Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
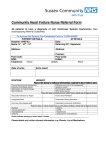
Pulse Wave Analysis of the Aortic Pressure Waveform in Severe Left Ventricular Systolic Dysfunction Scott J. Denardo, MD; Ramavathi Nandyala, MD; Gregory L. Freeman, MD; Gary L. Pierce, PhD; Wilmer W. Nichols, PhD Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 Background—The effect of moderate left ventricular systolic dysfunction (LVSD) on ventricular/vascular coupling and the aortic pressure waveform (AoPW) has been well described, but the effect of severe LVSD has not. Methods and Results—We used noninvasive, high-fidelity tonometry of the radial artery and a mathematical transfer function to generate the AoPW in 25 treated patients with LVSD (mean LV ejection fraction, 24⫾8.8%; range, 11% to 40%; 21 patients ⬍30%). Pulse wave analysis of the AoPW was used to characterize ventricular/vascular coupling and compared with pulse wave analysis performed in 25 normal subjects matched for age, gender, height, body mass index, and heart rate. Measurements obtained using pulse wave analysis in LVSD patients indicated features of poor LV stroke performance and also reduced indices of arterial stiffness: increased travel time of the pressure wave (147⫾10 ms versus 132⫾21 ms; P⬍0.001); decreased systolic duration of reflected wave (134⫾24 ms versus 167⫾26 ms; P⬍0.001); ejection duration (277⫾22 ms versus 299⫾25 ms; P⬍0.008); percent systolic duration (32⫾5.3% versus 35⫾4.0%; P⬍0.02); aortic systolic pressure (100⫾16 mm Hg versus 121⫾16 mm Hg; P⬍0.001); unaugmented pressure (24⫾6.3 mm Hg versus 32⫾6.4 mm Hg; P⬍0.001); augmented pressure (4.8⫾3.1 mm Hg versus 9.6⫾4.5 mm Hg; P⬍0.001); pulse pressure (28⫾7.4 mm Hg versus 42⫾9.5 mm Hg; P⬍0.001); augmentation index (12⫾6.6% versus 23⫾7.6%; P⬍0.006); wasted LV effort (5.3⫾2.8⫻102 dyne sec/cm2 versus 17⫾10⫻102 dyne sec/cm2; P⬍0.001); systolic pressure time index (17⫾4.1⫻102 mm Hg-sec/min versus 23⫾4.2⫻102 mm Hg sec/min; P⬍0.001); and pressure systolic area (383⫾121 mm Hg sec/min versus 666⫾150 mm Hg sec/min; P⬍0.001). Conclusions—Severe LVSD causes measurable changes in the AoPW. Standardization of AoPW findings in LVSD patients may allow for the clinical use of radial artery pulse wave analysis to noninvasively determine the severity of dysfunction and aid in logical therapy. (Circ Heart Fail. 2010;3:149-156.) Key Words: aortic pressure waveform 䡲 left ventricular dysfunction 䡲 hemodynamics 䡲 ventricular/vascular coupling T he measured central aortic pressure waveform (AoPW) is the summation of a forward-traveling (incident) wave generated by left ventricular (LV) ejection and a backwardtraveling wave caused by reflection of the forward wave from sites of change in impedance within the peripheral arterial system.1–3 Both the forward and reflected pressure waves are related to LV ejection wave amplitude. Additionally, the forward traveling wave is affected by central (elastic) arterial stiffness and peak LV ejection, whereas the reflected wave is affected by the elastic properties of the entire arterial tree, transmission velocity of the forward and reflected waves, and distance to the major reflecting site. The functions of the LV and peripheral arterial system are interactive (ie, ventricular/ vascular coupling) and conditions that directly affect one can cause a responsive change in the other.4 The net effect of this coupling on the morphology of the AoPW can be described by a series of quantifiable characteristics obtained using pulse wave analysis (PWA).5–7 Certain clinical conditions, such as advanced age, obesity, hypertension, diabetes mellitus, coronary artery disease, myocardial infarction, and chronic renal disease unfavorably alter ventricular/vascular coupling, and the associated changes in the AoPW have been described.8 –12 Additionally, this unfavorable alteration of ventricular/vascular coupling is associated with increased arterial stiffness and has been linked directly to the subsequent development of adverse cardiovascular outcomes including chronic heart failure and death. Clinical Perspective on p 156 Central aortic pulse pressure (cPP)—the difference between the central aortic systolic and diastolic blood pressure—is a characteristic of the AoPW that is relatively simple to measure. Recent studies have shown that both invasive13 and noninvasive14,15 measurements of cPP correlate positively and strongly with the subsequent development of cardiovascular disease and adverse outcomes. Conversely, 3 Received March 10, 2009; accepted October 10, 2009. From the University of Florida (S.J.D., W.W.N.) and Department of Veterans Affairs Medical Center (S.J.D.), Gainesville, Fla; University of Texas Health Science Center (R.N., G.L.F.), San Antonio, Tex; and University of Colorado (G.L.P.), Boulder, Colo. Correspondence to Scott J Denardo, MD, Division of Cardiovascular Medicine, University of Florida College of Medicine, 1600 SW Archer Rd, PO Box 100277, Gainesville, FL 32610. E-mail [email protected] © 2010 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org 149 