Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
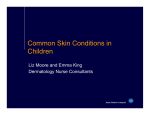
PRESCRIBING IN CHILDREN n Management of atopic eczema in children REBECCA PHILLIPS, HYWEL WILLIAMS and JANE RAVENSCROFT Atopic eczema is a common condition, affecting about a fifth of children in the UK. Although the severity varies, it can cause great distress to a child and their family. This article discusses the evidencebased management of atopic eczema in children. A topic eczema, or atopic dermatitis, is a very common chronic inflammatory skin condition with a genetic tendency that is influenced by environmental factors. Around 20 per cent of UK children are affected, with most presenting in infancy. The symptoms can cause a great deal of distress to both a child and their family. Up to 60 per cent of children will grow out of the condition by early adolescence although many will have future relapses. While the severity of the condition varies greatly, most children will suffer with mild disease and the majority of these patients rely on primary care input. Atopic eczema is characterised by skin dryness, itching, redness, vesicles and crusting in the acute stage, and lichenification in the chronic phase. The clinical presentation of eczema varies depending on the age of the child affected; infants under the age of one year usually present with eczema on the cheeks and scalp, whereas in those older than one year, eczema often extends to affect the extensor surfaces. In older children, eczema may become more widespread and typically involves the flexural surfaces (see Figure 1). Simple validated diagnostic criteria have been developed that may assist in diagnosis (see Table 1).1 prescriber.co.uk Figure 1. Moderate-to-severe eczema in a 9-year-old girl This article focuses on the management of atopic eczema in children. It presents the evidence supporting current interventions and proposes treatment approaches for example cases. Aim of management The aim of the management in atopic eczema is first, to get control of skin inflammation and second, to then maintain control while at the same time enhancing the skin hydration and barrier through emollient use. This management approach first involves identifying and minimising potential trigger factors. Once allergic or irritant factors are identified and dealt with, Prescriber January 2016 z 33 n PRESCRIBING IN CHILDREN l Eczema Must have: An itchy skin condition in the last 12 months Plus three or more of: i. Onset below age two years* ii. History of flexural involvement iii. History of a generally dry skin iv. Personal history of other atopic disease** v. visible flexural dermatitis as per photographic protocol * not used in children under four years ** in children aged under four years, history of atopic disease in a first-degree relative may be included Table 1. UK diagnostic criteria for atopic eczema1 the key is then to control skin inflammation. The NICE guideline presents a stepwise management approach to eczema depending on the severity, as shown in Table 2. Patient and family education, along with a clear written care plan, are vital to ensure a good understanding of the condition, compliance and effective management of future flares. This is particularly important, as topical treatments can be time-consuming and messy. It is also imperative to address any potential fears regarding side-effects of medications, such as topical steroids, which may hinder adequate treatment. Table 3 outlines the factors to consider when managing a child with atopic eczema and Table 4 summarises the treatment approaches in mild-to-moderate and moderate-to-severe eczema flares. Management of mild-tomoderate eczema Emollients Liberal use of emollient therapy in managing eczema is currently recommended but should be tailored according to the individual patient and degree of skin dryness. Even though the evidence for using these products is limited, recent studies have highlighted the steroid-sparing effects of emollient therapy and their ability to prevent eczema flares.2,3 Emollients are safe to use and have few adverse effects, which are usually mild and include transient burning and poor cosmetic acceptability. However, some emollients such as the aqueous cream have actually been shown to cause harm.4 Because emollients need to be applied daily and lifelong, patients should be given a choice of emollients