 This study confirms for the first time sex differences and the influence of age, BSA, and training status on echocardiographic RA area in a large number of healthy adult subjects. Mixed-sex values for absolute RA area11 should therefore not be used any longer to avoid the risk of underestimation of RA enlargement, especially in women. However, no significant sex differences were observed when RA area was corrected for BSA and training status (endurance athletes). Different reference values for men and women have also been documented for echocardiographic RV end-diastolic area.28 Absolute RA area was significantly, but weakly, correlated with age. Older subjects had slightly enlarged RA areas. However, most subjects of this study were <50 years of age. In this cohort, age accounted for only 3% of the variance of values. According to the results of the prospective study and the pooled analysis of all previous studies, there is no need to adapt the reference values of 15 cm2 for women and 16 cm2 for men to age. Nevertheless, further evaluation of children and healthy subjects >50 years of age is necessary to determine normal RA area in these groups. Numerous studies have described “athlete’s heart syndrome” with chamber enlargement of the left and right sides of the heart.29 However, the effect on RA size is less well evaluated. Acute, transient RA and RV dilatation, reduction of Grünig et al Reference Values of Right Atrial Area 123 RV ejection fraction obtained by magnetic resonance imaging, and release of B-type natriuretic peptides30 and cardiac troponin I31 were seen immediately after severe endurance exercise such as marathon running. Ector et al32 proposed that the right ventricle may be more severely affected by endurance training because of its thin-walled structure compared with the left ventricle. Larger RA size compared with that of sedentary control subjects by 2-dimensional echocardiography was also described in professional tennis players participating at the French Open.21 In our study, endurance-trained top-level athletes had substantially larger RA areas with a 95% quantile of 19.5 cm2 compared with that measured in nonathletes and strength athletes. A possible explanation for this might be that endurance training leads to higher volume loads of the RV,29,33 whereas strength athletes generate higher pressures with only transiently increased volume loads.29,33 Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 Limitations The studies included in the pooled analysis had different definitions of “healthy participants.” Right-sided and left-sided heart catheterization was performed in only 1 study.22 Some other studies were retrospective in design, and not all studies aimed to determine reference values, so we cannot exclude a referral bias. These studies caused a larger standard deviation of mean RA areas that is also reflected in the larger 95% percentile for the mixed-sex group in the pooled analysis compared with the values obtained in the prospective study. However, the strength of this article is that the values for RA area selected for pooled analysis have been compared with data that have been prospectively assessed. The prospective examinations used actual standards in the definition of healthy subjects and avoided referral bias by the assessment of subjects who ask for a job certificate. If we had referred to the prospective study only, reference values for absolute RA area would have been slightly smaller than 15 cm2 in women and 16 cm2 in men. The majority of subjects analyzed in the prospective study and in the pooled analysis were young (<45 years of age). There is a lack of data describing RA area in children or subjects >50 years of age. In older subjects, the definition of “healthy” would need a detailed diagnostic workup, including right-sided and left-sided heart catheterization. However, the findings in the study of Bommer et al22 indicate that RA area in subjects of older age do not significantly exceed the reference values confirmed in this study. Only a few studies have been excluded from this pooled analysis. Their values obtained for RA area would not have changed the reference values obtained in the analysis. We chose the 95% quantiles as normal reference values because the largest 5% of values may indicate pathological processes. Another quantile such as 97.5% could have been considered but would have changed the resulting reference values only slightly. Conclusions To the best of our knowledge, this is the largest data set to describe RA size in adult healthy subjects (<50 years of age). Cutoff values for RA area were significantly different in women (15 cm2) and men (16 cm2); therefore, sex-specific values should be used in the future. Age, sex, BSA, and high-level endurance training were determinants of RA area. Further studies in children and subjects >50 years of age are needed. Disclosures None. References 1. Bustamante-Labarta M, Perrone S, De La Fuente RL, Stutzbach P, De La Hoz RP, Torino A, Favaloro R. Right atrial size and tricuspid regurgitation severity predict mortality or transplantation in primary pulmonary hypertension. J Am Soc Echocardiogr. 