DOI: 10.1161/CIRCHEARTFAILURE.109.862383 150 Circ Heart Fail January 2010 taking cardiovascular drugs at the time of the study. All patients and subjects had data collected in the basal state, in the supine position, and in a quiet, temperature-controlled room after a rest period of at least 10 minutes. Peripheral Cuff Blood Pressure Measurement Brachial systolic and diastolic blood pressures (bSP and bDP, respectively) were measured in the left arm using a validated, automatic, oscillometric BP monitor (Omron R3, Omron Healthcare, Kyoto, Japan), and an appropriately sized cuff. Three measurements were taken at least 2 minutes apart and the latter 2 were averaged and used in data analysis and calibration of the AoPW. The variable bPP was calculated as the difference between bSP and bDP. Pulse Waveform Analysis Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 Figure 1. A synthesized central aortic pressure waveform. The early part of the ascending aortic pressure wave of amplitude (Pi⫺Pd) is generated by LV ejection. The later part of the pressure wave with amplitude (Ps⫺Pi) is generated by the reflected wave arriving during systole and adding to the forward pressure wave. cPP⫽(Pi⫺Pd)⫹(Ps⫺Pi)⫽(Ps⫺Pd) and AIa⫽(Ps⫺Pi)/(Ps⫺Pd). The area under the systolic portion of the reflected wave (dark shaded area) is defined as LV wasted effort (Ew). PSA⫽⌬PSA⫹Ew and is the area enclosed by the systolic pulse pressure wave. SPTI⫽⌬SPTI⫹⌬PSA⫹Ew and is the area under the systolic portion of the pressure wave and DPTI is the area under the diastolic portion of the wave. P1 indicates the first systolic pressure peak (or shoulder); Pi, merging point (inflection point) of the forward and reflected waves; Tr, round-trip travel time of the pressure wave; SDR, systolic duration of reflected wave; ED, ejection duration. previous large clinical studies found an inverse (or negative) relation between peripheral brachial pulse pressure (bPP) and mortality in patients with severe LV systolic dysfunction (LVSD).16 –18 Additionally, the effects of mild to moderate LVSD on arterial stiffness and the AoPW in patients with normal mean arterial pressure have been fairly well described and show an increase in aortic stiffness, pulse wave velocity (PWV), characteristic impedance, and cPP compared with normal subjects.19 –23 However, a quantitative description of the AoPW in patients with severe LVSD beyond cPP has not been fully described. We therefore sought to investigate changes in the AoPW associated with altered ventricular/ vascular coupling in patients with severe LVSD using noninvasive, high-fidelity tonometry of the radial artery and synthesized central aortic PWA. Methods LVSD Patient and Normal Subject Populations This cross sectional study was approved by the University of Florida Institutional Review Board, and all LVSD patients (N⫽25) and normal subjects gave informed written consent. Twenty-three of the LVSD patients had New York Heart Association Class III to IV chronic congestive heart failure symptoms. Additionally, all LVSD patients were in normal sinus rhythm; all had undergone quantitative echocardiography which confirmed LVSD as the cause of heart failure (LV ejection fraction [EF] range, 11% to 40%; 21 patients ⬍30%) and demonstrated no significant valvular abnormality, and all were receiving medical therapy accordingly. Data from these 25 LVSD patients were compared with those from a group of normal subjects (N⫽25) matched for age, gender, height, body mass index, and heart rate. Normal subjects were all asymptomatic, had no history of cardiovascular disease, and had normal clinical examinations and normal ECGs. None of them were current smokers or Assessment of wave reflection characteristics, ejection duration, and area indices were performed using the SphygmoCor system (AtCor Medical, Sydney, Australia). Radial artery pressure waveforms, calibrated using cuff measured brachial systolic and diastolic pressure, were recorded at the left wrist noninvasively, using applanation tonometry that incorporated a high-fidelity micromanometer (Millar Instruments, Houston, Tex). A validated generalized mathematical transfer function was applied to 20 sequential waveforms, which were then ensemble averaged to generate the central AoPW (Figure 1).24 Characteristics of the AoPW were then determined using PWA.5,6,25 Importantly, the time from the beginning upstroke of the synthesized aortic systolic pressure waveform (Pd) to the upstroke of the reflected wave (inflection point, Pi) is the round-trip travel time (Tr) of the pressure wave to and from the major reflecting site in the lower body and is related to arterial stiffness of the entire arterial system.2,4,7 Increased arterial stiffness increases PWV and leads to a more rapid Table 1. Baseline Characteristics of LVSD Patients and Normal Subjects LVSD Patients (N⫽25) Normal Subjects (N⫽25) P Age, y 57⫾11 54⫾11 0.43 Male gender 20 (80) 20 (80) 1.00 173⫾9.5 174⫾7.4 0.62 Characteristic Height, cm Weight, kg 2 85⫾18.6 82⫾16.8 0.58 Body mass index, kg/m 29⫾6.1 27⫾3.9 0.08 Heart rate, bpm 