Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
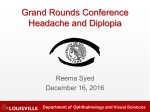
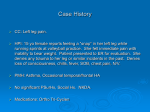
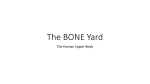
Case Report iMedPub Journals http://journals.imedpub.com Health Science Journal ISSN 1791-809X Care of a Patient with Fibrous Dysplasia of the Clavicle and Ribs: Case Report Abstract Introduction: Fibrous dysplasia of the ribs and clavicle is a polyostotic form of skeletal system disease. The most commonly reported symptom is pain. Surgical treatment, which is the primary therapeutic approach, may contribute to the emergence of complications in surgical site that are difficult to treat. The aim of the study was to analyze interdisciplinary care of a patient chronically treated for fibrous dysplasia of the clavicle and ribs. Methods: The interview, observation, and analysis of medical records method was used in the study. The case describes a 51-year-old man with a diagnosis of fibrous dysplasia of the clavicle and ribs, hospitalized in the Department of Thoracic Surgery of Medical University of Gdansk (MUG) in the years 1995-2013. 2015 Vol. 10 No. 1:12 Agnieszka Kruk1, Janina Książek1, Wojciech Żurek2, Sylwia Terech1, Piotr Jarzynkowski1 and Renata Piotrkowska1 1 Department of Surgical Nursing, Medical University of Gdansk, Poland 2 Faculty and Clinic of Chest Surgery, Medical University of Gdansk, PolandIran Correspondence: Janina Książek Results: Progressive disease process caused a lot of health problems in the patient and deterioration in the quality of life in every aspects of his life . Conclusions and relevance for clinical practice: Care and treatment in hospital and at home are focused on the pain and chronic wound healing process, which require the involvement of the entire interdisciplinary team. Zakład Pielęgniarstwa Chirurgicznego, Katedra Pielęgniarstwa GUMed, Dębinki 7, 15, Poland. Keywords: Fibrous dysplasia of bone; Smoking; Interdisciplinary care; Chronic wound healing; Education Tel: +48 58 3491247 Received: November 30, 2015; Accepted: December 12, 2015; Published: December 30, 2015 Introduction Fibrous dysplasia - FD (lat. dysplasia fibrosa – DF) is a rare chronic bone disease, characterized by the presence of one or more areas where healthy bone is replaced by fibrous tissue [1]. The cause of this disease is not fully understood. It is currently considered that the reason for its development is a mutation in the GNAS1 gene, which leads to the production of abnormal G protein responsible for the regulation of bone synthesis. This promotes the development of metabolic bone disorders. Normal trabecular bone structure is rebuilt in fibrous tissue, in which, as the disease progresses, metaplastic bone structure occurs. This can cause impaired growth, brittleness, and deformation of bones affected by disease process. The effects of mutation apply also to endocrine balance and disrupt the body pigmentation [2]. The clinical picture of a generalized form of FD (lat. osteitis fibrosa generalisata) was first described in 1981 by Recklinghausen. It was only in 1938 when Lichtenstein distinguished fibrous dysplasia of bone as a separate disease entity (lat. dysplasia fibrosa ossium) [1,2]. The incidence of the disease is not precisely known. © Copyright iMedPub | This article is available in: www.hsj.gr/archive [email protected] Citation: Kruk A, Książek J, Żurek W, et al., Care of a Patient with Fibrous Dysplasia of the Clavicle and Ribs: Case Report. Health Sci J. 2015, 10:1. Epidemiological data say that it constitutes 2.5% of tumor-like changes and about 7% of benign tumors [3,4]. The World Health Organization defines three forms of the disease: 1) monostotic, which accounts for about 70% of all cases and affects one bone; 2) polyostotic, when the changes are observed in many bones; and 3) the form in which the disease involves craniofacial bones only. McCune-Albright syndrome is a polyostotic form where, in addition to multifocal changes, disorders of the endocrine glands occur (precocious puberty, hyperthyroidism, hyperpituitarism, hyperadrenocorticism, overactive adrenal medulla) and the presence of café au lait spots on the skin, scoliosis [1,4]. The image of the disease may be preceded by the appearance of disease symptoms, such as pain, deformations, and bone fractures. However, the diagnosis is based on the result of histopathological and imaging tests. An additional diagnostic procedure is the determination of the alkaline phosphatase level in serum. The treatment of choise is surgery if possible, which reduces pain and improves mobility, and a secondary healing of fractures [5]. The surgery involves the removal of pathological focus with a 1 ARCHIVOS DE MEDICINA Health Science Journal ISSN 1698-9465 1791-809X 2015 Vol. 10 No. 1:12 margin of healthy bone and subsequent tissue transplantation. In some cases a stabilizing action is required with the use of metal implants and bone cement. Conservative treatment consists of regularly taking bisphosphonates, which influence bone remodeling, reduce pain, and slow the pathogenic processes. Availability of