Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
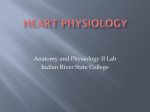
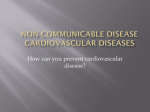
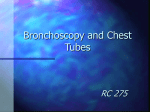
Intercostal Artery Laceration Following Thoracentesis Mary L Yacovone MEd RRT, Ritha Kartan MD, and Manuel Bautista MD Intercostal artery laceration is an unusual complication following thoracentesis, and has been reported only in elderly patients. We report a case of a 78-year-old man who developed a massive hemothorax following thoracentesis. Post-thoracentesis radiograph revealed a substantial increase in pleural fluid, and emergency chest tube insertion identified the hemothorax. He underwent right thoracotomy for repair of the intercostal artery laceration. Key words: intercostal artery laceration; thoracentesis; hemothorax; thoracotomy. [Respir Care 2010;55(11):1495–1498. © 2010 Daedalus Enterprises] Introduction Case Report Thoracentesis is a common diagnostic and therapeutic procedure, in which a percutaneously introduced needle is used to remove fluid from the pleural space. Clinically, the most common post-thoracentesis complication is pneumothorax, with an incidence of 3–30%.1-10 Table 1 lists postthoracentesis complications.1-18 There are very few documented cases of intercostal artery laceration during thoracentesis, and they appear to be most commonly reported in the elderly.11 Intercostal artery laceration can also occur during thoracostomy for chest tube insertion,19 and probably in patients with coarctation of the aorta, which leads to engorgement and tortuosity of the intercostal arteries.20 We report a case of an elderly patient who developed a massive hemothorax due to an intercostal artery laceration that occurred despite our following all the recommended thoracentesis procedures. A 78-year-old white man with a history of congestive heart failure secondary to ischemic cardiomyopathy was admitted with generalized weakness and shortness of breath that had worsened during the week prior to admission. He complained of dyspnea on exertion, and orthopnea, and stated that he used 3 pillows during sleep. Chest radiograph on admission showed a large right pleural effusion (Fig. 1). Review of the chest radiograph from 3 months before this presentation showed no pleural effusion. His medical history was notable for diabetes mellitus, anemia secondary to gastrointestinal bleeding, hypothyroidism, hyperlipidemia, coronary artery disease, coronary artery by- Mary L Yacovone MEd RRT is affiliated with the Department of Health Professions, The Bitonte College of Health and Human Services, Youngstown State University, Youngstown, Ohio. Ritha Kartan MD, and Manuel Bautista MD are affiliated with the Department of Internal Medicine, Forum Health, and with Northeastern Ohio Universities Colleges of Medicine and Pharmacy, Youngstown, Ohio. The authors have disclosed no conflicts of interest. Correspondence: Mary L Yacovone MEd RRT, Department of Health Professions, The Bitonte College of Health and Human Services, Youngstown State University, Youngstown OH 44515. E-mail: mlyacovone@ ysu.edu. RESPIRATORY CARE • NOVEMBER 2010 VOL 55 NO 11 Table 1. Complications Following Thoracentesis Complication Occurrence Rate (%) Pneumothorax Re-expansion pulmonary edema Vasovagal reaction Hemothorax Pneumohemothorax Retained intrapulmonary catheter fragments Splenic laceration Abdominal hemorrhage Intercostal artery laceration Pulmonary hemorrhage Subcutaneous implantation of cancer 3–30 0.2–14 ⬍3 ⬍1 ⬍1 ⬍1 ⬍1 ND ND ND ND ND ⫽ no data available, though case reports of these complications suggest that their occurrence rate is ⬍ 1% 1495 INTERCOSTAL ARTERY LACERATION FOLLOWING THORACENTESIS Fig. 1. Admission radiograph shows large right pleural effusion. Fig. 2. Radiograph immediately after thoracentesis is negative for pneumothorax and shows reduced pleural effusion. pass graft of 4 vessels (in 2005), congestive heart failure secondary to ischemic cardiomyopathy, an ejection fraction of 20%, inducible ventricular tachycardia, placement of an implantable cardioverter defibrillator, hypertension, carotid endarterectomy, and prostate cancer with radiation treatment. He was an