Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Early detection of cancer by screening
Riga, 2007
Early detection of cancer by screening
Authors
Solvita Upmale
Gunta Rozentale
Jolanta Skrule
Consultants Pieter Kramers
Ludmila Engele
Iveta Pudule
State Agency “Public Health Agency”, Latvia
State Agency “Public Health Agency”, Latvia
State Agency “Public Health Agency”, Latvia
Expert of the European Commission, the
Netherlands National Institute for Public Health
and the Environment
State Limited Liability Company “Riga Eastern
Hospital”, Latvian Oncology Centre
Health Promotion State Agency, Latvia
The report has been developed within the framework of the EU Transition Facility
Programme 2005 Project “Development of Public Health Monitoring and Reporting
System” No LV/2005-IB/SO/01.
An electronic version of the report is available at the home page of the State Agency
“Public Health Agency” www.sva.gov.lv.
A publication by
State Agency “Public Health Agency”
Klijanu Street 7
Riga, LV-1012
Latvia
All rights reserved © 2007, State Agency “Public Health Agency”, Latvia
CONTENTS
Early Detection of Cancer by Screening
2 of 50
CONTENTS
2
LIST OF FIGURES
4
KEY MESSAGES
6
INTRODUCTION
9
PROBLEM DESCRIPTION
11
GENERAL TRENDS
LEADING CANCERS IN MEN AND WOMEN
CANCERS DETECTABLE BY SCREENING
COMPARATIVE CHARACTERISTICS OF CANCERS DETECTABLE BY SCREENING
11
13
16
26
UNDERLYING CAUSES AND RISK FACTORS
31
POLICY INITIATIVES
34
CONCLUSIONS AND RECOMMENDATIONS
40
CONCLUSIONS
CONCLUSIONS ON SCREENING IMPLEMENTATION IN LATVIA
RECOMMENDATIONS
40
42
43
COMMENTS ON DATA
44
DEFINITIONS
44
ABBREVIATIONS
45
REFERENCES
46
Early Detection of Cancer by Screening
3 of 50
LIST OF FIGURES
FIGURE 1. CANCER INCIDENCE AND MORTALITY (PER 100 000 INHABITANTS)
FIGURE 2. CANCER INCIDENCE IN THE EU COUNTRIES (PER 100 000 INHABITANTS)
FIGURE 3. STANDARDIZED CANCER MORTALITY INDICATORS (PER 100 000 INHABITANTS)
FIGURE 4. INCIDENCE OF LEADING CANCERS IN MEN (PER 100 000 INHABITANTS)
FIGURE 5. MORTALITY FROM LEADING CANCERS IN MEN
FIGURE 6. INCIDENCE OF LEADING CANCERS IN WOMEN (PER 100 000 INHABITANTS)
FIGURE 7. MORTALITY FROM LEADING CANCERS IN WOMEN (PER 100 000 INHABITANTS)
FIGURE 8. PROPORTION OF CANCER INCIDENCE IN I–II AND III–IV STAGES (PERCENTAGE)
FIGURE 9. FIRST-YEAR LETHALITY AND FIVE-YEAR SURVIVAL RATES (PERCENTAGE), ALL
11
12
12
13
14
14
15
15
STAGES
FIGURE 10. PROSTATE CANCER INCIDENCE AND MORTALITY (PER 100
16
000 INHABITANTS) IN
2005
17
FIGURE 11. COLORECTAL CANCER INCIDENCE AND MORTALITY (PER 100 000 INHABITANTS)
18
FIGURE 12. COLORECTAL CANCER INCIDENCE (PER 100 000 INHABITANTS) IN 2005
18
FIGURE 13. COLORECTAL CANCER MORTALITY (PER 100 000 INHABITANTS) IN 2005
19
FIGURE 14. BREAST CANCER INCIDENCE AND MORTALITY (PER 100 000 INHABITANTS)
20
FIGURE 15. BREAST CANCER INCIDENCE AND MORTALITY (PER 100 000 INHABITANTS) IN
2005
20
FIGURE 16. BREAST CANCER INCIDENCE IN THE EU COUNTRIES (PER 100 000 INHABITANTS)
21
FIGURE 17. STANDARDIZED BREAST CANCER INCIDENCE IN THE EU COUNTRIES IN 2002 (PER
100 000 INHABITANTS)
22
FIGURE 18. STANDARDIZED BREAST CANCER MORTALITY INDICATORS (PER 100 000
INHABITANTS)
22
FIGURE 19. CERVICAL CANCER INCIDENCE AND MORTALITY (PER 100 000 INHABITANTS) 23
FIGURE 20. CERVICAL CANCER INCIDENCE IN LATVIA AND RIGA (PER 100 000 INHABITANTS)
23
FIGURE 21. CERVICAL CANCER FIVE-YEAR SURVIVAL RATES (PERCENTAGE)
24
FIGURE 22. CERVICAL CANCER INCIDENCE AND MORTALITY IN 2005 (PER 100 000
INHABITANTS)
25
FIGURE 23. CERVICAL CANCER INCIDENCE IN SOME EU COUNTRIES (PER 100 000
INHABITANTS)
25
FIGURE 24. STANDARDIZED CERVICAL CANCER MORTALITY INDICATORS (PER 100 000
INHABITANTS)
26
FIGURE 25. INCIDENCE OF CANCERS DETECTABLE BY SCREENING (PER 100 000 INHABITANTS)
26
FIGURE 26. MORTALITY FROM CANCERS DETECTABLE BY SCREENING (PER 100 000
INHABITANTS)
27
FIGURE 27. COMPARISON OF MORTALITY AND PYLL INDICATORS FOR CANCERS DETECTABLE
BY SCREENING IN 2005 (PER 100 000 INHABITANTS)
28
FIGURE 28. LATE DIAGNOSIS OF CANCERS DETECTABLE BY SCREENING (III-IV STAGE)
(PERCENTAGE)
28
FIGURE 29. FIVE-YEAR SURVIVAL RATES IN PATIENTS WITH CANCERS DETECTABLE BY
