Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
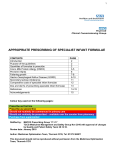
A GUIDE FOR PRESCRIBING SPECIALIST FORMULAS IN PRIMARY CARE FOR THE DIAGNOSIS, TREATMENT AND MANAGEMENT OF COWS’ MILK PROTEIN ALLERGY Authors: Chris Smith Paediatric Dietician Royal Alexandra Children’s Hospital, Dr Assad Butt Consultant Paediatric Gastroenterologist REFERRALS TO RACH All children requiring longer term elimination diets e.g. > 6 weeks should be referred to paediatric Dietitians. Children with severe symptoms or anaphylaxis should be referred to speciality allergy and gastroenterology services. BACKROUND Making the right choice of formula for infants presenting with cows’ milk protein allergy (CMPA) is important in both the infants’ best interests and the financial implication on the NHS. The incidence of CMP (Cows ‘milk protein) allergy appears to peak in the first year of life with a prevalence of around 2% to 7% in the infant population. Recognition of the condition has been greatly increased in the UK in part due to several well established guidelines on its identification and management. ASSESSMENT AND DIAGNOSIS Clear and established algorithms guide the management pathways. Full clinical guidelines can be found at the following: MAP GUIDELINES http://www.ctajournal.com/content/3/1/23 Diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy - a UK primary care practical guide. 2013 NICE http://guidance.nice.org.uk/CG116 In most cases with suspected CMPA the diagnosis needs to be confirmed or excluded by an allergen elimination and challenge procedure. Royal Alexandra Children’s Hospital Algorithm for the Diagnosis and Management of Cows’ Milk Protein Allergy SUSPICION OF MILD TO MODERATE CMPA One or more of the following symptoms: Gastrointestinal: frequent regurgitation, vomiting, diarrhoea, constipation (without perianal rash), blood in stool, iron deficiency anaemia Dermatological: atopic dermatitis General: persistent distress or colic (> 3 hours per day walling/irritable) at least 3 days/week over a period of > 3 weeks Others: (rare) ELIMINATION DIET BREASTFEEDING Elimination diet in mother Elimination diet in mother – no CMP plus Ca-supplement FORMULA FED-INFANTS Therapeutic Extensive Hydrolysed Formula (eHF) 2 to 4 weeks elimination IMPROVEMENT Challenge If acute and objective symptoms of skin (acute urticaria, angioedema), respiratory tract (stridor, wheezing) or systemic reactions (anaphylaxis) occur immediately, or up to 2 hours after a clear history of ingesting dairy products, then CMP should be strictly excluded. In this situation, the oral challenge test can be omitted. NO CMPA SYMPTOMS Resume CMP in diet and monitor NO IMPROVEMENT An allergic reaction to the remaining peptides in the eHF must be considered, particularly in infants with sensitisation against multiple foods. Amino Acid Formula (AAF) Minimal for 2-4 weeks CMPA SYMPTOMS Maintain CMP elimination diet until 9 to 12 months of age, but for at least 6 months. Refer to dietician for advice on management. IMPROVEMENT Refer to dietician for advice on management. NO IMPROVEMENT Unlikely to be CMPA consider differential diagnosis and refer to specialist SUSPICION OF SEVERE CMPA One or more of the following symptoms: Gastrointestinal: Failure to thrive due to chronic diarrhoea, and/or regurgitation/vomiting and or refusal to feed; iron deficiency anaemia due to occult or macroscopic blood loss; protein losing enteropathy (hypoalbuminaemia); endoscopic/histologically confirmer enteropathy or severe allergic colitis Dermatological: Exudative or severe atopic dermatitis with hypoalbuminaemia-anaemia or failure to thrive or iron deficiency anaemia Respiratory: Acute layngoedema or bronchial obstruction with difficulty in breathing Systemic reaction (anaphylactic shock – needs immediate referral to hospital for management) ELIMINATION DIET Amino Acid Formula (AAF) Minimal for 2-4 weeks REFERRAL TO PAEDIATRIC SPECIALIST TREATMENT + PRESCRIPTIONS HIG FIRST LINE EXTENSIVELY HYDROLYSED FORMULAE (lactose free) SECOND LINE EXTENSIVELY HYDROLYSED FORMULAE (containing lactose) * EXTENSIVELY HYDROLYSED FORMULAE WITH MEDIUM CHAIN TRIGLYCERIDES TO BE STARTED IN SECONDARY CARE. AMINO ACID FORMULAE NORMALLY (1) TO BE STARTED IN SECONDARY CARE. Nutramigen Lipil 1 Birth to 6 months (Mead Johnson) Nutramigen Lipil 2 * 6 months onwards (Mead Johnson) * Higher calcium content in this formula likely to be required due to restriction of dairy foods in weaning diet. Requires dietetic assessment. First line for patient with severe CMPA is amino acid formula (See AMINO ACID box below) NOTE- Alternative extensively hydrolysed formulas available nationally but not on local formulary are: Similac Alimentum (Abbott), Althera (SMA) Pepti 1 Birth to 6 months (Cow and Gate) Pepti 2 6 months to 1 year (Cow and Gate) *These formulas may be tried if infant is not tolerating first line products because of refusal associated with taste. Pepti Junior ® (Cow and Gate) Birth to 2 years or birth to 1 year if can then tolerate over the counter suitable milk alternatives ® Pregestimil Lipil Birth to 2 years or birth to 1 year if (Mead Johnson) can then tolerate over the counter suitable milk alternatives These formulas are used where CMPA is accompanied by malabsorption. Neocate LCP (Nutricia) Neocate Active® (Nutricia) (2) Neocate Advance® (Nutricia) (3) Birth to 1 year 1 year onwards 1 year onwards 1. If a patient presents with clear anaphylactic reaction to cow’s milk these formula should be commenced in primary care, with immediate onward referral to secondary or specialist care. 2. Neocate Active® is a high calorie formula and will not be required automatically by all infants over 1 year. It is not suitable as a sole source of nutrition. Seek dietetic advice. 