69⫾13 72⫾11 0.51 NYHA CHF class III/IV 23 (92) 0 LVEF, % 24⫾8.8 NA CAD 10 (40) 0 CABG 9 (36) 0 17 (68) 0 ACE-I 15 (60) 0 ARB 3 (12) 0 -blocker 6 (24) 0 ␣-blocker 13 (52) 0 Diuretic 18 (72) 0 ALD-blocker 9 (36) 0 Digoxin 6 (24) 0 Risk Conditions ICD Medication, % Data are presented as mean⫾SD or n (%). NYHA indicates New York Heart Association; NA, not available; CAD, coronary artery disease; CABG, coronary artery bypass grafting; ICD, intracardiac defibrillator; ACE-I, angiotensin converting enzyme inhibitor; ARB, angiotension receptor blocker; ALD, aldosterone. Denardo et al Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 return of the reflected wave from the periphery to the heart, a shorter Tr, and a longer systolic duration of the reflected wave (SDR).4,7 Aortic augmentation index (AIa), a measure of wave reflection intensity, can be estimated as the ratio of wave reflection amplitude (Ps⫺Pi) and cPP (Ps⫺Pd). When the reflected wave returns during systole as a result of increased PWV and/or decreased reflection site distance, as seen in Figure 1, the aortic pressure is augmented in late systole, and, therefore, the LV must generate enough effort to overcome this augmentation in pressure and opposition to emptying during flow deceleration.4 This pressure effort, which takes into account both amplitude and SDR, is wasted (ie, wasted effort, Ew) because it does not contribute to blood flow production and can be estimated as the area under the systolic portion of the reflected wave.26 Ew is that portion of the systolic pressure time index (SPTI) resulting from wave reflection and is directly related to LV hypertrophy.26 The SPTI is directly related to myocardial oxygen demand and is estimated as the area under the systolic portion of the aortic pressure wave above zero.27 The pressure systolic area (PSA) is the area under the systolic portion of the aortic pressure wave above diastolic pressure. When Ew is small or zero, PSA is directly related to stroke volume and is dependent AoPW and LV Systolic Dysfunction 151 on ejection duration and cPP. Diastolic pressure time index (DPTI) is an estimate of coronary artery perfusion pressure and is related to coronary blood flow and is estimated as the area under the diastolic portion of the pressure wave. The ratio of DPTI/SPTI represents the ratio of myocardial supply and demand and is termed the myocardial viability ratio.28 The ratio of bPP and cPP is the pressure pulse amplification, and it increases as arterial stiffness and wave reflection amplitude decrease and vice versa.4 Only high-quality recordings, defined as an in-device quality index of ⬎80% (derived from an algorithm including average pulse height, pulse height variation, diastolic variation, and the maximum rate of rise of the peripheral waveform) and acceptable curves on visual inspection, were included in the analysis. Statistical Analysis Data for continuous variables are presented as mean⫾SD. Comparisons between individual hemodynamic variables obtained from the 2 matched groups were made using a paired 2-tailed Student t test. Comparisons within the LVSD patients were made using an unpaired 2-tailed Student t test. Statistical significance was assumed when probability values were ⬍0.05. Figure 2. Illustration showing the alterations in noninvasively measured radial artery and synthesized aortic pressure waves in a patient with heart failure and severe LVSD (lower panel) compared to a normal subject (upper panel) with similar heart rate, height and age. Ejection duration (270 versus 322 ms), percent systolic duration (31 versus 36%), unaugmented pressure (21 versus 29 mm Hg), augmented pressure (1.0 versus 13 mm Hg), and AIa are reduced in the heart failure patient resulting in diminished wasted LV effort (96 versus 1887 dyne sec/cm2), SPTI (1880 versus 2355 mm Hg sec/min) and PSA (301 versus 627 mm Hg sec/min). In this example, mean arterial pressure was similar between the two (96 versus 98 mm Hg) while both peripheral (36 versus 50 mm Hg) and central (22 versus 41 mm Hg) pulse pressures were less in the heart failure patient. Pi is the inflection point and denotes the beginning upstroke of the reflected wave. The radial artery pressure wave of the heart failure patient displays a dicrotic wave while the aortic pressure wave does not. 152 Circ Heart Fail January 2010 Statement of Responsibility The authors had full access to the data and take responsibility for its integrity. All authors have read and agree to the manuscript as written. Results Patients and Subjects The LVSD patients and normal subjects were well matched with regard to age, gender, height, body mass index, and heart rate (Table 1). The mean EF for the 25 LVSD patients was 24⫾8.8% (range, 11% to 40%; 21 patients ⬍30% and 4 patients ⱖ30%). Additionally, the LVSD patients had multiple risk conditions, and they were on multiple medications oriented toward the management of severe LVSD. Table 2. Measured and Calculated Variables for LVSD Patients and Normal Subjects Variable Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 All