ex-smoker of 30 pack years. He denied any fever or chills, chest pain, cough, or hemoptysis. His medications on presentation included carvedilol, metformin hydrochloride, enalapril, iron, levothyroxine, atorvastatin, tamsulosin hydrochloride, warfarin, aspirin, and oxygen therapy (4 L/min via nasal cannula). At the time of admission he was afebrile (36.1° C), with blood pressure 135/75 mm Hg, heart rate 78 beats/min, respiratory rate 18 breaths/min, and oxygen saturation 94% while on supplemental oxygen at 4 L/min via nasal cannula. Auscultation revealed normal heart sounds, a grade 3/6 parasternal systolic murmur, bilateral crackles, diminished breath sounds and dullness to percussion on the right side, and decreased tactile fremitus. Abdominal examination found a fluid wave due to ascites. Physical examination was also positive for jugular venous distention and 3⫹ peripheral edema. Both his lower extremities were wrapped for skin erythema and skin breakdown. Pertinent laboratory findings included hemoglobin 8.1 g/L, CO2 content 30 mmol/L, blood urea nitrogen 45 mg/ dL, creatinine 1.5 mg/dL, and INR [prothrombin time international normalized ratio] 4.5. Chest radiograph on his second hospital day revealed an increase in the right effusion. He continued to complain of dyspnea and orthopnea and had failed diuretic therapy. The pulmonary service was consulted for a diagnostic and therapeutic thoracentesis. After evaluation, the pulmonologist agreed to perform a thoracentesis once his INR was less than 2.0, and vitamin K and fresh frozen plasma were administered. On his third hospital day, his INR was 1.6, and, after obtaining informed consent, he underwent right thoracentesis. He was positioned upright and leaning forward throughout the procedure. Once the fluid was located via ultrasound, the skin was prepped and draped with sterile technique. The skin, the superior aspect of the periostium of the eighth rib at the midscapular line, and the parietal pleura were then anesthetized with 1% lidocaine. An 8 French catheter attached to a 50-mL syringe was inserted over the same tract of the superior aspect of the rib, and approximately 1,200 mL of light amber fluid was obtained and sent for analysis. He denied any chest discomfort or pain during or after the procedure. A chest radiograph was obtained immediately after the thoracentesis, and he was closely monitored for changes in vital signs. The pleural fluid analysis revealed pH 7.49, glucose 115 mg/dL, albumin 1.7 g/dL, lactate dehydrogenase 88 g/ dL, and total protein 3.0 g/dL. Total serum protein was 5.7 g/dL, serum albumin was 3.1 g/dL, and serum lactate dehydrogenase was 202 g/dL. The pleural fluid was transudative and secondary to his congestive heart failure. The chest radiograph was negative for pneumothorax and showed a reduction in the pleural effusion (Fig. 2). Approximately 2 hours after the thoracentesis, he complained of chest pain and shortness of breath, and his blood pressure dropped to 80/40 mm Hg. On physical examination he was diaphoretic and his skin was pale. Another chest radiograph revealed a substantial increase in the right pleural opacity (Fig. 3). A hemothorax was immediately suspected, and surgery was consulted for chest tube insertion. He underwent emergency chest tube insertion, which immediately drained a large amount of blood and clots. He was transported to the operating room for exploration and control of bleeding in the right chest cavity. Right antero- 1496 RESPIRATORY CARE • NOVEMBER 2010 VOL 55 NO 11 INTERCOSTAL ARTERY LACERATION FOLLOWING THORACENTESIS Fig. 3. Radiograph approximately 2 hours after thoracentesis shows a right pleural opacity, which was found to be a hemothorax from an intercostal artery laceration during thoracentesis. lateral thoracotomy revealed a right hemothorax full of clots compressing the right lung and mediastinum, and a bleeding intercostal artery. Intraoperatively he received 4 units of packed red blood cells, 3 units of fresh frozen plasma, 1 unit of platelets, and 1,300 mL of crystalloid. Estimated blood loss was 2 L. The intercostal artery was repaired and a second chest tube was inserted. Postoperative hemoglobin