SCREENING IN ALL STAGES (PERCENTAGE)
29
Early Detection of Cancer by Screening
4 of 50
FIGURE 30. LETHALITY DURING THE FIRST YEAR FOLLOWING DIAGNOSIS FOR CANCERS
DETECTABLE BY SCREENING (PERCENTAGE)
30
FIGURE 31. LATE ATTENDANCE OF A PHYSICIAN AS THE MAIN CAUSE FOR LATE DETECTION OF
TIMELY DETECTABLE CANCERS (PERCENTAGE)
30
FIGURE 33. PREVENTIVE EXAMINATIONS — CYTOLOGICAL EXAMINATIONS IN WOMEN
37
Early Detection of Cancer by Screening
5 of 50
Key Messages
KEY MESSAGES
With the ageing of populations, cancer is an increasing problem in
the entire world and also in Latvia.
Mortality due to cancer is the second leading cause of death in
Latvian inhabitants, after cardiovascular diseases (almost 18% of all
deaths), and it shows an increasing trend. Over the past ten years, cancer
mortality in Latvia has increased by 17% and incidence of cancer — by
29%.
Cancer incidence indicators in Latvia are lower compared to other
EU countries, while cancer mortality indicators are higher. This is evidence
of late detection of cancer.
Timely detection is very significant for successful treatment. In
Latvia, almost 60% of cancers are firstly detected at an already advanced
stage (III–IV stage). Late detection increases first-year lethality and
mortality in general and lowers five-year survival rate.
Causes of late detection of cancer include inconsiderate attitude of
inhabitants to their health, low awareness about the necessity of preventive
examinations and symptoms of a disease, as well as insufficient
availability of health care services, especially from the financial point of
view.
As regards cancers from several localizations characterized by high
incidence and mortality, it has been proven that adequate population
screening can provide for a more timely diagnosis and, consequently, a
significantly decreased mortality. In Europe, screening for colorectal,
breast and cervical cancer is proven to be effective. In the case of cervical
and colorectal cancer, the screening allows for the detection of even precancer diseases thus decreasing incidence and mortality.
In women, breast cancer is taking the first place among various
cancer types, for mortality as well as incidence. Over the past ten years,
breast cancer incidence and mortality have shown an increasing trend —
incidence has increased by 23% and mortality – by 15%. Although precancer conditions will not be detected during screening, mammography
provides a possibility to detect breast cancer at early stages and treat it
effectively.
The fourth place in the ranking of cancer mortality is taken by
colorectal cancer. During the past five years, both mortality and incidence
of colorectal cancer have increased. This may be due to the fact that more
Early Detection of Cancer by Screening
6 of 50
Key Messages
than 50% of cases are detected in advanced stages as well as due to
population ageing as the highest incidence and mortality rates are seen at
ages over 60 (80–85% of all cases).
In Latvia, cervical cancer incidence has shown an increase over the
past five years. Since cervical cancer often occurs in women at relatively
young ages, the associated mortality causes a greater loss of potential years
of life than other cancers. During recent years, cervical cancer was first
detected in advanced stages in more than 40% of the cases.
In order to promote early detection of oncological diseases, in 2005
Latvia has launched the facilities for state payment of the following
screening examinations: oncocytological smear from the cervix of uterus,
mammography, and examination of faeces for hidden blood.
According to its organizational principles, the present programme of
preventive examinations in Latvia would be characterized as nonorganized, or opportunity screening. According to the recommendations of
the European Council on cancer screening, this approach is considered
ineffective for early detection, it would not provide improvement in
detection time or survival on a national level, and is therefore not
recommended for the implementation in the member states of the European
Union.