and more than one may need to be prescribed, for example, a different emollient for the face and body. Topical corticosteroids Topical corticosteroids have been shown to be significantly more effective at treating patients with atopic eczema in the short-term compared with placebo.5 Intermittent treatment with fluticasone propionate using various regimens has been shown to significantly reduce relapse rates of eczema.6 Such intermittent use (also known as “weekend therapy” as it refers to application at previously active sites on two to three days a week) is perhaps one of the most useful Mild atopic eczema Moderate atopic eczema Severe atopic eczema Emollients Emollients Emollients Mild-potency topical corticosteroids Moderate-potency topical corticosteroids used proactively Potent topical corticosteroids Topical calcineurin inhibitors Topical calcineurin inhibitors Bandages Bandages Phototherapy Systemic therapy Table 2. NICE guideline: a stepwise approach to the management of atopic eczema13 34 z Prescriber January 2016 evidence-based treatment approaches to emerge for those with chronic or relapsing eczema. All patients should be started on once daily treatments as twice daily applications have shown no additional benefits.6 Pulsed treatment has also not shown any benefit over continuous treatment, and there is no good evidence to support dilution of preparations. Shortterm treatment is not associated with any serious systemic effects or skin atrophy.6 It should be stressed that side-effects of topical corticosteroids rarely occur when they are used appropriately and it is important to dispel any anxieties surrounding their use. The largest eczema trial ever conducted showed that mild or moderate topical corticosteroids are extremely safe when used as needed over a five-year period; just one case of clinical skin thinning out of 1213 children (0.1 per cent) was noted.7 Bandaging Application of wet-wrap bandaging over emollients or topical steroids may be of some benefit to certain patients. Studies have shown that bandaging can significantly reduce the severity of the condition; however, other studies have found no benefit.8-10 Oral antihistamines There seems to be no clear benefit of administering oral antihistamines and these are not recommended. However, the sedative effect may be of some benefit in individual cases.6 Topical tacrolimus and pimecrolimus Topical tacrolimus (Elidel) and pimecrolimus (Protopic 0.03% and 0.1%) are immunosuppressive agents. Both have been shown to be more effective than placebo. Topical tacrolimus is more effective than topical pimecrolimus and of similar efficacy to mild or moderate corticosteroids in the treatment of eczema.11,12 Topical pimecrolimus is aimed at milder atopic eczema where its main claimed advantage is absence of skin thinning, yet a direct comparison of topical pimecrolimus against mild or moderate topical corticosteroids did not show any significant skin thinning in the prescriber.co.uk Eczema corticosteroid group.7 NICE recommends both topical tacrolimus and pimecrolimus as second-line therapy in moderately severe and severe eczema.13 Various safety studies have demonstrated that shor t-term use of tacrolimus is safe and there is no clear evidence of increased risk of skin malignancy. 6 The precise role of topical pimecrolimus for mild eczema is unclear, although it appears to be safe over a five-year period. Higher potency 0.1% tacrolimus is more likely to cause local skin burning and irritation than 0.03% tacrolimus or moderate potency topical corticosteroids.11 In clinical practice, topical tacrolimus may be useful as an alternative for patients requiring almost continuous topical preparations or in those with resistant facial eczema. Lower potency 0.03% tacrolimus is licensed for use in children from the age of two years, while 0.1% tacrolimus is licensed only for children aged 16 years and above. They should be used once or twice daily until symptoms have resolved or can be used intermittently to prevent flares. These medications should usually be initiated under the guidance of a GP with a special interest (GPSI) in dermatology or a dermatologist. Allergens Sensitisation to aeroallergens and food allergens is present in 70–80 per cent of children with moderate-to-severe eczema, but this does not imply clinical allergy, which is best assessed through thorough questioning.14 Common food allergens in young children include cow’s milk, egg, peanuts, soya and tree nuts, while allergies to fish, tree nuts and peanuts are more frequent in older children. Many children will grow out of milk and egg allergies by the age of about three years.14 A food allergy should be considered in children with a history of a reaction to certain foods, those with moderate-to-severe eczema who have not responded to usual treatment, those with early-onset eczema in infancy and those with associated gut symptoms. There is no evidence that exclusion diets have a beneficial impact on eczema in unselected patients. 