was 9.3 g/L and hematocrit was 27.2%. He tolerated the procedure well and was transported in stable condition to the intensive care unit. The following day he was weaned from mechanical ventilation and extubated. Fig. 4. Anatomy of the intercostal rib space. Thoracentesis is a diagnostic and therapeutic procedure that is routinely performed for evaluation of pleural effusion. Clinical judgment determines if the information obtained from pleural fluid analysis is important for diagnostic and therapeutic intervention. The most commonly reported thoracentesis complication is puncture of the visceral pleura, which can cause a pneumothorax. Ultrasound guidance allows the physician to determine a more accurate needle insertion depth into the intercostal space and thus reduces the incidence of pneumothorax.9,21 Evaluation of rib-space width or visualization of arterial blood flow is not determined with the current method of pleural ultrasonography.21,22 Furthermore, ultrasound guidance does not completely replace the physical examination and confirmation of the appropriate site for thoracentesis. In this case thoracentesis was performed in the recommended manner. Ultrasound guidance and chest radiograph were also employed to evaluate the pleural effusion prior to and immediately following the thoracentesis. In retrospect, we believe that the choice of the 8 French catheter may have increased the risk of intercostal artery laceration in this patient. We hypothesize that this patient’s history of coronary artery bypass graft may have produced thoracic anatomical changes. Coronary artery bypass graft can cause rib fractures, abnormal rib cage motion, and pleural fibrosis,23-27 which could increase the risk of intercostal artery laceration. This case emphasizes the importance of understanding the anatomy of the rib cage and the anatomical changes in the elderly. Understanding the rib and intercostal space anatomy is key to choosing the proper thoracentesis technique. Between each rib is the intercostal space, which is largely filled with the external and internal intercostal muscles. Also within the intercostal space and beneath the costal grove of the rib is a neurovascular bundle made of intercostal vein, artery, and nerve. The intercostal arteries lie between the intercostal vein and nerve. Each intercostal artery passes obliquely and laterally to the angle of the superior rib (Fig. 4). The patient is positioned upright and leaning forward to increase the area within the intercostal space. A site midway between the spine and axillary line is selected because the ribs are easily palpated in that location. The needle is inserted 1 to 2 interspaces below the level where the percussion note becomes dull and fremitus is absent. If ultrasound guidance is used, the patient position must be precisely maintained during the thora- RESPIRATORY CARE • NOVEMBER 2010 VOL 55 NO 11 1497 Discussion INTERCOSTAL ARTERY LACERATION FOLLOWING THORACENTESIS centesis. The needle should pass over the superior aspect of the rib to decrease the likelihood of injury to the neurovascular bundle that traverses the inferior rib margin. Increase in tortuosity of intercostal arteries and decrease in the “safe area” (the space between the superior aspect of the lower rib and the lowest point of the intercostal artery) for thoracentesis appear to occur with aging.11 This increases the likelihood of intercostal artery laceration in the elderly, so extreme caution and strict adherence to the recommended thoracentesis techniques are essential. Proper thoracentesis techniques, including physical examination confirmation of appropriate thoracentesis site, correct patient positioning, ultrasound guidance, and close post-thoracentesis monitoring, did not avoid intercostal artery laceration in our patient, but the close monitoring did allow for early diagnosis and treatment. The possibility that catheter diameter and distortion of our patient’s intercostal anatomy may have caused the intercostal artery laceration should also be considered. This case led to a change in catheter selection in our practice. Now we routinely substitute an 18-gauge angiocatheter for the catheter that is currently part of the kit. This case report emphasizes a thoracentesis complication that is more likely in an elderly patient. Although intercostal artery laceration is rare, it should be considered a potential thoracentesis complication, particularly in the elderly. Every attempt should be made to minimize this risk. Close monitoring is necessary, and catheter size should be carefully considered in the planning of thoracentesis in elderly patients. REFERENCES 1. Collins TR, Sahn SA. Thoracentesis. Clinical value, complications, technical problems, and patient experience. Chest 1987;91(6):817822. 