Practical experience with preventive screening in Latvia over the
past two years shows that the number of examinations performed is small
compared to the planned amount and that the funds assigned are not spent.
This is evidence of insufficient participation of the inhabitants in screening
programmes. Possible explanations for that include insufficient capacity of
the health care system, ineffective organization of the screening and the
lack of inhabitants’ awareness on the new facilities.
In order to support the performance of cancer screening in
accordance with best practices, the European Commission has approved
basic guidelines for breast and cervical cancer screening. On this basis,
draft guidelines “National Cancer Control Programme for 2007–2017”
were developed, including proposals for the implementation of an
organized screening in Latvia.
It is common experience in many EU countries that implementation
of a well-designed, comprehensive national cancer control programme,
adjusted to local conditions, can substantially improve the situation in
oncology in a few years' time by decreasing cancer mortality, proportion of
Early Detection of Cancer by Screening
7 of 50
Key Messages
late diagnoses and the general prevalence of cancer, even in circumstances
of limited financial resources.
Early Detection of Cancer by Screening
8 of 50
Introduction
INTRODUCTION
Mortality due to cancer is the second leading cause of death in
Latvian inhabitants, after cardiovascular diseases (almost 18% of all
deaths1), and it shows an increasing trend. Cancer is an important public
health problem despite the recent achievements in medical technology and
pharmacy, and it is also related to considerable health care expenses.
In Latvia, most cancers are firstly detected at already relatively
advanced stages: almost 60% of first diagnoses are made in III–IV stage
(25% – in IV stage). The later the diagnosis, the more limited the treatment
possibilities. Moreover, treatment of late-stage cancer is more expensive
than treatment of cancer at early stages; prognoses of complete recovery
and regaining of capacity for work are small in this case, thereby mortality
is higher too.
Part of cancers, especially breast cancer, cervical cancer and
colorectal (colon and rectum) cancer, can be timely detected using
screening (see Definitions) methods. Timely detection is very important for
a successful treatment of a disease. Many international population
epidemiology studies have concluded that implementation of effective
primary prevention measures and dissemination of information on them to
the population can potentially prevent 26–40% of all cancers2.
In Latvia, breast cancer takes the first place among all malignant
tumours in women, for incidence as well as mortality. Breast cancer is the
leading cause of premature death in women aged 35-64 years, thus
decreasing able-bodied female population.
Presently, almost one third of breast cancers are detected at an
advanced stage (III–IV stage), even though timely detection of breast
cancer within screening programmes with mammography examinations
allows for effective treatment and even recovery.
Cervical cancer detection is often also late (in 2005 — 42.5%), and
the five-year survival rate in case of this cancer has decreased recently (in
2001 — 52.73%, in 2005 — 46.06%). Oncocytological screening for
cervical cancer allows for detection of pre-cancer diseases that can be
treated, thus decreasing cervical cancer incidence and mortality. Latvia,
along with Lithuania, Estonia, Poland and Romania, ranks among the
European states with the highest cervical cancer mortality rates.
Colorectal cancer is one of the leading cancers (according to
mortality rates it occupied the second place in women in 2005 and the
fourth place in men). Both incidence and mortality due to this cancer has
Early Detection of Cancer by Screening
9 of 50
Introduction
increased over the past five years. Late detection of colorectal cancer
occurs in more than a half of patients (in 2005 — 53.2%), thus outpacing
late detection rates for breast and cervical cancer. Also in the case of
colorectal cancer, by detecting pre-cancer conditions or an early stage of
this cancer by screening the treatment is easier and complete recovery rates
are higher.
The aim of the report is to analyze the state of cancer prevalence by
determining factors that have affected late detection of cancer and to
provide recommendations for the improvement of situation in the field of
timely detection of cancer (by screening) in Latvia based upon data
analysis, thereby decreasing the associated mortality.
The report provides an analysis of incidence, survival and mortality
indicators for the following cancers detectable by screening: breast cancer
(in women), cervical cancer and colorectal cancer (further in the text —
cancers detectable by screening). The report will improve awareness of
professionals, decision-makers and the public in this field, thus facilitating
cooperation among various institutions. The analysis included in the report
could support decision-making related to screening of the above-mentioned
cancers, considering also experience of other states in its effective
implementation.
Early Detection of Cancer by Screening
10 of 50
Problem Description
PROBLEM DESCRIPTION
General trends
The oncological situation can be characterized by several indicators,
the most important of them are:
cancer morbidity or incidence,
late detection,
first-year lethality,
five-year survival,
mortality.
These indicators are interconnected: for instance, increase in
incidence that is faster than increase in mortality could be a sign of
improvement of survival rate and decrease of first-year lethality.