15 However, in infants with a suspected prescriber.co.uk l PRESCRIBING IN CHILDREN n Factor Comment Age of child Severity of eczema Pattern of eczema •S ide-effects are more common in young infants • Important to prescribe a steroid of adequate potency • Discoid and extensor eczema are often more stubborn and require longer or more aggressive treatment with topical agents • To guide emollient use • To guide future treatment Skin dryness Previous treatments and their effect Possible trigger factors, eg irritants, allergens, stress, infections Compliance/attitudes Psychosocial impact Growth and development Sleep disturbance Personal history of atopic disease •D iscuss avoidance of triggers and consider referral for allergy assessment if indicated •P arents may have preconceived ideas about eczema or treatments • The psychosocial impact on the child and family should be explored. Consider involving school nurses • Severe eczema may affect the growth of a child • Poor sleep can have a negative psychological impact • Consider and treat co-morbidities in children with atopic disease Table 3. Factors to consider when managing a child with atopic eczema allergy to egg and a positive specific IgE test, exclusion diets may help.6 Children with suspected food allergies should be referred for specialist assessment and advice, which may include skin prick tests and specific IgE tests. A six-toeight week trial of hypoallergenic bottle formula may also be tried in babies with moderate-to-severe eczema younger than six months old.14 Allergy to environmental aeroallergens such as house dust mites, pets and pollens, and to contact allergens such as fragrances and preservatives, is more common in older children. It may be suspected in those with a seasonal or environmental variation in their eczema and those with a particular distribution of eczema. Response to these allergens may also be investigated by skin prick tests, specific IgE or patch testing if indicated, which can help guide advice on allergen avoidance. Evidence for the efficacy of house dust mite reduction methods is limited and of low quality.16 They are generally not recommended as they are time consuming and probably not beneficial.13 Washing and bathing routines There is no randomised controlled trial (RCT) evidence on the effects of bathing frequency, showers versus baths or water temperature.6 Bath additives may appear to be a useful way to use emollients but there is no clear evidence to support their use over and above direct topical application. In practice, patients are advised to avoid soaps and bubble bath and instead to use emollients exclusively to moisturise and wash. Washing powders and clothing There is no evidence to suggest that biological washing powders provoke worsening of eczema compared to nonbiological products.6 Synthetic fibres and rough textiles in clothing may be irritating and should be avoided. Psychological interventions Some psychological interventions may be useful as an adjunct in managing eczema, such as cognitive behavioural therapy (CBT), habit reversal and hypnotherapy.17-19 Severe eczema Systemic therapy and ultraviolet light Systemic immunosuppressive therapy, including ciclosporin, methotrexate, azathioprine, and phototherapy, can be used to gain control of severe atopic eczema. Despite not being licensed for use in children, there is reasonable evidence to suggest that these agents are Prescriber January 2016 z 35 n PRESCRIBING IN CHILDREN l Eczema Case Example of treatment approach Mild-to-moderate eczema flare •L iberal use of emollients and soap substitutes tailored to skin dryness. These should be prescribed regularly and used even when the eczema is not active • Consider infection and triggers • Short bursts (3–7 days) of a mild topical