Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
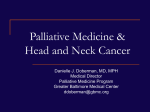
Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives • • • • Identify which patients to refer to hospice Review symptom management Think about rationalising medications Be aware of services which the hospice could provide Questions to consider • What are the barriers to providing good end of life care for patients with heart failure? • What works well? • What is more challenging? • Are there specific patient examples that you can share? Some heart failure statistics • • • • • • 500,000 people in UK 76y - average age at diagnosis 30-40% die within 1 year Costs NHS £378.6 million/year 2% of all NHS inpatient bed days 5% of all emergency admissions • Cardiovascular disease statistics 2014 BHF More statistics • Prevalence of heart failure rising – Ageing population – Improved survival with IHD – Improved heart failure treatment • 6 month mortality rate falling: – 26% 1995 to 14% 2005 • Hospital admissions predicted to rise by 50% over next 25 years NYHA classification Morbidity • Significant symptom burden • Patients have poor understanding of illness progression • Less likely to plan for death & dying – 83-95% die in acute or elderly care hospital bed – 1% die in hospice When to refer to hospice The typical disease trajectories identified in patients with different diseases. Integrated palliative/cardiology services • Which deterioration is the terminal one? • Change of emphasis from active to palliative management difficult • Indicators of poor prognosis provide a trigger for conversations about future plans • “what would you want to do if things get worse” • Heart failure MDT Indicators of Poor Prognosis • • • • • • Previous admissions with worsening heart failure No identifiable reversible precipitant Receiving optimum tolerated conventional drugs Worsening renal function and low sodium Failure to respond within 2-3 days to appropriate change in diuretic or vasodilator drugs Sustained hypotension Up to 50% patients with heart failure die suddenly Specific clinical indicators for heart failure: ― CHF NYHA Stage 3 or 4 ― Patient thought to be in last year of life ― Repeated hospital admissions with heart failure symptoms ― Physical or psychological symptoms despite optimal tolerated therapy Roles of specialist palliative care Symptoms Anderson et al (2001) Pall Med 15(4): 279-86 SOB • • • • • • • Non-pharmacological Relaxation/distraction Breathing retraining Lifestyle changes Hand-held fan Complementary tx Exercise group • • • • Drugs Oramorph 2.5mg 4hrly Lorazepam 0.5mg prn GTN spray Fatigue • Exclude reversible causes – Hb, TFTs, U&E, calcium, magnesium • Review medication – Beta blockers, ACE • • • • Screen for anxiety/depression Pace activity Graded exercise Dietary advice Polypharmacy • Chronic use of >4 medications – 36% patients over 75 take >4 drugs – 50% drugs are not taken as prescribed • Drug interactions • Adverse reactions • Pill burden ADRs Rationalising medications • Which medications are providing immediate symptom benefit? • Which medications might produce rebound symptoms/rapid deterioration if stopped? Consider 1st Consider 2nd Consider 3rd Discontinue drugs with only long term benefit (mortality) Weigh up advantages/disadvantages of continuing drugs with medium term benefit (morbidity/mortality) Continue drugs for short term benefit (morbidity) Statins Digoxin (in sinus rhythm) ACE/ARB Beta blocker Spironolactone Loop & thiazide diuretics Digoxin/beta-blockers (in AF) Anti anginals Drugs for co-morbidities Hypoglycaemics Antihypertensives Thyroxine Warfarin Subcutaneous furosemide • Patient selection • Advanced CHF • Wish to avoid hospital • Need parenteral diuretics • • • • Indications Symptom management End of life Unresponsive to high dose oral diuretics • PPC home/hospice • Poor venous access Paracentesis • Patients with right heart failure – Ascites persists despite aggressive diuretic tx – Symptomatic • 4-6 litre slow paracentesis • Over few days Input from palliative care • • • • • • Hospital Hospice day service Hospice in the home Hospice inpatient unit Counselling Carer support