bisphosphonates in Poland is limited because they have not been registered for the treatment of FD [6,7]. plexus at the left side was performed. The image clearly showed compression of the upper lobe of the left lung by pathological tissue with low signal at time T1 and T2 dependent. Probably the changes corresponded to the postoperative scar and partly to the main process - FD. Nerve trunks with blurred outlines were seen, probably in the course of accompanying fibrosis due to compressive and postoperative changes. What does this Paper contribute to the wider global clinical community? In 1999, on the basis of radiological documentation from the years 1994 to 1999, an opinion was given, based on which the constant progression of lesions of the dysplasia fibrosa ossium type was stated. The nature of progression was uneven, i.e. on the right side it is clearly slower than on the left side, where currently the morphological status of the bone corresponds almost exactly to the degree of severity of the changes just before surgery. The described case shows the need for the introduction of consultation meetings involving specialist doctors, psychologists, and health workers into clinical practice in the care of FD patients. Methods The interview, observation, analysis of medical records, and case study method was used in the study. The place of research is the Department of Thoracic Surgery, University Clinical Center, Medical University of Gdansk. The case describes a 51-year-old man diagnosed with fibrous dysplasia of the clavicle and ribs, hospitalized in the years 1995-2013. The report is additionally supplemented with figures of the wound healing process in years 2012-2014. The aim of this case report is to analyze interdisciplinary care of a patient chronically treated for fibrous dysplasia of the clavicle and ribs . Case Report A 51-year-old male, heavy smoker (30 pack years, without willingness to quit the habit) was treated for bone fibrous dysplasia since 1994. The first symptoms appeared at the age of 30. The patient came to the physician because of severe pain in the chest. In 1995, based on computed tomography scan (CT) of the chest, features of thickening of the proximal parts of clavicles and ribs I and II on the left side in the parasternal part with characteristics of fibrous-like intraosseous hypertrophy and sclerosis. In addition to intraosseous changes, thickening of the adjacent soft tissues was observed. In the CT image bone remodeling characteristic for fibrous dysplasia of the clavicle and ribs was observed. Initially, the patient was qualified for the partial resection of the left clavicle. After three months thoracotomy was done with resection of parasternal fragments of the second and the third rib on the left. On the anatomopathological examination, the image of FD was confirmed. Results of laboratory tests showed normal serum levels of inorganic phosphorus, total calcium, and alkaline phosphatase. In 1996 the case was consulted by representatives of the Polish Osteoporosis Foundation (Polska Fundacja Osteoporozy, PFO). The PFO advised that due to the lack of established methods for the treatment of FD, pharmacological treatment is recommended. It was stated that the use of calcitonin, a known stimulant of somatostatin should have a positive effect on bone morphological image. According to the recommendations, treatment with Miacalcic Nasal Spray, a 100 I.U. in a scheme of two times a day for a month, then a month break, was used for the next three years. Despite therapy, the man continued to suffer pain. In 1998, an Magnetic Resonance Imaging (MRI) of the brachial 2 In 2001, the patient was again qualified for surgery, in this time for partial resection of the left clavicle. In anatomopathological examination of surgical specimen irregular trabeculae of bone and intertrabecular spaces filled with the connective tissue in larger spaces in the purulent inflammation of the clavicle fragment were seen. There were no characteristics of fibrous dysplasia of bone. In 2004, resection of a fragment of the sternum, part of clavicle, and first and second rib on the left was performed, and subsequently the patient was qualified for chest radiation in a single fraction 6Gy. Following treatment the patient was discharged home. In 2006, the patient came to the Department of Thoracic Surgery because of severe pain. It was caused by compression of the hypertrophic clavicle and first rib on the brachial plexus on the right side. During qualification for the surgery, the patient was found to be a carrier of hepatitis C. Right clavicle resection and partial resection of the first rib were done. The postoperative course was uneventful. The patient was discharged home with Figure 1 3D CT reconstruction of bony elements of the chest after resection of upper ribs and upper part of the sternum. Source: Own material provided by the patient. This article is available in: www.hsj.gr/archive ARCHIVOS DE MEDICINA Health Science Journal ISSN 1698-9465 1791-809X instructions for urgent control in the Pain Clinic to reduce the doses of opioid drugs. The