steroid such as hydrocortisone 1% once daily to control flares. If this is not adequate, a moderately potent topical steroid such as clobetasone butyrate 0.05% ointment can be tried using such a reactive approach Moderate-to-severe eczema flare •L iberal use of emollients and soap substitutes as above • Consider infection and triggers • Potent topical corticosteroid such as betnovate valerate 0.1% ointment once daily to eczematous areas of the body for 1–3 weeks until clear, followed by an emollient-only period. Any future flares should be treated with short bursts of the same potent steroid • Areas on the face, axillae and groin should be treated with a moderately potent steroid such as clobetasone butyrate 0.05% ointment to avoid side-effects • In the case of frequent flares, once the initial 1–3 week treatment has been completed, a topical corticosteroid can be continued as weekend therapy (Sat/Sun) to maintain control of the eczema and prevent relapses. Alternatively, Protopic ointment may be used intermittently, eg twice weekly Mon/Thur, to keep control of flares in the same way Antiseptics Antiseptics preparations can be used in patients who suffer with recurrent clinical skin infections but their long-term regular use is not supported by any studies. The use of bleach baths appears to have some benefit in children with moderate-to-severe eczema who have recurrent significant skin infections. 6 One study has recommended that 250ml Milton Sterilising Fluid (containing 2% sodium hypochlorite) is added to a full bath tub (about 120 litres). The patient should soak in the water for 5–10 minutes before rinsing thoroughly, once or twice weekly.24 Aciclovir If a child with eczema is suspected to have a localised herpes simplex infection, oral aciclovir should be commenced.13 Eczema herpeticum presents with widespread, rapidly worsening and painful eczema, clustered vesicles and punched-out lesions. If this is suspected, systemic aciclovir should be started immediately and the patient must be referred for urgent specialist advice.13 Table 4. Treatment approaches in mild-to-moderate and moderate-to-severe eczema References effective. They should be initiated and monitored in a secondary care setting. Short-term (five to seven days) oral prednisolone may be useful in a crisis, but this is not recommended longer term due to rebound.20 Ultraviolet light in the form of narrow-band UVB is commonly used in a hospital setting for those with more severe eczema with inadequate responses to topical therapies. 1. Williams HC. UK diagnostic criteria for atopic dermatitis. Centre of Evidence Based Dermatology, Nottingham (cited 2015). Available at: http://www.nottingham.ac.uk/ research/groups/cebd/resources/ukdiagnostic-criteria-for-atopic-dermatitis.aspx. 2. Grimalt R, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology 2007;214(1):61–7. 3. Wiren K, et al. Treatment with a barrier-strengthening moisturizing cream delays relapse of atopic dermatitis: a prospective and randomized controlled clinical trial. J Eur Acad Dermatol Venereol 2009;23(11):1267–72. 4. Cork MJ, Danby S. Aqueous cream damages the skin barrier. Br J Dermatol 2011;164(6):1179–80. 5. Hoare C, et al. Systematic review of treatments for atopic eczema. Health Technol Assess 2000;4(37):1–191. 6. Williams HC, Bigby ME. Evidence-based Dermatology. 3rd edn. Chichester, West Sussex: John Wiley & Sons, Ltd, 2014. 7. Sigurgeirsson B, et al. Safety and efficacy of pimecrolimus in atopic dermatitis: a 5-year randomized trial. Pediatrics 2015;135(4):597–606. Infected eczema Systemic antibiotics Clinically infected eczema has been shown to respond to systemic anti b i o t i c s , s u c h a s f l u c l o x a c i l l i n . 21 However, there is no benefit for their use in clinically uninfected eczema.22 Patients should continue to use topical corticosteroids and emollients to treat the underlying eczema, although it is reasonable to delay the use of topical corticosteroids by 24–48 hours in cases of widespread or severe infection. Patients with atopic eczema are more prone to acquiring bacterial, viral and fungal skin infections. Infection might present with weeping, oozing and serous crusting overlying the eczematous lesions. Staphylococcus aureus is the most commonly implicated organism, which is found in around 80 per cent of people with atopic eczema even in the absence of clinical