Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
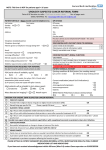
GP REFERRAL PROFORMA FOR SUSPECTED CANCER UROLOGICAL CANCER PLEASE USE 2WW SERVICE ON CHOOSE AND BOOK OR FAX TO 01823 343 417 (MPH) OR 01935 384 640 (YDH) This form should only be used for patients who meet the NICE referral criteria for suspected cancer (2005). All other referring symptoms (e.g. family history for surveillance) should be referred non-urgently by Choose and Book or letter. Do not use this form for non-suspected cancer referrals Decision to refer date (to be completed by GP): Referral received date (to be completed by hospital): Has the patient been informed that they are being referred for suspected cancer? Yes Has the patient been given the 2WW referral patient information leaflet? Yes Please inform the patient that they will be offered an appointment / test within 14 days of receipt of referral Dates patient is unavailable in next 14 days: Patient Details: Surname: Forename: Address: NHS No: Hosp No: No No Referring GP Details: Name: Practice: Post Code: Telephone No: Fax No: E-mail Address: DOB: Daytime Tel No: Mobile Tel No: Please indicate all referring criteria appropriate to your patient from the list below: PROSTATE: BLADDER AND RENAL: Hard, irregular prostate typical of a prostate carcinoma Any age with painless visible (macroscopic) haematuria High PSA (> 20ng/ml) in men with clinically malignant prostate/and/or bone pain 40 years and older with recurrent or persistent urinary tract infection associated with haematuria Elevated age specific PSA in men with 10 year life expectancy 40 years and older with unexplained invisible (microscopic) haematuria on 2 of 3 diptests Please specify PSA result: Abdominal mass identified clinically or on imaging thought to arise from urinary tract Date taken: ___/____/_____ Age specific PSA ranges: 40-49 years 0 – 2.5 ng/ml 50-59 years 0 – 3.5 ng/ml 60-69 years 0 – 4.5 ng/ml 70-79 years 0 – 6.5 ng/ml TESTICULAR: Swelling or mass in body of the testis NB: local agreed PSA levels and men over 80 should only be referred for high PSA levels if likely to need palliative treatment PENIS: Any suspected penile cancer WHO Performance Status: 0 1 2 3 4 (circle) (0: fully active; 1: able to carry out light work; 2: capable of self care, up and about more than 50% of waking hours; 3: only limited self care, confined to bed or chair; 4: completely disabled, no self care ability) Please attach* additional clinical details to include: significant medical history co-morbidities current medication, clearly indicating if the patient is receiving any anti coagulation therapy. recent blood results any other relevant information * Please note that referrals received without adequate supporting clinical information and relevant blood results cannot be processed and will be returned to the referrer as incomplete 1 Final Urological Suspected Cancer Combined CAB Proforma March 2013