macroscopic test result confirmed the clinical diagnosis corresponding to FD. On the CT image from 2007, bone distension and deformation was visible; discreetly uneven internal profile of the cortex with small foci of sclerosis (Figure 1). Because of the persistent chest pain and visible changes in the radiographic image in 2008, surgical treatment was continued. The sternum and a fragment of the chest wall were resected with mesh implantation. Resection of the second and third rib on the right side was performed. A year later, the patient came to the hospital because of purulent fistula in the postoperative wound. Plastic surgery of the chest wall was performed and antibiotic therapy included. The patient was discharged on the seventh postoperative day. In 2009, the patient was hospitalized again for recurrent skin-mediastinal fistula. The fistula was excised with skin-muscle flap plastic reconstruction was performed. In 2010, the patient was hospitalized twice because of chronic suppuration of the wound. Revision of the wound was performed. The skinmuscle fistula was excised with wound left for granulation In 2011 an improvement in the wound healing process was achieved, and the decision to close it was made. In the further postoperative course the patient developed symptoms of inflammation again, the wound was opened, and treatment with the use of dressings was continued. The bacteriological test confirmed methicillinresistant Staphylococcus aureus (MRSA) wound infection. During hospitalization the patient was treated with the vacuum dressing.. After achieving local improvement and after consulting the plastic surgeon the patient was qualified for surgery. The granulating chest wound was covered with a skin autograft from the left thigh. In the following postoperative days the wound was without signs of inflammation. The patient was discharged home. In 2012, outpatient therapy was needed because of wound suppuration (Figure 2). In September 2013, the patient came to Figure 2 Picture of the chest wound around the upper part of the sternum, November 2012. Prolongated healing of the wound after full thicknes skin transplantation with areas of granulation. Prolongated healing due to local infection with discharge and scabbing. Source: own material. © Under License of Creative Commons Attribution 3.0 License 2015 Vol. 10 No. 1:12 the hospital with purulent fistula at the upper part of the sternum, for further treatment. Revision of the wound in the upper part of the sternum was performed under general anesthesia. In that time patient reported progressive weakness with body weight loss of approximately 10% of his total body weight. Now he is a lonely person, living from social welfare benefits. He is under the care of a pain clinic, and he is addicted to narcotic drugs for pain. He currently takes medication in doses: Morphine 40 mg (s.c.) 4 x daily; MST 200 Continus 200 mg/ BD Sevredol 20 mg/tablet 4 x daily; and Ketoprofene 50 mg/tablet 4 x daily. Additionally, Diazepam 5 mg/tablet 2-3 times a day, and due to difficulty in falling asleep Lorazepam 2.5 mg/tablet once a day were included. He requires the assistance of another person in the field of wound care (Figures 3 and 4) and remains under the ambulatory care of a surgeon and a health worker. Table 1 shows the course of the therapy and nursing care over the years 1995 to 2013. Discussion Surgical treatment of FD is a complex process with uncertain results and often requires repeated operations. At a time when significant attention is devoted worldwide to stem cells as a potential tool for curing incurable diseases, fibrous dysplasia of bone (FD) provides a paradigm for stem cell diseases. Recognizing FD as a stem cell disease gives way to generate appropriate models of the disease, which will continue to provide further insight into its natural history and pathogenesis. It is believed that skeletal stem cells may be a tool for innovative treatments. These can be conceived as directed to alter the in vivo behavior of mutated stem cells, to replace mutated cells through local transplantation, or to correct the genetic defect in the stem cells themselves. In vitro and in vivo models are currently being generated and results are being expected [2]. Several years of experience with treatment and nursing care of patients with fibrous dysplasia of the clavicle and ribs have revealed how serious and complex problem is for the interdisciplinary team in the care of chronically treated patients. Long-term surgical treatment of patients causes frequent changes of the environment and can be a source of emotional tension, leading even to social isolation. Pain is one of the most frequent symptoms of fibrous dysplasia (FD). The severity of pain in patients with FD is highly variable, and it is more common in adults than in children. It has been observed in 81% of adults and 49% of children [8,9,10]. Analysis of the course of treatment shows that bone pain was the most frequently reported symptom (Table 1). Basic analgesics have insufficient effect, and such a situation leads doctors to refer patients to