Cancer is a problem of increasing importance in the entire world and
also in Latvia: during the time period 1996–2005, incidence of oncological
diseases in Latvia has increased from 337.5 to 433.8 (per 100 000
inhabitants), or by 28.5% during the entire period (~2-2.5% per year). In
absolute numbers these are 8294 firstly diagnosed cancer cases in 1996 and
9935 cases in 2005. As of January 1, 2006, Latvian Cancer Registry
contained 54 549 oncology patients.
Mortality indicators are also alarming, and they have increased by
16.7% over the last ten years in Latvia.
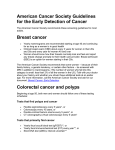
Figure 1. Cancer incidence and mortality (per 100 000 inhabitants)
Per 100 000 inhabitants
(Data of Latvian Cancer Registry)
500
450
400
350
300
250
200
150
100
50
0
Incidence
Mortality
1999
2000
2001
2002
2003
2004
2005
Year
Figure 1 illustrates the increasing trend of incidence and mortality in
Latvia between 1999 and 2005. Both curves show a rather proportional
Early Detection of Cancer by Screening
11 of 50
Problem Description
increase confirming that survival rate has had no explicitly positive
changes during this time period (see also Figure 9).
Cancer incidence indicators in Latvia are lower compared to other
EU countries, while mortality indicators are higher. Low incidence
indicators are more likely indicative of late detection rather than low
incidence level.
Figure 2. Cancer incidence in the EU countries (per 100 000
inhabitants)
(WHO, European health for all database)
Per 100 000 inhabitants
500
Finland
400
EU-15
300
EU
200
Latvia
100
0
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Year
As Figure 2 reflects non-standardized incidence indicators, their
trends may be influenced by age group division of population in each state,
hence also the aging of populations.
Figure 3. Standardized cancer mortality indicators (per 100 000
inhabitants)
Per 100 000 inhabitants
(WHO, European health for all database)
240
220
200
180
160
140
120
100
80
60
40
20
0
Latvia
EU
EU-15
Finland
1996
1997
1998
1999
2000
2001
Year
2002
2003
2004
2005
Analysis of standardized mortality indicators shows that mortality
level in Latvia has no substantial changes. In the EU, and especially EU-15
states (the so-called “old” member states), however, these indicators show
Early Detection of Cancer by Screening
12 of 50
Problem Description
a decrease (the lowest are in Finland), and considering relatively higher
incidence indicators this is an evidence of a more timely detection and
effective treatment (see Figure 3).
Leading cancers in men and women
Figures 4–7 reflect localizations of some of the leading cancers in
men and women in terms of their incidence and mortality.
Lung, prostate and gastrointestinal cancers are the leading types of
cancer among men (Figure 4).
Figure 4. Incidence of leading cancers in men (per 100 000 inhabitants)
(Data of Latvian Cancer Registry)
120
Per 100 000 inhabitants
100
Lung cancer
Prostate cancer
Colorectal cancer
Gastric cancer
Skin cancer (except melanoma)
Urinary bladder cancer
Kidney cancer
Pancreatic cancer
Laryngeal cancer
80
60
40
20
0
1999
2000
2001
2002
2003
2004
2005
Year
Lung, gastric, colorectal and prostate cancers are taking the first
places among cancer types with regard to mortality.
After evaluating Figures 4 and 5, i.e., comparing the ratio between
incidence and mortality for different cancer types, it can be concluded that
lung, gastric and colorectal cancers have higher lethality, while prostate
and skin cancers have a comparatively low lethality level.
Early Detection of Cancer by Screening
13 of 50
Problem Description
Figure 5. Mortality from leading cancers in men
(Data of Latvian Cancer Registry)
120
Lung cancer
100
Per 100 000 inhabitants
Gastric cancer
Colorectal cancer
80
Prostate cancer
60
Pancreatic cancer
Urinary bladder cancer
40
Kidney cancer
20
Laryngeal cancer
Skin cancer (except melanoma)
0
1999
2000
2001
2002
2003
2004
2005
Gads
Breast and colorectal cancers as well as skin cancer are the most
widespread types of cancer in women (see Figure 6 and 7); however,
cancers of reproductive organs (uterus, cervix and ovaries) occupy
comparatively high positions as well. Evaluation of incidence indicators
provides an indication of this.
Figure 6. Incidence of leading cancers in women (per 100 000
inhabitants)
(Data of Latvian Cancer Registry)
120
Breast cancer
Colorectal cancer
Per 100 000 inhabitants
100
Skin cancer (except melanoma)
80
Uterine cancer
Gastric cancer
60
Ovarian cancer
40
Cervical cancer
Lung cancer
20
Kidney cancer
0
Pancreatic cancer
1999
2000
2001
2002
2003
2004
2005
Year
Also in cancer mortality patterns in women, the first places are taken
by breast and colorectal cancers, followed by gastric and lung cancer (these
indicators have increased recently); high places are taken also by cancers
of reproductive organs.