2002;15(pt 2):1160–1164. 2. Raymond RJ, Hinderliter AL, Willis PW, Ralph D, Caldwell EJ, Williams W, Ettinger NA, Hill NS, Summer WR, de Boisblanc B, Schwartz T, Koch G, Clayton LM, Jöbsis MM, Crow JW, Long W. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol. 2002;39:1214–1219. 3. Grapsa J, Gibbs JS, Cabrita IZ, Watson GF, Pavlopoulos H, Dawson D, Gin-Sing W, Howard LS, Nihoyannopoulos P. The association of clinical outcome with right atrial and ventricular remodelling in patients with pulmonary arterial hypertension: study with real-time three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging. 2012;13:666–672. 4. Guerra VC, Coles J, Smallhorn JF. Aneurysm of right atrium diagnosed by 3-dimensional real-time echocardiogram. J Am Soc Echocardiogr. 2005;18:1221. 5. Gaynor SL, Maniar HS, Prasad SM, Steendijk P, Moon MR. Reservoir and conduit function of right atrium: impact on right ventricular filling and cardiac output. Am J Physiol Heart Circ Physiol. 2005;288:H2140–H2145. 6. Gaynor SL, Maniar HS, Bloch JB, Steendijk P, Moon MR. Right atrial and ventricular adaptation to chronic right ventricular pressure overload. Circulation. 2005;112(suppl):I212–I218. 7. Kushner FG, Lam W, Morganroth J. Apex sector echocardiography in evaluation of the right atrium in patients with mitral stenosis and atrial septal defect. Am J Cardiol. 1978;42:733–737. 8. Cioffi G, de Simone G, Mureddu G, Tarantini L, Stefenelli C. Right atrial size and function in patients with pulmonary hypertension associated with disorders of respiratory system or hypoxemia. Eur J Echocardiogr. 2007;8:322–331. 9. Grünig E, Barner A, Bell M, Claussen M, Dandel M, Dumitrescu D, Gorenflo M, Holt S, Kovacs G, Ley S, Meyer JF, Pabst S, Riemekasten G, Saur J, Schwaiblmair M, Seck C, Sinn L, Sorichter S, Winkler J, Leuchte HH. Non-invasive diagnosis of pulmonary hypertension: ESC/ERS guidelines with updated commentary of the Cologne Consensus Conference 2011. Int J Cardiol. 2011;154(suppl 1):S3–12. 10. Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34:1219–1263. 11.Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713; quiz 786. 12. Triulzi MMD, Gillam LD, Gentile F, Newell JB, Weyman BS, Weyman AE. Normal adult cross-sectional echocardiographic values: linear dimensions and chamber areas. Echocardiogr Rev Cardiovasc Ultrasound. 1984;1:403–426. 13. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ; Chamber Quantification Writing Group; American Society of Echocardiography’s Guidelines and Standards Committee; European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463. 14. D’Andrea A, Riegler L, Golia E, Cocchia R, Scarafile R, Salerno G, Pezzullo E, Nunziata L, Citro R, Cuomo S, Caso P, Di Salvo G, Cittadini A, Russo MG, Calabrò R, Bossone E. Range of right heart measurements in 124 Circ Cardiovasc Imaging January 2013 Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 top-level athletes: the training impact [published online ahead of print July 5, 2011]. Int J Cardiol. doi:10.1016/j.ijcard.2011.06.058. 15. Yock PG, Popp RL. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation. 1984;70:657–662. 16. Ommen SR, Nishimura RA, Hurrell DG, Klarich KW. Assessment of right atrial pressure with 2-dimensional and Doppler echocardiography: a simultaneous catheterization and echocardiographic study. Mayo Clin Proc. 2000;75:24–29. 17. Du Bois D, Du Bois EF. A formula to estimate the approximate surface area if height and weight be known; 1916. Nutrition. 1989;5:303–311. 18. Lambertz H, Heiliger R, Flachskampf FA, Wohltmann D, Krebs W, Mittermayer C. A new echocardiographic procedure for calculation of the accurate volume of the right atrium. Z Kardiol. 1986;75:342–354. 19. Lambertz H, Krebs W, Soeding S, Wohltmann D, Sechtem U, Kemmer HP. Determination of the size of the right atrium in patients with pulmonary hypertension using 2-dimensional echocardiography. Z Kardiol. 1984;73:646–653. 20. Wang Y, Gutman JM, Heilbron D, Wahr D, Schiller NB. Atrial volume in a normal adult population by two-dimensional echocardiography. Chest. 