specialist outpatient treatment of chronic pain. In the case described, the patient has taken opioids for several years, and their doses had to be modified during therapy due to the increasing tolerance. In the group of patients treated chronically with opioids, cases of addiction are reported sporadically, and studies have shown the existence of genetic predisposition to addiction, either to drugs or other psychoactive substances [11,12]. Treatment of chronic wound is a difficult and long-term process that requires close cooperation between specialists. In this case, there were a chest surgeon, primary care physician, nurses 3 ARCHIVOS DE MEDICINA Health Science Journal ISSN 1698-9465 1791-809X 2015 Vol. 10 No. 1:12 control of a primary care physician and health visitor. The analysis of this case revealed deterioration in wound healing during this period of treatment (Figures 3 and 4). Outpatient care is primarily focused on continuing education in the field of wound care and health behaviors. The patient refuses to quit smoking despite the fact that he has been a smoker for 30 years. Any attempts of anti-smoking education during hospitalization did not bring the expected result. The patient was informed about the negative effects of smoking on wound healing [13]. In the last years of hospitalization increased somatic symptoms and impaired functioning in many spheres of life were observed in this patient. They can cause deterioration of quality of his life. Studies previously published by Kelly, concerning the quality of life in adults and children with FD, showed worse physical functioning than in the control group [14]. Conclusions Figure 3 Picture of the chest wound around the upper part of the sternum, June 2013. Healing of the wound after full thicknes skin transplantation with still visible areas of granulation without epithelisation (oozing granulation). Light pink colour cicatrix in the process of remodelling with more smooth surface. Source: own material. 1. Education in wound care and overcoming pain in the home environment requires constant support of physicians and nurses and special attention paid to the patient's psychosocial requirements. 2. Chronic smoking indicates a need to focusing on the problem of health behaviors and their impact on wound healing, and consideration of professional anti-smoking therapy for the patient. 3. Long-term results of surgical treatment of multifocal form of FD are uncertain and the treatment is long lasting. The chronicity of the treatment significantly affects the psyche of the patient and requires psychological support. 4. Steam cell therapy is possible promising approach as a new FD therapy directed to alter the in vivo behavior of mutated stem cells – in vitro and in vivo models are currently being generated and final results are expected. 5. Treatment of FD patients should be carefully planned by multidisciplinary consultation meetings with the participation of physicians, psychologists, and health worker. Relevance for Clinical Practice Figure 4 Picture of the chest wound around the upper part of the sternum, January 2014. The scar in majority is remodelled with light, smooth surface. There is overgrown granulation on the right side of the scar. Source: own material. working in the surgical department, and a health visitor who takes care of patients in their home. Nurses and physicians must continuously update their knowledge in the field of new wound treatment regimens to ensure the effective treatment for the patient in accordance with the current treatment algorithm. A vacuum-based method of wound healing was applied during the patient's stay in hospital, which resulted in the desired therapeutic effect. The patient was discharged home with instructions to continue the treatment of wounds under the 4 The aim of the study is to draw attention to fibrous dysplasia of the clavicle and ribs, uncommon in clinical practice. Previously published works that describe the clinical image of the disease often ignore issues related to the functioning of the patient and the influence of the treatment on quality of life. Physical and epidemiological indicators, previously used in the treatment process, became insufficient for evaluation of some diseases, especially chronic ones. The described case shows the need for the introduction of multidisciplinary consultation meetings involving specialist doctors, psychologists, and health workers into clinical practice in the care of FD patients. Conflict of Interest None of the authors declared any conflict of interest. Acknowledgements The language assistance was provided by Proper Medical Writing Sp. z o.o., Warsaw, Poland. This article is available in: www.hsj.gr/archive ARCHIVOS DE MEDICINA Health Science Journal ISSN 1698-9465 1791-809X 2015 Vol. 10 No. 1:12 Table 1. The course of the disease with regard to surgical methods for the treatment and care of selected problems. Years of hospitalization 1994, 1995 UCK 1995 PCT & UCK 2001 PCT & 2002 OSK 2004 PCT Diagnosis and treatment Selected problems of nursing care •The emergence of severe chest pain. •Anxiety