3. Neocate Advance® is a sole source of nutrition for patients with CMPA aged 1-10 years. It is a high calorie product and will not be required automatically by all patients over 1 year. Seek dietetic advice. 4. If formula top-ups are needed for a child who is otherwise breastfed (mother on a milk free diet) AAF will be required. NOTE- Alternative amino acid formulas available nationally but not on local formulary are: Nutrmigen AA (Mead Johnson), Alfamino (SMA) Non–Specialist Drugs Specialist Initiation WITHOUT Shared Care Drugs Specialist Initiation WITH Shared Care Drugs Specialist ONLY Drugs RGY FORMULA IRST-LINE GUIDE TO PRESCRITION VOLUMES Age of child Number of tins for 28 days Under 6 months 13 x 400g tins or 6 x 900g tins 6-12 months 7-13 x 400g tins or 3-6 x 900g tins Over 12 months 7 x 400g tins or 3 x 900g tins DURATION OF ELIMINATION DIET The duration of a diagnostic elimination diet (either mother restriction in a breast fed case or use of an extensively hydrolysed in a bottle fed) depends on manifestation and should be kept as short as possible, but long enough to judge whether clinical symptoms resolve or not or become stable. This ranges from 3 – 5 days in children with immediate clinical reactions (e.g. angioedema, vomiting or exacerbation of eczema within 2 hours) to 1 – 2 weeks in children with delayed clinical reactions (e.g. exacerbation of eczema, rectal bleeding). In patients with gastrointestinal reactions (e.g. chronic diarrhoea, growth faltering) it may take 2 to 4 weeks on a CMP free diet to judge on the response. If there is no improvement in symptoms within these timelines, CMPA is unlikely. FOLLOW UP AND RESOLUTION Patients should be re-evaluated every 6 – 12 months to assess whether they have developed tolerance to CMP. This is achieved in >75% of children by three years and >90% by six years of age. LACTOSE AND CMPA Adverse reactions to lactose in CMPA are not supported in the literature and complete avoidance of lactose in CMPA is not warranted. These formulae may also be more palatable for infants over 6 months. It is however possible for secondary lactose intolerance to co-exist in infants who have enteropathy with diarrhoea and therefore a lactose-free eHF will be required initially in these cases. SECONDARY LACTOSE INTOLERANCE (Adapted from PrescQipp) Symptoms and diagnosis • Lactose intolerance is defined as a non-immune mediated adverse reaction to food i.e. it is not due to allergy but a lack of the enzyme lactase. • Usually occurs following an infectious gastrointestinal illness but may be present alongside newly or undiagnosed coeliac disease. • Symptoms include abdominal bloating, increased (explosive) wind, loose green stools. • Lactose intolerance should be suspected in infants who have had any of the above symptoms that persist for more than 2 weeks. • Resolution of symptoms within 48 hours of withdrawal of lactose from the diet confirms diagnosis. Onward referral • If symptoms do not resolve when standard formula and/or milk products are reintroduced to the diet, refer to secondary or specialist care. • Refer to the paediatric dietitian if the child is weaned and a milk free diet is required. Treatment • Treat with low lactose/lactose free formula not a hypoallergenic formula) Appropriate formulas include Enfamil OLac (Mead Johnson) or SMA Lactofree. These are a similar price to standard formulas and parents should be encouraged to buy them •Treat for 4-8 weeks to allow symptoms to resolve. Rarely symptoms may last up to 3 months • In infants who have been weaned, low lactose/lactose free formula should be used in conjunction with a milk free diet. • Standard formula and/or milk products should then be slowly reintroduced to the diet. • In children over 1 year who previously tolerated cow’s milk, do not prescribe low lactose/lactose free formulae. Suggest use of lactose free full fat cow’s milk, yoghurt and other dairy products which can be purchased from supermarkets (Lactofree® brand). REFERENCES 1) Venter et al. Diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy - a UK primary care practical guide Clinical and Translational Allergy 2013 3:23 2) Koletzko B, et al. Diagnostic Approach and Management of Cow’s-Milk Protein Allergy in Infants and Children: ESPGHAN GI Committee Practical Guidelines. Journal of Paediatric Gastroenterology and Nutrition. Volume 55, Number 2, August 2012 3)Fiocchi A et al. World Allergy organization (WAO) diagnosis and rationale for action against Cow's milk allergy (DRACMA) guidelines. World Allergy Organ J 2010, 3(4):57-161. 4) Sladkevicius E et al. Resource implications and budget impact of managing cow milk allergy in the UK. J Med Econ 2010, 13(1):119-128 5)Allen KJ et al. Management of cow's milk protein allergy in infants and young children: an expert panel perspective. J Paediatr Child Health 2009, 45(9):481-486. Prepared Aug 2014 Reviewed Aug 2015 Date for review Aug 2016