infection. Other organisms include β-haemolytic streptococci, herpes simplex and the yeast Malassezia furfur. Topical antibiotics NICE recommends that topical antibiotics, including those in combination with topical steroids, should only be used for short periods (less than 14 days) in cases of clinically infected eczema.13 However, there is no clear evidence that the addition of antibiotics to topical corticosteroids offers any advantage over topical corticosteroids alone, and they are not recommended in noninfected eczema.6,23 36 z Prescriber January 2016 prescriber.co.uk Eczema 8. Pei AY, et al. The effectiveness of wet wrap dressings using 0.1% mometasone furoate and 0.005% fluticasone proprionate ointments in the treatment of moderate to severe atopic dermatitis in children. Pediatr Dermatol 2001;18(4):343–8. 9. Hindley D, et al. A randomised study of “wet wraps” versus conventional treatment for atopic eczema. Arch Dis Child 2006;91(2):164–8. 10. Beattie PE, Lewis-Jones MS. A pilot study on the use of wet wraps in infants with moderate atopic eczema. Clin Exp Dermatol 2004;29(4):348–53. 11. Svensson A, et al. A systematic review of tacrolimus ointment compared with corticosteroids in the treatment of atopic dermatitis. Curr Med Res Opin 2011;27(7):1395–406. 12. Cury Martins J, et al. Topical tacrolimus for atopic dermatitis. Cochrane Database Syst Rev 2015;7:CD009864. 13. NICE. Atopic eczema in children: management of atopic eczema in children from birth up to age of 12 years. CG57. December 2007. https://www.nice.org.uk/guidance/CG57 14. Harper J, et al. Textbook of Pediatric Dermatology. 3rd edn. Oxford: Blackwell Publishing, 2012. 15. Bath-Hextall F, et al. Dietary exclusions for established atopic eczema. Cochrane Database Syst Rev 2008;1:CD005203. 16. Nankervis H, et al. House dust mite reduction and avoidance measures for treat- ing eczema. Cochrane Database Syst Rev 2015;1:CD008426. 17. Melin L, et al. Behavioural treatment of scratching in patients with atopic dermatitis. Br J Dermatol 1986;115(4):467–74. 18. Noren P, Melin L. The effect of combined topical steroids and habit-reversal treatment in patients with atopic dermatitis. Br J Dermatol 1989;121(3):359–66. 19. Sokel B, et al. The development of a hypnotherapy service for children. Child Care Health Dev 1990;16(4):227–33. 20. Schmitt J, et al. Prednisolone vs. ciclosporin for severe adult eczema. An investigator-initiated double-blind placebo-controlled multicentre trial. Br J Dermatol 2010;162(3):661–8. 21. Salo OP, et al. Efficacy and tolerability of erythromycin acistrate and erythromycin stearate in acute skin infections of patients with atopic eczema. J Antimicrob Chemother 1988;21(Suppl. D):101–6. 22. Ewing CI, et al. Flucloxacillin in the treatment of atopic dermatitis. Br J Dermatol 1998;138(6):1022–9. 23. Birnie AJ, et al. Interventions to reduce Staphylococcus aureus in the management of atopic eczema. Cochrane Database Syst Rev 2008;3:CD003871. 24. Vlachou C, et al. Bleach baths using Milton Sterilising Fluid for recurrent infected atopic dermatitis. Am J Acad Dermatol 2010; 63(Suppl. 1):126. l PRESCRIBING IN CHILDREN n Further reading NICE. Eczema - atopic. Clinical Knowledge Summaries. July 2015. http://cks.nice.org. uk/eczema-atopic University of Nottingham. The Global Resource for Eczema Trials. December 2014. http:// www.greatdatabase.org.uk/GD4/Home/ Index.php University of Nottingham Centre of EvidenceBased Dermatology. Maps of systematic reviews on atopic eczema. May 2014. http://www.nottingham.ac.uk/research/ groups/cebd/documents/methodologicalresources/maponaewebsite.pdf Declaration of interests None to declare. Dr Phillips is a clinical fellow in paediatric dermatology at Nottingham University Hospital/Nottingham Children’s Hospital, Dr Ravenscroft is a consultant dermatologist at Nottingham University Hospital/Nottingham Children’s Hospital and Professor Williams is professor of dermato-epidemiology and co-director of the Centre of EvidenceBased Dermatology, Nottingham University Hospitals NHS Trust Visit Prescriber online at Prescriber.co.uk The Prescriber website provides an easy-to-use search function and visitors have free access to all articles published since 2006. In addition there are up-to-date news items, CPD, blogs, Ask Prescriber and diary dates. Visit us at Prescriber.co.uk www.prescriber.co.uk prescriber.co.uk Prescriber January 2016 z 37