Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
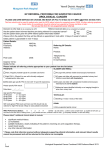
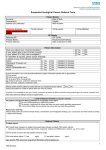
NOTE: This form is NOT for patients aged < 16 years UROLOGY SUSPECTED CANCER REFERRAL FORM Date of GP decision to refer: Click here to enter a date. No. of pages sent: EMAIL REFERRAL TO: [email protected] PATIENT DETAILS – Must provide current telephone no. GP DETAILS Address: TEL: FAX: Practice email: Practice’s direct access telephone/GP mobile – for use by Consultant only: Last name: Gender: M ☐ F ☐ NHS No: First name: DOB: Telephone (mobile/daytime): Telephone (evening): Patient agrees to telephone message being left? Email: Interpreter required? Y ☐ Learning difficulties? Y ☐ GP name: Practice Code: Address: DISCUSSIONS WITH PATIENT PRIOR TO REFERRAL Y☐N☐ Language/Hearing: Cancer needs to be excluded Patient given referral information leaflet Date(s) unavailable next 14 days: ☐ ☐ CONFIRM PATIENT’S RENAL FUNCTION: Mental capacity assessment required? Y ☐ CREATININE _______ Known safeguarding concerns? Y ☐ OTHERWISE IT IS NOT POSSIBLE FOR US TO ORDER CT SCANS WITH CONTRAST AS PART OF A ONE STOP SERVICE. IF NO CREATININE SEND BLOOD SAMPLE FOR U&E. Mobility requirements (unable climb on/off bed)? Y☐ INVESTIGATIONS REQUIRED FOR REFERRAL Microscopic haematuria: 2 of 3 urine dip or >12RBC on microscopy PATIENT MEDICAL HISTORY Existing conditions & Risk factors (inc smoking status): You don’t need to wait for results of tests to refer. PSA (serial values if available, ng/ml) 1. Date: / /20 2. Date: _ / /20 Repeat PSA after 4 weeks, (inc where PSA <15 and rectal examination yields normal results) If UTI present, treat and repeat PSA after 6 weeks. Most patients will go straight to test, please report: ☐ Creatinine ☐ eGFR ☐ WBC ☐ Hb Mass detected on imaging? Y ☐ N ☐ Attach report ☐ current smoker ☐ referred to stop-smoking service Current medication (attach list & indications): Allergies Anticoagulants/Antiplatelets Immunosuppressants Diabetic WHO Patient Performance status (see key below) ☐0 ☐1 ☐2 CRITERIA FOR URGENT 2WW SUSPECTED CANCER REFERRAL ☐ PROSTATE CANCER ☐ Prostate feels malignant (hard, irregular) on digital rectal examination (DRE) Please, specify PSA level _______ ng/ml ☐ Raised/rising age specific PSA ☐ BLADDER / RENAL CANCER ☐ Age >45 yrs with unexplained visible haematuria without UTI ☐ Age >45 yrs with visible haematuria that persists or recurs after successful treatment of UTI ☐ NB: ☐ ☐ ☐ ☐ ☐ ☐ ☐ Y☐ Y☐ Y☐ Y☐ ☐3 ☐4 OR OR OR Age >60 yrs with unexplained non-visible haematuria and either dysuria or a raised white cell count on blood test – please specify level Consider non-urgent referral in patients aged ≥60 yrs with unexplained recurrent or persistent urinary tract infection. TESTICULAR CANCER Non-painful enlargement or change in shape or texture of the testis OR Abnormal ultrasound scan, please send report with this referral PENILE CANCER Penile mass or ulcerated lesion, where a sexually transmitted infection has been excluded as a cause OR A persistent penile lesion after treatment for a sexually transmitted infection has been completed OR Unexplained or persistent symptoms affecting the foreskin or glans PLEASE ATTACH A PATIENT SUMMARY INCLUDING REFERRAL LETTER, INVESTIGATION RESULTS, PMH, CURRENT MEDICATIONS LIST AND INDICATIONS If you have not received acknowledgement within 48 hours (Mon-Fri) contact 2ww supervisor on 01438 285206 If your patient does not meet NICE suspected cancer referral criteria, but you feel they warrant further investigation, please disclose full details in your referral letter. ADDITIONAL INFORMATION WHO PATIENT PERFORMANCE STATUS KEY 0 1 2 3 4 Fully active, able to carry on all pre-disease performance without restriction Restricted in physically strenuous activity but ambulatory and able to carry out light/sedentary work, e.g. house or office work. Ambulatory and capable of self-care, but unable to carry out work activities. Up and active > 50% of waking hours. Capable of only limited self-care. Confined to bed or chair >50% of waking hours. Completely disabled. Cannot carry out any self-care. Totally confined to bed or chair. FOR HOSPITAL USE ONLY Date referral received: _ _ /_ _ /_ _ _ _ 1st appointment date offered: _ _ /_ _ /_ _ _ _ 2nd appointment date offered: _ _ /_ _ /_ _ _ _ If 1st appointment date not accepted, give reason/s: