Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
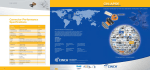
REPRINT December 2015 COVER STORY Daniel J. Marino William Faber Meredith Duncan healthcare financial management association hfma.or g patient access innovations integrating patients within the system of care As the nation’s healthcare system continues to be reshaped by the forces of reform, increased patient engagement will emerge as a defining outcome of this profound transformation. Provider coordination is of paramount importance for healthcare organizations preparing for the industry’s shift in focus from volume to value. The most ambitious coordination model that has been developed to date is the clinically integrated network (CIN)—a contractual collaboration among hospitals, physicians, and other providers to manage patients across the entire continuum of care. A CIN uses population health management tools, including care management techniques, to build value through improving patient outcomes and controlling costs. This innovative model offers providers access to value-based payment contracts and an opportunity to improve quality and reduce costs. Despite the compelling benefits of clinical integration, this approach also poses risks. Value-based payment contracts hold CIN participants accountable for both clinical and financial outcomes, although the ability to influence these outcomes depends largely on patient choice and patient compliance. Whenever a patient leaves the CIN, even if the patient returns to the network for certain services, network providers lose the opportunity to fully manage the patient’s care and utilization, ultimately undercutting their ability to coordinate the patient’s care and accrue the benefits of improved clinical outcomes and reduced costs. This risk makes it critically important for CINs to keep patients within their organized systems of care. CINs need to make sure patients can access the network easily and are motivated to stay connected, requiring a strategic focus on patient access and engagement. AT A GLANCE Clinically integrated networks seeking to ensure in-network access and strengthen patient engagement should adopt five strategic areas of focus: >> Extend access beyond traditional models >> Manage out-migration >> Make it easy for patients to stay in the network >> Build patient engagement into clinical care models >> Explore innovative methods to engage patients hfma.org December 2015 1 COVER STORY A PATIENT ACCESS AND ENGAGEMENT MODEL FOR CLINICALLY INTEGRATED NETWORKS Expand Access: > Nontraditional > Convenience > Leverage Mid-Level Practitioners Clinically Integrated Network Boost Engagement: > Education > Technology > Social Media Minimize Leakage: > Care Pathways > Partnerships > Narrow Networks Source: The Camden Group Based on the experiences of leading CINs, strategies aimed at improving patient access tend to be most effective when they are focused on three primary objectives: expanding entry points to the network, making access more convenient and inexpensive, and keeping patients engaged in the care they receive from network providers. The following five strategies, in particular, have been proven effective for ensuring in-network access and strengthening patient engagement. Extend Access Beyond Traditional Models Traditionally, healthcare access has been understood in terms of the patient-provider relationship, with patient access usually defined as a patient’s ability to schedule an appointment with a physician or other healthcare service provider. This definition continues to be prevalent because traditional fee-for-service reimbursement covers only face-to-face provider encounters, and organizations have long seen strong physician relationships as the key to acquiring and retaining patients. Health care also has seen the steady growth of new access models built around nontraditional care 2 December 2015 healthcare financial management delivery. Examples include urgent care centers and, more recently, retail healthcare clinics. Patients visit retail clinics because they provide convenient access to services such as vaccinations, sports physicals, basic health screenings, and simple lab tests. For more pressing medical problems, urgent care centers provide a fast and relatively inexpensive alternative to hospital emergency departments (EDs). Many CIN leaders see retail and urgent care centers as a threat because of the potential for these centers to siphon patients away from a CIN’s organized system of care. However, this view is shortsighted. CINs also have the option of adopting these nontraditional delivery models, thereby creating new access points to network providers. Such a strategy provides three important benefits. Better cost management. The urgent care and retail clinic delivery models promote cost management because they allow the network to address patients’ low-acuity problems in a low-cost setting. Patients with flu symptoms, sore throat, or minor cuts, for example, can receive effective care without using expensive physician or hospital resources. More comprehensive care management. CINs that incorporate retail and urgent care can better manage patients’ needs across the continuum of care. Suppose an older patient goes to a retail clinic for an infection and gets a prescription for an antibiotic. If the clinic is linked to a CIN, the patient’s primary care provider could follow up directly with the patient to make sure the prescription is working. The model also could be used proactively. For example, hypertensive patients could be directed to conveniently located CIN retail clinics for their periodic blood pressure check, promoting compliance while allowing the network to monitor test results. COVER STORY Enhanced marketing opportunities. Greater convenience and lower costs can be strong selling points for a CIN. Nontraditional access is especially important for appealing to patients with high-deductible health plans, because nontraditional settings provide certain kinds of care at lower out-of-pocket expense. Because patients bear most of these expenses until their yearly deductibles are met, patients with high-deductible plans tend to be focused on costs and convenience. For most CINs, the best way to leverage nontraditional access is to partner with existing providers. For example, Providence Health recently announced a partnership with Walgreens to create retail health clinics in up to 25 stores in Washington and Oregon. The clinics will be staffed by advanced practice nurses and will be fully integrated with Providence Health’s electronic health records. Retail clinic partnerships can be structured in several ways. Typically, no money changes hands between the CIN and the retail clinic organization, because the partnership represents an opportunity for both parties to benefit from the arrangement. However, a CIN could offer its retail partner incentive payments based on performance. For example, the clinic could receive bonus payments based on meeting patient wait-time benchmarks. When pursuing a nontraditional access strategy, a CIN should take three steps. First, it should educate patients on the availability of nontraditional access and how they can benefit from it. Patients should understand the available care settings (e.g., retail clinic, urgent care center, physician office, hospital ED) and how each setting can help them optimize their health and minimize their costs. Second, CINs should establish robust data sharing among network providers and nontraditional access points, with the objective of helping primary care providers stay fully informed of the services their patients have received at these nontraditional points of care. Such data sharing not only supports better coordination of care but also helps primary care providers feel more comfortable directing patients to retail and urgent clinics when appropriate. Third, CINs should pay attention to the attribution model outlined in payer contracts. Typically, insurance products that use an attribution model assign global responsibility for the medical spend and quality of care to the primary care provider that the patient sees most often over a period of time. Contracts often require primary care oversight of retail or urgent care activities. One way to meet this requirement is to appoint a CIN physician to act as medical director for partner clinics. Aligning clinical practice with the contractual attribution methodology will ensure payment and help the CIN manage care, quality, and costs. Manage Out-Migration Some level of patient out-migration is unavoidable in any healthcare network. However, a CIN that is seeing an inordinately high outmigration of its patient population will have diminished ability to manage care at the population level. Managing out-migration is particularly important for high-risk and rising-risk patients, for whom costs of care can be significant, because the CIN must be able to coordinate care for such patients exclusively within its network to manage those costs effectively. The first step is to determine where out-migrating patients are accessing care. Claims data, by payer, can help the CIN identify specific providers and services that represent the bulk of leakage. With an understanding of why patients are leaving the hfma.org December 2015 3 COVER STORY network for outside care and where they are going, a CIN can use three strategies to address this challenge. Proactively steer patients to in-network providers. Effective care management processes can reinforce patients’ perception of the CIN as the appropriate setting for addressing their healthcare needs. For example, care management of patients with high blood pressure should include appropriate monitoring for kidney disease. Detecting kidney disease early creates the opportunity to refer patients to in-network nephrologists. Expand the network through new partnerships. Strong patterns of out-migration to certain specialties or providers may indicate the need for the CIN to expand its offerings. For instance, if a significant number of patients are using outof-network urologists, the CIN might want to consider bringing new urology providers into its network. If a partnership with the out-of-network provider preferred by the CIN’s patients is not feasible, the CIN should at least pursue a data-sharing agreement. For example, if patients with cancer are leaving a network to receive treatment at an academic medical center (AMC), an effective strategy for the CIN might be to negotiate an agreement with the AMC to exchange medical records for these shared patients. This approach may not help the CIN control the direct cost of cancer services, but it will help the CIN’s providers deliver more coordinated care overall. Negotiate narrow network contracts. Direct contracting with employers is emerging as a strong option for CINs. Under narrow network contracts, employees pay reduced fees for receiving care from CIN providers. These contracts are another means to influence costs and quality by steering 4 December 2015 healthcare financial management patients to high-value providers within the network. Make It Easy for Patients to Stay in the Network Even with the rise of nontraditional access points, physicians remain an important entry point for patients who receive care from CINs. To make accessing a physician appointment as simple as possible for patients, CINs should focus on optimizing the scheduling process, expanding accessibility, and increasing capacity by using mid-level providers. Optimize the scheduling process. Top physician organizations have developed convenient, user-friendly scheduling systems that allow patients to schedule appointments easily. These organizations have well-designed appointment reminder systems for keeping no-shows to an absolute minimum, and use care coordinators to follow up on diagnostic orders, specialist referrals, and other recommended services. The entire system is focused on helping patients to receive the services they need in the appropriate setting when they need them. Expand accessibility. For many patients, appointment access is limited by traditional medical office hours, commonly 9 a.m. to 4 p.m. CINs should consider requiring providers, especially primary care practices, to establish “open access” scheduling and to expand hours that enable same-day or next-day appointments. Practices also can schedule some providers to be available later in the day (for example, from 3 to 8 p.m.) to accommodate patients’ work and school hours. Increase capacity by using mid-level providers. Practices patterned after the patient-centered medical home (PCMH) model emphasize the use of mid-level providers to handle routine services, answer patient questions, provide follow-up COVER STORY services, and coordinate patient care. The PCMH model improves patient access to care while freeing physicians to focus on more complex patients. It is important to communicate the “value proposition” to both patients and physicians: Patients gain faster access to the provider team; quality is maintained and potentially increased; and costs are held down for both patients and the system. Build Engagement