Early Detection of Cancer by Screening
14 of 50
Problem Description
Figure 7. Mortality from leading cancers in women (per 100 000
inhabitants)
(Data of Latvian Cancer Registry)
40
Breast cancer
Colorectal cancer
Gastric cancer
Ovarian cancer
Lung cancer
Pancreatic cancer
Uterine cancer
Cervical cancer
Kidney cancer
Urinary bladder cancer
Skin cancer (except melanoma)
Per 100 000 inhabitants
35
30
25
20
15
10
5
0
1999
2000
2001
2002
2003
2004
2005
Year
Following evaluation of the ratio between incidence and mortality, it
can be concluded that lethality in the case of colorectal cancer is noticeably
higher than, for instance, breast cancer or skin cancer lethality.
If increase in incidence in some cases could be evaluated positively
(for instance, if diagnostics has improved), then simultaneous increase in
mortality indicators of several cancer types such as lung, colorectal, breast
and prostate cancer (see Figures 4–7) clearly points to a necessity of
making an immediate evaluation of its causes. One of the most significant
causes of mortality increase is late detection.
If cancer is detected at an advanced stage (III–IV stage), prognoses
and survival possibilities are much lower than if cancer is detected at I–II
stage; moreover, in such case a more complicated treatment and more
financial investments are needed.
Figure 8. Proportion of cancer incidence in I–II and III–IV stages
(percentage)
(Data of Latvian Cancer Registry)
70
Percentage
60
III-IV and an
unknown stage
I-II stage
50
40
30
20
10
0
1999
2000
2001
2002
2003
2004
2005
Year
Early Detection of Cancer by Screening
15 of 50
Problem Description
As it can be seen from Figure 8, in Latvia almost 60% of first
diagnoses are belated — in III and IV stage (~25% — in IV stage).
Analysis of indicators in dynamics (Figure 8) shows slight
improvement of the situation as evidenced by a slight increase in the fiveyear survival rates and a decrease in first-year lethality (Figure 9).
Figure 9. First-year lethality and five-year survival rates (percentage),
all stages
(Data of Latvian Cancer Registry)
50
Five-year survival
Percentage
45
40
35
Lethality during the first
year of diagnosis
30
25
20
1999
2000
2001
2002
2003
2004
2005
Year
Despite the noticeable slight improvement trends, first-year lethality
is very high and five-year survival is low compared to the indicators of the
EU-15 states. There is an increase in five-year survival rates; still this
indicator does not exceed 45%3.
Decrease in lethality during the first year following diagnosis should
be positively evaluated.
Cancers detectable by screening
As regards cancers from several localizations characterized by high
incidence and mortality, it has been proven that adequate population
screening can provide for a more timely diagnosis and, consequently, a
significantly decreased mortality. In Europe, screening for colorectal,
breast and cervical cancer has proven to be effective4.
In order to timely detect breast and cervical cancer, and prostate and
colorectal cancer, in 2005 Latvia has launched facilities for state payment
of screening examinations.
However, the oncology specialists have given up the prostate
screening, and as of January 1, 2007 preventive examinations for this
cancer type are not covered by the state, because its impact on mortality
reduction is not cogent and it does not correspond to the screening criteria
posed by the WHO5. Figure 10 shows incidence and mortality indicators
Early Detection of Cancer by Screening
16 of 50
Problem Description
for this cancer type in 2005. Although this cancer type may be detected
early, it is not cost-effective (too expensive); in addition, more than a half
of patients are over 70 years of age and the disease has a relatively slow
progress.
Figure 10. Prostate cancer incidence and mortality (per 100 000
inhabitants) in 2005
(Data of Latvian Cancer Registry)
Per 100 000 inhabitants
800
700
600
Incidence
500
400
300
Mortality
200
100
0
35 - 39 40 - 44 45 - 49 50 - 54 55 - 59 60 - 64 65 - 69 70 - 74 75 - 79 80 - 84 85 and
older
Year
In view of that, the following sections of the report will be dedicated
to a more detailed analysis of the above-mentioned three cancer types:
colorectal, breast (in women, also further in the text) and cervical cancer.
Colorectal cancer
Colorectal cancer is one of the most frequently detected cancers in
men and in women (especially after the age of 60).
As in most cases colorectal cancer develops from polyps (by
malingnization), timely detection and elimination of polyps as well as
detection of pre-cancer conditions or colorectal cancer at an early stage by
screening will allow for an easier treatment of the disease and often even a
complete recovery.
If these cancer types are detected in advanced stages, survival rate
will be low, for instance, in IV stage it does not reach even 10% (see
Figure 7 in the Annex).
Figure 11 shows incidence and mortality trends of colorectal cancer.
Colorectal cancer incidence shows a statistically valid increasing
trend that could be evaluated positively only in case of a timely diagnosis
(increased number of cancers detected at an early stage). Increasing
mortality, however, attests to late detection and is facilitated by the ageing
of the population.