measured and calculated variables for the normal subjects were similar to those previously published for other normal subjects.29 An example of the radial artery pressure wave and the synthesized central AoPW obtained in a normal subject and a LVSD patient is shown in Figure 2. The measured bSP and bDP were each significantly less in LVSD patients compared with normal subjects (Table 2), as was the calculated bPP. Additionally, the measured central systolic blood pressure, central mean pressure, cPP, and calculated unaugmented pressure (ie, forward wave amplitude [Pi⫺Pd]) were each less in LVSD patients. Also, ejection duration (Figure 3), percent systolic duration, and PSA were each less in the LVSD patients. However, pulse pressure amplification was greater in the LVSD patients compared with normal subjects. Amplitude and Timing of Wave Reflection Indices The amplitude (augmented pressure) and systolic duration (SDR) of the reflected pressure wave were both less in the LVSD patients compared with the normal subjects (Table 2; Figure 3). Additionally, Tr of the pressure wave to and from the periphery was greater. This delay in return of the reflected wave to the heart indicates a decrease in PWV and/or an increase in reflection site distance. These differences in wave reflection characteristics produced a lower AIa and suggest a decrease in wave reflection intensity and arterial stiffness in the LVSD patients. This contention is also supported by the increase in pulse pressure amplification. Indices of Myocardial Oxygen Demand The observed differences in arterial wall properties and wave reflection characteristics indicate a significant reduction in pulsatile LV afterload. These afterload changes were associated with a decrease in indices of myocardial oxygen demand. The decrease in wave reflection amplitude and duration in the LVSD patients caused a decrease in Ew (Table 2; Figure 3). Also, the decreased central systolic blood pressure and abbreviated ejection duration in LVSD patients caused a decrease in the cross product (heart rate⫻central systolic blood pressure) and estimated SPTI compared with the normal subjects. Finally, DPTI was decreased in the LVSD patients. These area changes in systole and diastole caused an increase in the myocardial viability ratio. Normal Subjects (N⫽25) P bSP, mm Hg 111⫾17 134⫾18 ⬍0.001 bDP, mm Hg 71⫾13 78⫾10 ⬍0.04 bPP, mm Hg 40⫾9.5 56⫾11 ⬍0.001 cSP, mm Hg 100⫾16 121⫾16 ⬍0.001 cMP, mm Hg 83⫾14 98⫾12 ⬍0.001 cPP, mm Hg 28⫾7.4 42⫾9.5 ⬍0.001 Unaugmented pressure, mm Hg 24⫾6.3 32⫾6.4 ⬍0.001 277⫾22 299⫾25 ⬍0.002 32⫾5.3 35⫾4.0 ⬍0.02 PSA, mm Hg-sec/min 383⫾121 666⫾150 ⬍0.001 Augmented pressure, mm Hg 4.8⫾3.1 9.6⫾4.5 ⬍0.001 SDR, ms 134⫾24 167⫾26 ⬍0.001 Tr, ms 147⫾10 132⫾21 ⬍0.001 AIa, % 12⫾6.6 23⫾7.6 ⬍0.006 Pulse pressure amplification (dimensionless) 1.5⫾0.11 1.4⫾0.09 ⬍0.008 17⫾10⫻102 ⬍0.001 87⫾19⫻102 ⬍0.002 Ejection duration, ms Components of Peripheral Brachial and Central Aortic Blood Pressure LVSD Patients (N⫽25) Percent systolic duration, % Ew, dyne-sec/cm2 5.3⫾2.8⫻102 2 Cross Product 关HR⫻cSP], mm Hg/min 69⫾17⫻10 SPTI, mm Hg sec/min 17⫾4.1⫻102 23⫾4.2⫻102 ⬍0.001 DPTI, mm Hg sec/min 2 32⫾6.0⫻10 35⫾4.6⫻102 ⬍0.03 1.9⫾0.52 1.6⫾0.27 ⬍0.002 DPTI/SPTI (dimensionless) b indicates brachial; c, central; SP, systolic pressure; DP, diastolic pressure; PP, pulse pressure; MP, mean pressure; unaugmented pressure, (Pi⫺Pd); augmented pressure, (Ps⫺Pi); SDR, systolic duration of reflected wave; Tr, round-trip travel time of the pressure wave; AIa, augmentation index; Ew, wasted effort; HR, heart rate; SPTI, systolic pressure time index; DPTI, diastolic pressure time index; DPTI/SPTI, myocardial viability ratio. Intragroup Comparison of LVSD Patients Based on LVEF Among the LVSD patients, those with LVEF ⱕ20% (N⫽11) compared with those with LVEF ⬎20% (N⫽14) primarily contributed to the decrease in percent systolic duration (29⫾ 4.6% versus 34⫾5.6%; P⬍0.04), PSA (348⫾86 mm Hg sec/ min versus 429⫾126 mm Hg sec/min; P⬍0.02), and SPTI (1484⫾232 mm Hg sec/min versus 1924⫾428 mm Hg sec/ min; P⬍0.01). Otherwise, the data from these 2 subgroups appeared similar. Discussion The results of this study indicate that PWA of the AoPW, determined using noninvasive, high-fidelity tonometry of the radial artery, can describe the effects of severe LVSD and altered arterial properties on ventricular/vascular coupling in the time domain. In this description, there was a decrease in all components of both central and peripheral blood pressure Denardo et al AoPW and LV Systolic Dysfunction 153 Figure 3. Bar graphs showing average values in normal subjects (light bars) and patients with severe LVSD (dark bars) of ejection duration (299⫾25 versus 278⫾21 ms), reflected wave amplitude (9.6⫾4.5 versus 3.7⫾2.4 mm Hg), SPTI (2335⫾418 versus 1731⫾414 mm Hg sec/min), and wasted LV pressure effort (1680⫾1021 versus 534⫾380 dyne sec/cm2). Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 (systolic, diastolic, pulse, and mean) compared with normal subjects. Similar observations for peripheral blood pressure have been made in this population by others, and a low bPP has been found to be independently associated with increased mortality.16 –18 Earlier studies, including the Systolic Hypertension in the Elderly (SHEP) and Survival and Ventricular Enlargement (SAVE) studies, found that increased conduit artery stiffness, as assessed by bPP, may contribute to increased adverse outcomes in patients with LV dysfunction.30 –32 These studies, however, only measured the extremes in brachial blood pressure (ie, bPP⫽bSP⫺bDP), whereas in our study, the central AoPW, a more accurate indicator of LV afterload and adverse outcome, was measured. Several other studies have measured central AoPW, but most of those studies were performed in patients with mild-to-moderate LVSD (LVEF 30% to ⬎40%),20,22,23,33–35 whereas our study was performed primarily in patients with severe LVSD (21 of 25). Most of the earlier studies found no change in aortic PWV and travel time of the pressure wave to and from the periphery. However, in contrast to those results, we found an increase in Tr of the pressure wave, indicating a decrease in PWV, and an increase in pulse pressure amplification, which together imply a decrease in arterial stiffness and is consistent with the measured decrease in augmented pressure and AIa. Our results are supported by the results of Tartière et al,33 which involved patients with a similar EF (mean LVEF 24⫾9% among study patients with reduced EF) and which showed a decrease in the effects of wave reflection on AoPW. These pressure changes result from altered ventricular/vascular coupling. In systolic heart failure, when ventricular contractility is severely impaired, wave reflection does not boost late systolic pressure because the LV is incapable of responding adequately, so that systole is terminated prematurely, and wave reflection has a negative influence on the flow wave during deceleration and in heart failure shortens ejection duration.36 Additional novel characteristics of the AoPW in severe LVSD shown in this study include decreased unaugmented pressure, ejection duration, SDR, percent systolic duration and indices of myocardial oxygen demand, and LV function including unaugmented pressure, PSA, Ew, cross product, and SPTI. Most previous studies performed in patients with mild to moderate heart failure (LVEF 30% to ⬎40%) showed an increase or no change in arterial stiffness. Only one previous study reported a decrease in arterial stiffness and PWV similar to our findings; this was the study by Tartière et al,33 performed in patients with severe LVSD and reduced mean arterial pressure. Because the activities of the LV and peripheral arterial system are interactive (ventricular/vascular coupling), the decrease in arterial stiffness and PWV may be the result of a decrease in mean arterial pressure in response to reduced cardiac output and LV afterload. This decreased arterial stiffness and wave reflection— essentially, a decrease in impedance—is partly because of the effect of arterial vasodilating drugs and a decrease in mean arterial pressure which is probably just a marker of severe LV dysfunction. In both the Tartière et al33 study and this study, a majority of the LVSD patients received either angiotensin converting enzyme inhibiting or angiotension receptor blocking drugs, which decrease peripheral arterial stiffness directly (actively) and central arterial stiffness indirectly (passively). The measured decreases in systolic unaugmented pressure, Ew, and SPTI shown in this study are the result of a decrease in LV contractile function and consequent inability to generate force and pressure to overcome the augmented pressure associated with the severe LVSD resulting in reduced stroke volume and PSA. The decrease in SPTI and cross product indicate a consequent decrease in LV oxygen requirements, and the increase in DPTI/SPTI indicates an increase in myocardial viability ratio. This may serve as a compensatory mechanism in severe LVSD to optimize efficiency of the failing LV. Morphological changes in the pressure wave contour in systolic heart failure were reported well over a hundred years ago. Flemming suggested in 1881 that the necessary conditions for the presence of 2 distinct upstrokes in the peripheral 154 Circ Heart Fail January 2010 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 Figure 4. Illustration showing changes in the AoPW that occur during the development and progression of LVSD. A, Young normal healthy subject with reflected wave occurring predominately in diastole; ejection duration (broken line) is 316 ms, cPP is 26 mm Hg, SPTI is 2047 mm Hg sec/min and PSA is 440 mm Hg sec/min. B, During aging and develop of hypertension the reflected wave (amplitude 23 mm Hg in this example) occurs almost entirely in systole resulting in an increase in AIa, wasted effort, cPP (59 mm Hg), SPTI (3206 mm Hg sec/min) and PSA (802 mm Hg sec/min) causing LV hypertrophy which begins the process of systolic heart failure. C, As heart failure proceeds reflected wave amplitude (7 mm Hg), AIa, cPP, ejection duration (269 ms), SPTI (2196 mm Hg sec/min), and PSA (558 mm Hg sec/min) begin to decrease. D, In LVSD, the augmented systolic pressure and wasted effort become almost zero, LV ejection is shortened further (235 ms) which causes a reduction in SPTI (1535 mm Hg sec/min), percent systolic duration (28%) and PSA (361 mm Hg sec/min). pulse wave often seen in heart failure included a fast pulse, elastic vessels, feeble tension in the vessels, and a small amount of blood injected with each ventricular systole.37 A few years later, Lewis38 described a characteristic dicrotic (twice-beating) pulse, which is typical in patients with LVSD resulting from cardiogenic shock after myocardial infarction,3,4,39 after open heart surgery40 and in cardiomyopathy.41,42 Such morphological changes in pulse contour with LVSD are confined to the peripheral pulse and are seldom seen in the AoPW.43 Fifty-six percent of the patients in our study displayed a dicrotic wave in the radial pulse (Figure 2). An explanation for the progression from normal LV systolic function to severe LVSD is available on the basis of the argument proposed by Westerhof and O’Rourke36 and Nichols and O’Rourke.4 This explanation has been effectively used to characterize mechanical pumps, with the LV seen to act as a flow source (powerful ejection) in youth when the ventricle is optimally matched to a compliant arterial system and power generation is minimal. Under these circumstances, stroke volume is directly related to PSA and the reflected wave arrives in diastole (Figure 4A) and aids in coronary artery perfusion. The age-related increase in elastic artery stiffness (and PWV) causes the reflected wave to arrive earlier to the heart and boost pressure in late systole that places an extra pulsatile workload on the LV causing it to generate more force, which is wasted effort. These changes in arterial properties and wave reflection characteristics cause the LV to change from a flow source to a combined flow and pressure source (ejection limited by pressure achieved) as hypertension develops (Figure 4B). As the elastic arteries become stiffer, the LV becomes primarily a pressure source and the myocardial oxygen demand is greater. Sustained elevation and prolongation of late systolic augmentation results in LV hypertrophy,26,44,45 which is associated with progressive degenerative changes in the myocytes such that these weaken and develop less force with each contraction. The weakened, hypertrophied fibers lengthen and the LV dilates, with augmented systolic pressure and stroke output initially being maintained (Figure 4C) at greater muscle length and LV volume through the Frank-Starling mechanism.3,4 The LVEF in these patients is usually ⱕ40%. Ultimately, compensation is lost and the LV cannot generate the extra force necessary to completely overcome the late systolic augmented pressure. Augmented pressure, AIa, and Denardo et al systolic (and pulse) pressure are therefore reduced and associated with a decrease in ejection duration, Ew, PSA, SPTI, and stroke volume. The LVEF in these patients is usually ⬍30%.33 When LV contractility is severely impaired, wave reflection does not boost systolic pressure (Figure 4C) because the heart is incapable of responding, so that systole is terminated prematurely, and wave reflection is seen to have had a negative influence on flow rather than a positive influence on pressure3,33 and the LV reverts back to a flow source (weak and abbreviated ejection) as heart failure progresses (Figure 4D). Again there is a direct positive relation between stroke volume and PSA; therefore, an improvement in hemodynamics will be viewed as an increase in ejection duration, augmented pressure, pulse pressure, and PSA.9 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 Limitations This study has one principal limitation. The radial artery pressure waveforms were calibrated using cuff measured brachial systolic and diastolic pressure. However, this method of calibration may result in an overestimation of the central aortic pressures.46,47 Nonetheless, this overestimation should be a systematic error and affect all results proportionately. Conclusions PWA of the AoPW may provide more detailed and accurate information into the severity of LV dysfunction compared with the measures of brachial pulsatility. This information may prove vital in the diagnosis and risk stratification of patients with LV dysfunction, especially when severe, and yet may be performed accurately in the outpatient clinic setting. Further standardization of AoPW findings in LVSD patients may allow for the clinical use of arterial PWA to noninvasively characterize reduced LV systolic performance, including severe LVSD and aid in logical therapy. Disclosures Dr Nichols is a consultant for AtCor Medical (Sydney, Australia). References 1. Westerhof N, Sipkema P, van den Bos GC, Elzinga G. Forward and backward waves in the arterial system. Cardiovasc Res. 1972;6:648 – 656. 2. Murgo JP, Westerhof N, Giolma JP, Altobelli SA. Aortic input impedance in normal man: relationship to pressure wave forms. Circulation. 