into Clinical Care One often-overlooked opportunity to improve patient access is to use clinical processes to foster greater patient engagement. CINs can realize this opportunity by developing comprehensive clinical protocols and care pathways for common diseases and services. For example, a CIN’s clinical protocols for osteoporosis should specify all recommended specialist consultations, nutritional counseling, and guidelines for medical treatment. The existence of comprehensive clinical protocols can promote better outcomes by improving patient compliance and enabling staff to proactively identify potential complications and refer patients to the appropriate level of care. As with efforts to steer patients to in-network providers, a strategy to promote greater patient engagement can benefit from comprehensive care management protocols. Another way engagement can be built into clinical care is to emphasize education early in the care encounter. Typically, when a patient is hospitalized for an acute condition, staff provides education and instructions immediately before discharge. At this point, however, patients will tend to be focused on getting out of the hospital and heading home, and may not be fully alert to the details in the instructions. Patients and caregivers are more likely to absorb and act on follow-up instructions if they are initially provided during treatment and then reinforced at discharge. Staff should talk with patients and family members early in the hospitalization about post-discharge care, potential medications, and best sites for follow-up care. This approach results in better compliance, which leads to improved outcomes. Explore Innovative Methods to Engage Patients Many leading CINs are working to develop patient engagement strategies that involve the use of emerging technologies. These organizations are exploring how to use social media to build stronger links with patients, among the following approaches. Use of smartphone apps to support patient selfmanagement and provider communication. Hundreds of apps are now available to help patients manage their health. The most advanced apps allow patients to share health information with their caregivers. For example, an app recently cleared by the U.S. Food and Drug Administration (FDA) allows patients with arrhythmia to take electrocardiogram readings using a smartphone and an add-on device. A patient can then email the results to his or her physician. An FDAcleared app for patients with asthma links to a sensor device that tracks inhaler use. Patients can share inhaler usage data with their providers, and providers can monitor data remotely to detect poor adherence or worsening conditions. These types of apps can help CINs stay in touch with patients and respond to potential problems early, enabling timely interventions to improve outcomes and control costs. Use of social media to support connected patient communities. A CIN in the eastern United States recently created a Facebook page for patients with a specific kind of cancer. Patients use the page to share their experiences, encourage each other, and ask questions. CIN staff monitor the discussion to answer patient questions and share hfma.org December 2015 5 COVER STORY targeted educational information. Monitoring the page also enables staff to identify patients who may be experiencing emerging problems and complications. CIN leaders report that the initiative has been well-received by patients. The strategy keeps patients engaged with their care and with their network caregivers. Use of claims data to predict health needs. Many healthcare organizations have begun to analyze claims data to identify patients at risk for poor outcomes or high utilization. For example, claims data might help identify patients with heart failure who are at risk for hospitalization. More specifically, an analytics program could detect a pattern of patient age, medication consumption, office visits, ED visits, diagnoses, and prior hospitalization to predict the likelihood that a patient with heart failure will be admitted within the next 30 days if the care team does not intervene. The weakness of this approach is that it is necessarily retrospective. However, leading CINs are beginning to use “big data” analytics to get a real-time view of patients’ health status. This approach focuses on social determinants of health. For example, a diabetic patient who experiences a job loss might be less able to control his or her disease due to stress or diet changes. Data analytics tools that identify the job loss event could help the CIN intervene proactively with special counseling and resources. Such an approach moves beyond risk stratification: The CIN is able to segment patients, much the same way that consumer goods companies segment the market. A Financial Imperative CINs have compelling financial reasons to optimize patient access. Cost reduction initiatives inevitably target redundant utilization. Care improvement efforts prioritize prevention over highly reimbursed interventional services. Care coordination activities add expense to the system and simultaneously decrease utilization of services for which systems are paid in a fee-forservice environment, making it incumbent on CINs to seek and participate in payment methodologies that reward quality and cost effectiveness. To make up for the loss of revenue from providing redundant or unnecessary services, a CIN must adopt a paradigm of expanding its patient base by providing patient access that emphasizes expanded entry points, patient convenience, cost efficiency, and strong patient engagement. By integrating patients within the organized system of care, a CIN can influence patient behavior and manage care and utilization, improving both patient outcomes and the organization’s bottom line. About the authors Daniel J. Marino, MBA, MPH, is executive vice president, GE Healthcare Camden Group, Chicago, and a member of HFMA’s First Illinois Chapter (dmarino@thecamdengroup. com). William K. Faber, MD, MHCM, is vice president, GE Healthcare Camden Group, Chicago, and a member of HFMA’s First Illinois Chapter ([email protected]). Meredith D. Duncan, MPH, is vice president, clinical integration and accountable care, Seton Health Alliance, Austin, Texas, and a member of HFMA’s South Texas Chapter (mdduncan@ seton.org). Reprinted from the December 2015 Early Edition of hfm magazine. Copyright 2015 by Healthcare Financial Management Association, Three Westbrook Corporate Center, Suite 600, Westchester, IL 60154-5732. For more information, call 800-252-HFMA or visit hfma.org.