Early Detection of Cancer by Screening
17 of 50
Problem Description
Figure 11. Colorectal cancer incidence and mortality (per 100 000
inhabitants)
(Data of Latvian Cancer Registry)
Per 100 000 inhabitants
50
40
Incidence
y = 1,6607x + 35,414
R2 = 0,832
Mortality
30
Linear
(Incidence)
20
10
0
1999
2000
2001
2002
Year
2003
2004
2005
Incidence (per 100 000 inhabitants) is on average 1.4 times higher
than mortality (per 100 000 inhabitants), still in different age groups this
ratio is different.
There has been a more rapid increase in mortality from colorectal
cancer recently (in 2005, compared to 2002, it has increased by 21%). This
could be related to the ageing of population. Most of incidence and
mortality cases (80–85%) occur in the age group over 60.
Figure 12. Colorectal cancer incidence (per 100 000 inhabitants) in
2005
(Data of Latvian Cancer Registry)
400
Per 100 000 inhabitants
350
300
Men
250
200
150
Women
100
50
0
35 - 39 40 - 44 45 - 49 50 - 54 55 - 59 60 - 64 65 - 69 70 - 74 75 - 79 80 - 84
85 and
older
Year
Incidence indicators after 60 are noticeably higher both in men and
in women. It should be noted that these indicators are almost five times
higher in men (see Figure 12).
Recently, colorectal cancer mortality among men occupied 2nd–4th
place (see Figure 5). This, however, is related to age structure — most
patients are aged over 70, and diagnostics is late in nearly 60% of cases.
Early Detection of Cancer by Screening
18 of 50
Problem Description
Colorectal cancer incidence and mortality in women is increasing
after 60 as well.
Figure 13 shows that mortality indicators in men are 1.5–2 times
higher than in women; moreover, this increase is seen in almost all age
groups.
Figure 13. Colorectal cancer mortality (per 100 000 inhabitants) in
2005
Per 100 000 inhabitants
(Data of Latvian Cancer Registry)
500
450
400
350
300
250
200
150
100
50
0
Men
Women
35 - 39 40 - 44 45 - 49 50 - 54 55 - 59 60 - 64 65 - 69 70 - 74 75 - 79 80 - 84 85 and
older
Year
Even though high mortality, compared to incidence, attests to low
survival, it also shows a noticeable potential for the improvement of this
indicator.
Breast cancer (in women)
Breast cancer in women occupies the first place in the patterns of
cancer incidence and mortality. In 2005, almost every fifth woman with a
cancer diagnosis had breast cancer. 16% of all women who died of cancer
had breast cancer.
Breast cancer incidence (per 100 000 inhabitants) and mortality (per
100 000 inhabitants) in dynamics shows an increasing trend. During the
last ten years, incidence has increased by 23% and mortality — by 15%
(Figure 14).
Increase in incidence should be evaluated positively only in case of a
timely diagnosis (increased number of cancers detected at an early stage),
however, as in Latvia one third of cases of breast cancer is detected in
advanced stages (in III–IV stage), the increasing incidence points to the
high breast cancer prevalence (see Figure 28).
Early Detection of Cancer by Screening
19 of 50
Problem Description
Figure 14. Breast cancer incidence and mortality (per 100 000
inhabitants)
(Data of Latvian Cancer Registry)
90
Per 100 000 inhabitants
80
Incidence
70
60
50
40
Mortality
30
20
10
0
1999
2000
2001
2002
2003
2004
2005
Year
In Latvia, like everywhere else in the world, increase in cancer
incidence and mortality is partially facilitated by the ageing of populations.
In Figure 15 these indicators are shown in distribution by different age
groups.
Figure 15. Breast cancer incidence and mortality (per 100 000
inhabitants) in 2005
Per 100 000 inhabitants
(Data of Latvian Cancer Registry)
200
180
160
140
120
100
80
60
40
20
0
Incidence
Mortality
25 - 29 30 - 34 35 - 39 40 - 44 45 - 49 50 - 54 55 - 59 60 - 64 65 - 69 70 - 74 75 - 79 80 - 84 85 and
older
Age (years)
The highest breast cancer incidence is in the age group over 50. This
is one of the reasons for performing screening examinations with
mammography in women after 50 years of age.
In accordance with WHO data, performance of mammography tests
(used in screening) can decrease breast cancer mortality of women aged
50-69 even by 35%6. Unfortunately, in Latvia mortality due to breast
cancer has increased in young women (age group 30-34) recently.
Early Detection of Cancer by Screening
20 of 50
Problem Description
Figures 16–18 reflect the situation in the EU Member States. Most
countries have an increasing breast cancer incidence (per 100 000
inhabitants). This could be an evidence of a timely detection and a stable
breast cancer mortality level (per 100 000 inhabitants), showing even a
decreasing trend in some places.