caused by the onset of •Outpatient treatment. The X-ray examination of the chest disease symptoms. thickening of the clavicle bones and ribs on the left side was found. •Anxiety caused by •The resection of the fragment of the clavicle on the left side. prolonged diagnostic process. •Resection of parasternal fragments of ribs II-III on the left side. •Knowledge deficit of the surgical •Histopathological examination revealed fibrous dysplasia of clavicle site care. and ribs I, II, and III. •Fear as a result of the diagnosis of FD. •Excision of dysplasia focus in the proximal left clavicle. •Emotional problems as a result of •Partial resection of the right clavicle. marriage breakdwn. •Resection of the fragment of sternum, clavicle, • rib I and II on the left side. •Knowledge deficit due to the •Teletherapy - Cliniac linear accelerator 6 MeV photons on the chest inclusion of a new therapy. 2004 UCK area with the technique of 2 parallel opposed fields of dimensions •The risk of complications after 11x15 cm Dgref. = 6Gy/1FR. teletherapy. •Removal of the right clavicle and partial resection of rib I on the •Chronic pain. right side. 2006 UCK •Possibility of complications •Consultation in chronic pain clinic. Suspected addiction to resulting from smoking habit. analgesics. •The intensification of pain and radiological changes of the chest. •Resection of the clavicle and the fragment of the chest wall with •Anxiety caused by chronic wound 2008 UCK mesh implantation. treatment. •Resection of ribs II and III on the right side. •Disorders in the correct health •Postoperative wound suppuration. 2008 UCK behaviors. •Thoracomioplastic operation. •Anti-smoking education •Treatment for chronic skin/mediastinal fistula. 2009 UCK •Resection of fistula and skin/muscle plastic surgery •Resection of skin/mediastinal fistula 2010 UCK •Wound revision •Plastic surgery and postoperative wound closure. •Knowledge deficit of the care of •In the course of postoperative care the wound was opened and surgical site. 2011 UCK treatment was continued with the use of the vacuum based •Discomfort due to chronic dressings method. infection of the wound. •Fear as a result of the diagnosis of FD. 2012 •Outpatient treatment •The progressive body weight loss. •Difficult financial situation. 2013 Specialist Hospital •Surgery of suppurative fistula at the upper part of the sternum. •Loneliness. in Prabuty •Resection of the mesh and the chest wall. •Anxiety caused by chronic wound treatment. Source: author’s own analysis. Description: 1. UCK: University Clinical Centre in Gdansk, 2. PCT: Pomeranian Centre of Traumatology in Gdansk. (Copernicus), 3. OSK: District Railway Hospital in Gdansk. © Under License of Creative Commons Attribution 3.0 License 5 ARCHIVOS DE MEDICINA Health Science Journal ISSN 1698-9465 1791-809X References 1 Dixon JL, Smythe WR, Rascoe PA, Reznik SI (2013) Surgical resection of giant fibrous dysplasia for near respiratory collapse. Ann Thorac Surg 95: 135-137. 2 Riminucci M, Saggio I, Robey PG, Bianco P (2006) Fibrous dysplasia as a stem cell disease. J Bone Miner Res 21: 125-131. 3 Mohan H, Mittal P, Mundi I, Kumar S (2011) Fibrous dysplasia of bone: A clinicopathologic review. Pathol Lab Med Int 3: 31-42. 4 Bhadada S, Bhansali A, Das S, Singh R, Sen R, et al (2011) Fibrous dysplasia & McCune-Albright syndrome: An experience from a tertiary care centre in north India. Indian J Med Res 133: 504-509. 5 Ozkaya S, Findik S, Demir H, Yuksel C, Atici AG (2009) Polyostotic fibrous dysplasia of the ribs: An unusual cause of chest pain and dyspnea. Int Med Case Rep J 2: 23-25. 2015 Vol. 10 No. 1:12 8 Weerasuriya T, Nashi S, Morgan A, Ebizie A (2012) A dilemma of fibrous dysplasia versus chronic osteomyelitis of the clavicle. BMJ Case Rep 2012. 9 Chapurlat RD, Gensburger D, Jimenez-Andrade JM, Ghilardi JR, Kelly M, et al. (2012) Pathophysiology and medical treatment of pain in fibrous dysplasia of bone. Orphanet J Rare Dis 7 Suppl 1: S3. 10 Kelly MH, Brillante B, Collins MT (2008) Pain in fibrous dysplasia of bone: age-related changes and the anatomical distribution of skeletal lesions. Osteoporos Int 19: 57-63. 11 Jimenez-Andrade JM, Mantyh WG, Bloom AP, Freeman KT, Ghilardi JR, et al. (2012) The effect of aging on the density of the sensory nerve fiber innervation of bone and acute skeletal pain. Neurobiol Aging. 33: 921-932. 12 Clark JD (2002) Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage 23: 131-137. 6 DiCaprio MR, Enneking WF (2005) Fibrous dysplasia. Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am 87: 1848-1864. 13 Sorensen L (2012) Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: A systematic review and meta-analysis. Arch Surg 147: 373-383. 7 Stanton RP, Ippolito E, Springfield D, Lindaman L, Wientroub S, et al. (2012) The surgical management of fibrous dysplasia of bone. Orphanet J Rare Dis 7 Suppl 1: S1. 14 Kelly MH, Brillante B, Kushner H, Robey GP, Collins MT (2005) Physical function is impaired but quality of life preserved in patients with fibrous dysplasia of bone. Bone 37: 388-394. 6 This article is available in: www.hsj.gr/archive