Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
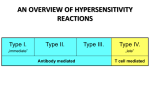
Hypersensitivity and Autoimmunity Aims & Objectives: • Understand the terms hypersensitivity, allergy, autoimmunity and autoimmune disease • Understand the classification and mechanisms of immunologically mediated tissue damage (hypersensitivity reactions), and know examples of diseases reflecting each of these • Understand what we mean by organ specific and non-organ specific autoimmune diseases, and know examples of both Definitions: Hypersensitivity: exaggerated or inappropriate immune reaction resulting in tissue damage Allergy: hypersensitivity reaction to an extrinsic (often innocuous) antigen Autoimmunity: immune response with specificity for self antigen(s) Autoimmune disease: disease in which an autoimmune response plays a pathogenetic role Hypersensitivity reactions – the mechanisms of allergy and autoimmunity (Gell and Coombs classification) Types of hypersensitivity reactions Type I: Type II: Type III: Type IV: anaphylactic or immediate cytotoxic Immune complex cell mediated or delayed 5 Type I (immediate) hypersensitivity reactions Mechanism of type I hypersensitivity Extrinsic allergen pollens house dust mite animal dander foods (eg peanut) wasp / bee venom IgE Th2 response IL-4 / IL-13 mast cells Priming sensitization elicitation Mediators of type I hypersensitivity vasodilatation increased vascular permeability tissue oedema smooth muscle contraction chemoattraction Most allergic reactions occur at mucosal sites (site of interaction with allergen) Sensitization against allergens and type-I hypersensitivity B cell TH2 Histamine, tryptase, kininegenase, ECFA Leukotriene-B4, C4, D4, Newly prostaglandin D, PAF synthesized mediators 9 Allergic rhinitis (Hay fever) Anaphylaxis – systemic type I hypersensitivity: a medical emergency Clinical features of anaphylaxis: Generalized urticaria Angioedema esp. around eyes, lips, tongue and larynx Gastrointestinal symptoms (nausea, cramps, vomiting, diarrheoa) Bronchospasm Hypotension i.m. injection of adrenaline (1:1000) Loss of consciousness Death plus i.v. antihistamine, i.v.hydrocortisone and oxygen Skin (prick) test for allergy 12 Type II (antibody mediated) hypersensitivity Antibody to tissue bound or cellular antigen: Type II hypersensitivity role of complement and phagocytes 14 Type II hypersensitivity induced by exogenous agents 15 Mechanism and prevention of Rhesus disease Rhesus disease of the newborn – a type II hypersensitivity disease Stimulatory and blocking antibodies in type II hypersensitivity Stimulatory Abs TSH receptor in Grave’s disease Blocking Abs ACh R in myasthenia gravis intrinsic factor in pernicious anaemia insulin receptor in diabetes Myasthenia gravis the mechanism Grave’s disease Type III (immune complex) mediated hypersensitivity Soluble antigen Immune complexes deposit in small vessels (esp joints, kidneys, skin) Complement activation Neutrophil attraction and activation Platelet aggregation and microthrombus formation Type III hypersensitivity mechanism 22 Arthus reaction Arthus reaction Type-III Weal & flare reaction Type-I 23 Serum sickness 24 Early and late joint changes in rheumatoid arthritis Typical “butterfly” malar rash in SLE Type IV (delayed) hypersensitivity Type IV hypersensitivity Delayed reaction 36 to 48 hours Characterized by induration and erythema Also known as cell mediated hypersensitivity Tuberculin test is the most common example 28 Tuberculin test 29 Contact hypersensitivity (to nickel) Contact dermatitis reaction to leather 31 Granuloma in a leprosy patient 32 Type IV hypersensitivity and coeliac disease Type IV hypersensitivity the three forms 34 “Patch” testing for contact hypersensitivity Summary or hypersensitivity reactions Autoimmunity and autoimmune disease Peripheral tolerance Autoantibodies and disease • presence of antibodies to self antigens indicates an autoimmune process or reaction • but does not necessarily equate with presence of disease (eg low titre ANA in elderly or after infection) • some (but not all) autoantibodies cause disease (pathogenetic) • some autoantibodies provide useful diagnostic markers of disease (often in association with other clinical features) • some autoantibodies can be used to monitor disease activity (often pathogenetic antibodies) • some autoantibodies have a higher predictive value than others (eg IgA endomysial Ab vs IgA gliadin Ab vs reticulin Ab in coeliac disease) • autoantibodies to many autoantigens are found (in low titres) in the elderly in the absence of disease (eg ANA) Comparison of organ specific and non-organ specific autoimmune diseases Organ specific Non-organ specific Antigen localized to given organ or tissue widespread distribution throughout the body Lesions confined to target organ or tissue multiple organs / tissues affected; immune complexes deposit in joints, skin and kidneys Overlap with other organ specific antibodies and diseases overlap with other non-organ specific antibodies and diseases Examples autoimmune thyroid disease (Grave’s; Hashimoto’s) myasthenia gravis pernicious anaemia diabetes mellitus SLE rheumatoid arthritis systemic sclerosis systemic vascultitis Autoantibodies and autoimmunity (Some) autoantibodies of clinical significance in organ specific and non-organ specific autoimmune disease: Antigen thyroid peroxidase TSH receptor islet cell acetyl choline R t transglutaminase / endomysial basement membrane mitochondrial (M2) ANCA (MPO / PR3) “rheumatoid factor” dsDNA Distribution thyroid gland thyroid gland pancreas neuromuscular junction GI tract Disease Hashimoto’s thyroiditis Grave’s disease type I diabetes myasthenia gravis coeliac disease kidney / lung all cells neutrophils immunoglobulin Fc all cells Goodpastures syndrome 1o biliary cirrhosis systemic vasculitis rheumatoid arthritis SLE Causes of autoimmunity – breakdown of self tolerance Molecular mimicry: cross reactivity between pathogen and self antigen Defective immunoregulation: aberrant Ag presentation by dendritic cells (failure of) regulatory T cells cytokines: excess immune stimulation lack of suppression Exposure of “hidden” self antigens: eg sympathetic opthalmia T cell bypass / hapten: eg drug induced autoimmune cytopenias Genetic susceptibility: HLA and non-HLA genes In most cases, trigger not known Summary • autoimmune reactions and diseases are relatively common, and represent a breakdown of immunological tolerance • autoimmunity can be organ-specific or non-organ specific, depending on the distribution of the autoantigen • allergic represents an exaggerated immune response to extrinsic antigen. Allergic diseases are common, and are becoming more common (especially in children) • allergic and autoimmune diseases are mediated by mechanisms of hypersensitivity • hypersensitivity reactions represent exaggerated or inappropriate immune reactions, resulting in tissue damage Summary • Four major types of hypersensitivity reaction have been defined, depending on the underlying immunological mechanism Type I IgE Type II IgG Type III Ag-Ab complexes Type IV delayed / T cell mediated • Anaphylaxis (systemic type I hypersensitivity reaction) represents a medical emergency, is potentially lifethreatening, and is effectively treated with i.m. adrenaline • In many autoimmune diseases, there is overlap between different types of hypersensitivity reaction