Figure 16. Breast cancer incidence in the EU countries (per 100 000
inhabitants)
(WHO, European health for all database)
160
The
Netherlands
Finland
Per 100 000 inhabitants
140
120
100
Estonia
80
Latvia
60
Lithuania
40
Romania
20
0
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Year
Breast cancer incidence indicators in Latvia, similarly to other new
EU Member States having joined the EU between 2004 and 2007, are
lower than in the 15 developed or the so-called “old” member states of the
European Union (see Figure 16). It should be noted that these data are not
standardized; therefore they are influenced by the population age structure
in each state.
After comparing the standardized incidence indicators (per 100 000
inhabitants), breast cancer incidence in Latvia is seen to be noticeably
lower than in other European states (see Figure 17).
In general, the data show that in the so-called “old” member states of
the EU breast cancer incidence indicators are higher than in the “new”
member states. High incidence indicators may possibly be explained by
good diagnostic possibilities and performance of screening. In this case,
low incidence indicators in Latvia do not attest to low breast cancer
prevalence, but to a relatively high proportion of undetected cases.
Early Detection of Cancer by Screening
21 of 50
Problem Description
Figure 17. Standardized breast cancer incidence in the EU countries in
2002 (per 100 000 inhabitants)
(Eurostat data)
Lithuania
Latvia
Romania
Bulgaria
Estonia
Poland
Czech Republic
Hungary
Finland
Great Britain
Sweden
Denmark
0
10
20
30
40
50
60
70
80
90
100
Per 100 000 inhabitants
Standardized mortality at all ages in Latvia is slightly lower than the
average in the EU-27 (see Figure 18).
Figure 18. Standardized breast cancer mortality indicators (per
100 000 inhabitants)
(WHO, European health for all database)
35
EU-15
Per 100 000 inhabitants
30
25
EU
20
Latvia
15
10
Finland
5
0
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Year
Yet, indicators of premature (at the age 0–64) standardized mortality
(per 100 000 inhabitants) in Latvia are among the highest in the EU-27
states. This situation should be evaluated negatively as it attests to the fact
that women die of breast cancer at a relatively earlier age than on average
in the EU, consequently, causing increase in PYLL rates related to breast
cancer (see Figure 9 in the Annex).
Early Detection of Cancer by Screening
22 of 50
Problem Description
Cervical cancer
In 2005, almost ten women died of cervical cancer each month. This
cancer is one of the cancer types affecting women at an earlier age than
cancers of other localizations, and it is preventable by timely detection of
pre-cancer diseases. In Latvia, cervical cancer incidence is having an
increasing trend during the last five years.
Figure 19. Cervical cancer incidence and mortality (per 100 000
inhabitants)
Per 100 000 inhabitants
(Data of Latvian Cancer Registry)
20
18
16
14
12
10
8
6
4
2
0
Incidence
Mortality
1999
2000
2001
2002
2003
2004
2005
Year
Increase in cervical cancer incidence should be negatively evaluated,
because with timely treatment of pre-cancer diseases, which may be
detected in oncocytological smears from the cervix (performed within the
screening), development of this cancer type may be prevented. Cervical
cancer mortality has remained at almost the same level during the last ten
years.
Figure 20. Cervical cancer incidence in Latvia and Riga (per 100 000
inhabitants)
Per 100 000 inhabitants
(Data of Latvian Cancer Registry)
20
19
18
17
16
15
14
13
12
11
10
Latvia except
Riga
Riga
1999
2000
2001
2002
2003
2004
2005
Year
Early Detection of Cancer by Screening
23 of 50
Problem Description
There are differences in cervical cancer incidence indicators (per
100 000 inhabitants) in Riga and the rest of Latvia (excluding Riga). Low
incidence and its decrease in Riga recently may attest to timely detection
and treatment of pre-cancer diseases, thereby decreasing cervical cancer
incidence. This could be explained by the raising of women’s awareness
and informedness and, possibly, by increased availability of health care
services (gynaecologist, examinations). Accordingly, this is an evidence of
a more negative situation outside the capital.
In general, stability of cervical cancer mortality in Latvia is a
negative trend. One fourth of women have died of cervical cancer already
during the first year after cancer diagnosis (see Figure 30). This cancer
incidence and mortality could be prevented by timely detection of precancer diseases within screening.
High mortality and lethality is facilitated by the fact that often (in
more than 40% cases) cancer is detected only at advanced stages (III-IV
stage) (see Figure 28), when the chances for positive treatment results are
small.
Figure 21. Cervical cancer five-year survival rates (percentage)
(Data of Latvian Cancer Registry)
100
I stage
Percentage
80
60
II stage
40
III stage
20
IV stage
0
1999
2000
2001
2002
2003
2004
2005
Year
If cervical cancer is diagnosed in IV stage, first-year lethality
reaches 80%. Consequently, five-year survival in IV stage was only 4.5%
in 2005. On the contrary, if cervical cancer is diagnosed in I stage, fiveyear survival reaches about 90% (see Figure 21).