1980;62:105–116. 3. O’Rourke MF. Time domain analysis of the arterial pulse in clinical medicine. Med Biol Eng Comput. 2009;47:119 –129. 4. Nichols WW, O’Rourke MF. McDonald’s Blood Flow in Arteries: Theoretic, Experimental and Clinical Principles. 5th ed. London: Edward Arnold; 2005. 5. Adji A, Hirata K, Hoegler S, O’Rourke MF. Noninvasive pulse waveform analysis in clinical trials: similarity of two methods for calculating aortic systolic pressure. Am J Hypertens. 2007;20:917–922. 6. O’Rourke MF, Hashimoto J. Pressure pulse waveform analysis in critical care. Crit Care Med. 2006;34:1569 –1570. 7. Nichols WW, Denardo SJ, Wilkinson IB, McEniery CM, Cockcroft J, O’Rourke MF. Effects of arterial stiffness, pulse wave velocity, and wave reflections on the central aortic pressure waveform. J Clin Hypertens (Greenwich). 2008;10:295–303. 8. Haider AW, Larson MG, Franklin SS, Levy D; Framingham Heart Study. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study. Ann Intern Med. 2003;138:10 –16. AoPW and LV Systolic Dysfunction 155 9. Safar ME. Systolic blood pressure, pulse pressure and arterial stiffness as cardiovascular risk factors. Curr Opin Nephrol Hypertens. 2001;10: 257–261. 10. Blacher J, Asmar R, Djane S, London GM, Safar ME. Aortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patients. Hypertension. 1999;33:1111–1117. 11. London GM, Blacher J, Pannier B, Guérin AP, Marchais SJ, Safar ME. Arterial wave reflections and survival in end-stage renal failure. Hypertension. 2001;38:434 – 438. 12. Mark PB, Doyle A, Blyth KG, Patel RK, Weir RA, Steedman T, Foster JE, Dargie HJ, Jardine AG. Vascular function assessed with cardiovascular magnetic resonance predicts survival in patients with advanced chronic kidney disease. J Cardiovasc Magn Reson. 2008;10:39. 13. Jankowski P, Kawecka-Jaszcz K, Czarnecka D, Brzozowska-Kiszka M, Styczkiewicz K, Loster M, Kloch-Badełek M, Wiliński J, Curyło AM, Dudek D; Aortic Blood Pressure and Survival Study Group. Pulsatile but not steady component of blood pressure predicts cardiovascular events in coronary patients. Hypertension. 2008;51:848 – 855. 14. Pini R, Cavallini MC, Palmieri V, Marchionni N, Di Bari M, Devereux RB, Masotti G, Roman MJ. Central but not brachial blood pressure predicts cardiovascular events in an unselected geriatric population: the ICARe Dicomano Study. J Am Coll Cardiol. 2008;51:2432–2439. 15. Roman MJ, Devereux RB, Kizer JR, Lee ET, Galloway JM, Ali T, Umans JG, Howard BV. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the Strong Heart Study. Hypertension. 2007;50:197–203. 16. Voors AA, Petrie CJ, Petrie MC, Charlesworth A, Hillege HL, Zijlstra F, McMurray JJ, van Veldhuisen DJ. Low pulse pressure is independently related to elevated natriuretic peptides and increased mortality in advanced chronic heart failure. Eur Heart J. 2005;26:1759 –1764. 17. Aronson D, Burger AJ. Relation between pulse pressure and survival in patients with decompensated heart failure. Am J Cardiol. 2004;93: 785–788. 18. Schillaci G, Di Luzio S, Coluccini M, Gonzini L, Porcu M, Pozzar F, Maggioni AP; Italian Network of Congestive Heart Failure Registry. A low pulse pressure is an independent predictor of mortality in heart failure: data from a large nationwide cardiology database (IN-CHF Registry). Ital Heart J. 2004;5:892– 898. 19. Giannattasio C, Achilli F, Failla M, Capra A, Vincenzi A, Valagussa F, Mancia G. Radial, carotid and aortic distensibility in congestive heart failure: effects of high-dose angiotensin-converting enzyme inhibitor or low-dose association with angiotensin type 1 receptor blockade. J Am Coll Cardiol. 2002;39:1275–1282. 20. Mitchell GF, Tardif JC, Arnold JM, Marchiori G, O’Brien TX, Dunlap ME, Pfeffer MA. Pulsatile hemodynamics in congestive heart failure. Hypertension. 2001;38:1433–1439. 21. Pepine CJ, Nichols WW, Conti CR. Aortic input impedance in heart failure. Circulation. 1978;58:460 – 465. 22. Curtis SL, Zambanini A, Mayet J, McG Thom SA, Foale R, Parker KH, Hughes AD. Reduced systolic wave generation and increased peripheral wave reflection in chronic heart failure. Am J Physiol Heart Circ Physiol. 2007;293:H557–H562. 23. Weber T, Auer J, Lamm G, O’Rourke MF, Eber B. Arterial stiffness, central blood pressures, and wave reflections in cardiomyopathyimplications for risk stratification. J Card Fail. 2007;13:353–359. 24. Pauca AL, O’Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001;38:932–937. 25. O’Rourke MF. Ascending aortic pressure wave indices and cardiovascular disease. Am J Hypertens. 2004;17:721–723. 26. Hashimoto J, Nichols WW, O’Rourke MF, Imai Y. Association between wasted pressure effort and left ventricular hypertrophy in hypertension: influence of arterial wave reflection. Am J Hypertens. 2008;21:329 –333. 27. Sarnoff SJ, Braunwald E, Welch GH Jr, Case RB, Stainsby WN, Macruz R. Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension-time index. Am J Physiol. 1958;192: 148 –156. 28. Buckberg GD, Fixler DE, Archie JP, Hoffman JI. Experimental subendocardial ischemia in dogs with normal coronary arteries. Circ Res. 1972;30:67– 81. 