1984;86:595–601. 21. Mansencal N, Marcadet DM, Martin F, Montalvan B, Dubourg O. Echocardiographic characteristics of professional tennis players at the Roland Garros French Open. Am Heart J. 2007;154:527–531. 22. Bommer W, Weinert L, Neumann A, Neef J, Mason DT, DeMaria A. Determination of right atrial and right ventricular size by two-dimensional echocardiography. Circulation. 1979;60:91–100. 23. Cacho A, Prakash R, Sarma R, Kaushik VS. Usefulness of two-dimensional echocardiography in diagnosing right ventricular hypertrophy. Chest. 1983;84:154–157. 24. Huez S, Faoro V, Guénard H, Martinot JB, Naeije R. Echocardiographic and tissue Doppler imaging of cardiac adaptation to high altitude in native highlanders versus acclimatized lowlanders. Am J Cardiol. 2009;103:1605–1609. 25. Kelly NF, Walters DL, Hourigan LA, Burstow DJ, Scalia GM. The relative atrial index (RAI): a novel, simple, reliable, and robust transthoracic echocardiographic indicator of atrial defects. J Am Soc Echocardiogr. 2010;23:275–281. 26. Reeves WC, Hallahan W, Schwiter EJ, Ciotola TJ, Buonocore E, Davidson W. Two-dimensional echocardiographic assessment of electrocardiographic criteria for right atrial enlargement. Circulation. 1981;64:387–391. 27. Keller AM, Gopal AS, King DL. Left and right atrial volume by freehand three-dimensional echocardiography: in vivo validation using magnetic resonance imaging. Eur J Echocardiogr. 2000;1:55–65. 28. Ogunyankin KO, Liu K, Lloyd-Jones DM, Colangelo LA, Gardin JM. Reference values of right ventricular end-diastolic area defined by ethnicity and gender in a young adult population: the CARDIA study. Echocardiography. 2011;28:142–149. 29. Baggish AL, Wood MJ. Athlete’s heart and cardiovascular care of the athlete: scientific and clinical update. Circulation. 2011;123:2723–2735. 30. La Gerche A, Burns AT, Mooney DJ, Inder WJ, Taylor AJ, Bogaert J, Macisaac AI, Heidbüchel H, Prior DL. Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur Heart J. 2012;33:998–1006. 31. Trivax JE, Franklin BA, Goldstein JA, Chinnaiyan KM, Gallagher MJ, deJong AT, Colar JM, Haines DE, McCullough PA. Acute cardiac effects of marathon running. J Appl Physiol. 2010;108:1148–1153. 32. Ector J, Ganame J, van der Merwe N, Adriaenssens B, Pison L, Willems R, Gewillig M, Heidbüchel H. Reduced right ventricular ejection fraction in endurance athletes presenting with ventricular arrhythmias: a quantitative angiographic assessment. Eur Heart J. 2007;28:345–353. 33. Roy A, Doyon M, Dumesnil JG, Jobin J, Landry F. Endurance vs. strength training: comparison of cardiac structures using normal predicted values. J Appl Physiol. 1988;64:2552–2557. Clinical Perspective Right atrial size is important in several indications such as screening, diagnosis, and follow-up assessment of patients with pulmonary hypertension. This is the first study to provide normal reference values for right atrial area in a large number of healthy subjects. Sex differences and the influence of age, body surface area, and training status on echocardiographic right atrial area are confirmed for the first time. Because an enlarged atrium may be an early indicator for pulmonary hypertension or primary diseases of the right heart, the results are of high clinical impact. For clinical practice, it is more convenient to measure the absolute area instead of performing corrections for body surface area. Therefore, the finding that women and men have significantly different absolute right atrial areas is of clinical importance. Cutoff values for right atrial area were significantly different in women (15 cm2) and men (16 cm2); therefore, sex-specific values should be used in the future. Reference Values for and Determinants of Right Atrial Area in Healthy Adults by 2-Dimensional Echocardiography Ekkehard Grünig, Philipp Henn, Antonello D'Andrea, Martin Claussen, Nicola Ehlken, Felicitas Maier, Robert Naeije, Christian Nagel, Felix Prange, Johannes Weidenhammer, Christine Fischer and Eduardo Bossone Downloaded from http://circimaging.ahajournals.org/ by guest on May 14, 2017 Circ Cardiovasc Imaging. 2013;6:117-124; originally published online November 29, 2012; doi: 10.1161/CIRCIMAGING.112.978031 Circulation: Cardiovascular Imaging is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-9651. Online ISSN: 1942-0080 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circimaging.ahajournals.org/content/6/1/117 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Imaging can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Imaging is online at: http://circimaging.ahajournals.org//subscriptions/