2. Seneff MG, Corwin RW, Gold LH, Irwin RS. Complications associated with thoracentesis. Chest 1986;90(1):97-100. 3. Doyle JJ, Hnatiuk OW, Torrington KG, Slade AR, Howard RS. Necessity of routine chest roentgenography after thoracentesis. Ann Intern Med 1996;124(9):816-820. 4. Raptopoulos V, Davis LM, Lee G, Umali C, Lew R, Irwin RS. Factors affecting the development of pneumothorax associated with thoracentesis. AJR Am J Roentgenol 1991;156(5):917-920. 5. Alemán C, Alegre J, Armadans L, Andreu J, Falcó V, Recio J, et al. The value of chest roentgenography in the diagnosis of pneumothorax after thoracentesis. Am J Med 1999;107(4):340-343. 1498 6. Grogan DR, Irwin RS, Channick R, Raptopoulos V, Curley FJ, Bartter T, et al. Complications associated with thoracentesis. Arch Intern Med 1990;150(4):873-877. 7. Colt HG, Brewer N, Barbur E. Evaluation of patient-related and procedure-related factors contributing to pneumothorax following thoracentesis. Chest 1999;116(1):134-138. 8. Mason RJ, Broaddus VC, Murray JF, Nadel JA (editors). Textbook of respiratory medicine, 4th edition, volume 2. Philadelphia: Mosby/ Elsevier/Saunders; 2005:1919. 9. Barnes TW, Morganthaler TI, Olson EJ, Hesley GK, Decker PA. Sonograhically guided thoracentesis and rate of pneumothorax. J Clin Ultrasound 2005;33(9):442-446. 10. Despars JA, Sasson CS, Light RW. Significance of iatrogenic pneumothoraces. Chest 1994;105(4):1147-1150. 11. Carney M, Ravin CE. Intercostal artery laceration during thoracentesis. Chest 1979;75(4):520-522. 12. Feller-Kopman D, Berkowitz D, Boiselle P, Ernst A. Large volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thorac Surg 2007;84(5):1656-1662. 13. Sue DY, Lam K. Retention of catheter fragment after thoracentesis. Postgrad Med 1982;72(1):101-106. 14. Stewart BN, Block AJ. Subcutaneous implantation of cancer following thoracentesis. Chest 1974;66(4):456-457. 15. Heffner JE, Sahn SA. Abdominal hemmorrhage after perforation of diaphragmatic artery during thoracentesis (letter). Arch Intern Med 1981;141(9):1238. 16. Feeney CM, Yoshioka H. A fatal case of pulmonary hemorrhage from thoracentesis (letter). West J Med 1993;158(6):638-639. 17. Sherman S, Nishio JN, Ravikrishnan KP. Massive pulmonary hemorrhage complicating thoracentesis in chronic renal failure (letter). Chest 1979;76(1):118. 18. Vardi M, Dori G, Bitterman H. Large-bore thoracentesis: a case report of a fatal consequence. Eur J Intern Med 2007;18(5):443-444. 19. Urschel JD. Balloon tamponade for hemmorrhage secondary to chest tube insertion. Respir Med 1994;88(7):549-550. 20. Brickner ME, Hillis LD, Lange RA. Congenital heart disease in adults: first of two parts. N Engl J Med 2000;342(4):256-264. 21. Feller-Kopman D. Ultrasound-guided thoracentesis. Chest 2006; 129(6):1709-1714. 22. Mayo PH, Doelken P. Pleural ultrasonography. Clin Chest Med 2006; 27(2):215-227. 23. Greenwald LV, Baisden CE, Panogiotis SN. Rib fractures in coronary bypass patients: radionuclide detection. Radiology 1983;148(2): 553-554. 24. Locke TJ, Griffiths TL, Mould H, Gibson GJ. Rib cage mechanics after median sternotomy. Thorax 1990;45(6):465-468. 25. Kenyon CM, Pedley TJ, Higenbottam TW. Adaptive modeling of the human rib cage in median sternotomy. J Appl Physiol 1991;70(5): 2287-2302. 26. Jantz MA, Veena AB. Pleural fibrosis. Clin Chest Med 2006;27(2): 181-191. 27. Lee GY, Vaz MA, Ely KA, McDonald EC, Thompson PJ, Nesbitt JC, et al. Symptomatic persistent post-coronary artery bypass pleural effusions requiring operative treatment. Chest 2001;119(3):795-800. RESPIRATORY CARE • NOVEMBER 2010 VOL 55 NO 11