29. McEniery CM, Yasmin Hall IR, Qasem A, Wilkinson IB, Cockcroft JR. Normal vascular aging: differential effects on wave reflection and aortic pulse wave velocity: the Anglo-Cardiff Collaborative Trial (ACCT). J Am Coll Cardiol. 2005;46:1753–1760. 156 Circ Heart Fail January 2010 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 30. Domanski MJ, Mitchell GF, Norman JE, Exner DV, Pitt B, Pfeffer MA. Independent prognostic information provided by sphygmomanometrically determined pulse pressure and mean arterial pressure in patients with left ventricular dysfunction. J Am Coll Cardiol. 1999;33: 951–958. 31. Kostis JB, Lawrence-Nelson J, Ranjan R, Wilson AC, Kostis WJ, Lacy CR. Association of increased pulse pressure with the development of heart failure in SHEP. Systolic Hypertension in the Elderly (SHEP) Cooperative Research Group. Am J Hypertens. 2001;14:798 – 803. 32. Mitchell GF, Moyé LA, Braunwald E, Rouleau JL, Bernstein V, Geltman EM, Flaker GC, Pfeffer MA. Sphygmomanometrically determined pulse pressure is a powerful independent predictor of recurrent events after myocardial infarction in patients with impaired left ventricular function. SAVE investigators Survival and Ventricular Enlargement. Circulation. 1997;96:4254 – 4260. 33. Tartière JM, Logeart D, Safar ME, Cohen-Solal A. Interaction between pulse wave velocity, augmentation index, pulse pressure and left ventricular function in chronic heart failure. J Hum Hypertens. 2006;20: 213–219. 34. Hirata K, Adji A, Vlachopoulos C, O’Rourke MF. Effect of sildenafil on cardiac performance in patients with heart failure. Am J Cardiol. 2005; 96:1436 –1440. 35. Ooi H, Chung W, Biolo A. Arterial stiffness and vascular load in heart failure. Congest Heart Fail. 2008;14:31–36. 36. Westerhof N, O’Rourke MF. Haemodynamic basis for the development of left ventricular failure in systolic hypertension and for its logical therapy. J Hypertens. 1995;13:943–952. 37. Flemming WJ. Pulse dicrotism. J Anatomy Physiol. 1881;15:278 –291. 38. Lewis T. The factors influencing the prominence of the dicrotic wave. J Physiol. 1906;34:414 – 429. 39. O’Rourke MF. The arterial pulse in health and disease. Am Heart J. 1971;82:687–702. 40. Orchard RC, Craige E. Dicrotic pulse after open heart surgery. Circulation. 1980;62:1107–1114. 41. Ewy GA, Rios JC, Marcus FI. The dicrotic arterial pulse. Circulation. 1969;39:655– 661. 42. Smith D, Craige E. Mechanism of the dicrotic pulse. Br Heart J. 1986; 56:531–534. 43. Wiggers CJ. The Pressure Pulses in the Cardiovascular System. London: Longmans, Green and Co; 1928. 44. Iketani T, Iketani Y, Takazawa K, Yamashina A. The influence of the peripheral reflection wave on left ventricular hypertrophy in patients with essential hypertension. Hypertens Res. 2000;23:451– 458. 45. Watabe D, Hashimoto J, Hatanaka R, Hanazawa T, Ohba H, Ohkubo T, Kikuya M, Totsune K, Imai Y. Electrocardiographic left ventricular hypertrophy and arterial stiffness: the Ohasama study. Am J Hypertens. 2006;19:1199 –1205. 46. Verbeke F, Segers P, Heireman S, Vanholder R, Verdonck P, Van Bortel LM. Noninvasive assessment of local pulse pressure: importance of brachial-to-radial pressure amplification. Hypertension. 2005;46: 244 –248. 47. Segers P, Mahieu D, Kips J, Rietzschel E, De Buyzere M, De Bacquer D, Bekaert S, De Backer G, Gillebert T, Verdonck P, Van Bortel L. Asklepios investigators. Amplification of the pressure pulse in the upper limb in healthy, middle-aged men and women. Hypertension. 2009;54:414 – 420. CLINICAL PERSPECTIVE The effect of moderate left ventricular systolic dysfunction on ventricular/vascular coupling and the aortic pressure waveform has been well described, but the effect of severe left ventricular systolic dysfunction has not. This research shows that severe left ventricular systolic dysfunction causes measurable changes in the aortic pressure waveform, as determined using noninvasive, high-fidelity tonometry of the radial artery and a mathematical transfer function. Standardization of aortic pressure waveform findings in left ventricular systolic dysfunction patients may allow for the clinical use of radial artery pulse wave analysis to noninvasively determine the severity of dysfunction and aid in logical therapy. Pulse Wave Analysis of the Aortic Pressure Waveform in Severe Left Ventricular Systolic Dysfunction Scott J. Denardo, Ramavathi Nandyala, Gregory L. Freeman, Gary L. Pierce and Wilmer W. Nichols Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 13, 2017 Circ Heart Fail. 2010;3:149-156; originally published online November 10, 2009; doi: 10.1161/CIRCHEARTFAILURE.109.862383 Circulation: Heart Failure is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2009 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 1941-3297 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circheartfailure.ahajournals.org/content/3/1/149 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Heart Failure can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Heart Failure is online at: http://circheartfailure.ahajournals.org//subscriptions/