Nearly half of women with cervical cancer are aged under 60.
Mortality indicators, compared with incidence, by the age of 60 are almost
two times lower; however, with age increasing the difference disappears
and mortality even surpasses incidence. This could be explained by the fact
that younger women attend the physician and perform tests more often.
Although this allows cervical cancer to be detected earlier, 35-43% of
women who died of this cancer were aged under 60.
Early Detection of Cancer by Screening
24 of 50
Problem Description
Figure 22. Cervical cancer incidence and mortality in 2005 (per
100 000 inhabitants)
(Data of Latvian Cancer Registry)
Per 100 000 inhabitants
40
35
Incidence
30
25
Mortality
20
15
10
5
0
25 - 29 30 - 34 35 - 39 40 - 44 45 - 49 50 - 54 55 - 59 60 - 64 65 - 69 70 - 74 75 - 79 80 - 84 85 and
older
Year
In comparison with other EU states, cervical cancer incidence rates
in Latvia (per 100 000 inhabitants), as well as in other “new” member
states, are higher than in the “old” member states, and even show an
increasing trend. This could possibly attest to late cancer detection and,
accordingly, belated treatment of pre-cancer diseases. It should be noted
that these data are not standardized; therefore they are influenced by the
population age structure in each state.
Figure 23. Cervical cancer incidence in some EU countries (per
100 000 inhabitants)
(WHO, European health for all database)
Per 100 000 inhabitants
35
30
Lithuania
25
Estonia
20
Latvia
15
Finland
10
5
0
1996
1997
1998
1999
2000 2001
Year
2002
2003
2004
2005
Figure 24 reflects standardized cervical cancer mortality indicators
in the EU states. Standardized mortality indicators in Latvia, like in
Lithuania and Estonia, are noticeably higher than the average in the EU-27.
Early Detection of Cancer by Screening
25 of 50
Problem Description
Figure 24. Standardized cervical cancer mortality indicators (per
100 000 inhabitants)
(WHO, European health for all database)
14
Per 100 000 inhabitants
12
10
Lithuani
a
Estonia
8
6
4
Latvia
2
EU
0
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Year
EU-15
Finland
Even a greater difference is seen between the Baltic States and the
EU-15, or the so-called “old” member states, many of which have reached
a relatively low cervical cancer mortality level, for instance, Finland.
Similar situation is also reflected by the standardized mortality indicators
at the age under 64.
Comparative characteristics of cancers detectable by screening
Figure 25. Incidence of cancers detectable by screening (per 100 000
inhabitants)
Per 100 000 inhabitants
(Data of Latvian Cancer Registry)
90
80
70
60
50
40
30
20
10
0
Breast cancer
Colorectal cancer
Cervical cancer
1999
2000
2001
2002
2003
2004
2005
Year
Comparison of incidence indicators (per 100 000 inhabitants) for
cancers detectable by screening reveals that breast cancer has the highest
incidence (see Figure 25). Accordingly, breast cancer has the smallest
(compared with the other two cancer localizations) proportion of late
detection (at III-IV stage) and first-year lethality (see Figures 28 and 30).
Early Detection of Cancer by Screening
26 of 50
Problem Description
Nevertheless, breast cancer remains to be the leading cause of death among
cancers in women.
Increasing breast cancer mortality (see Figure 26) is indicative of
high breast cancer prevalence.
Figure 26. Mortality from cancers detectable by screening (per 100 000
inhabitants)
(Data of Latvian Cancer Registry)
Per 100 000 inhabitants
40
35
Breast cancer
30
25
Colorectal cancer
20
15
10
Cervical cancer
5
0
1999
2000
2001
2002
Year
2003
2004
2005
Mortality indicators (per 100 000 inhabitants) can be characterized
similarly to incidence indicators: breast cancer is the leading type of cancer
in terms of mortality, and breast and colorectal cancer mortality shows an
increasing trend.
High mortality is explained by low survival rate. If these cancers are
detected in advanced stages, for instance, in IV stage, this rate hardly
reaches 10%. The increasing trend is also influenced by the ageing of
population, especially in the case of colorectal cancer, because it is often
detected in inhabitants aged over 60.
Comparison of mortality and PYLL indicators (per 100 000
inhabitants) for cancers detectable by screening shows that breast cancer
takes the first place, and PYLL indicator for colorectal cancer, despite the
high mortality, is lower than for cervical cancer, which has three times
lower mortality.
Figure 27 once again emphasizes the relation between mortality
indicators and age structure (ageing of population increases the number of
deaths). Cervical cancer affects younger women, causing the loss of many
potential years of life (before the age of 65), and, contrary to mortality rate,
PYLL indicator remains high. In most cases, deaths due to colorectal
cancer occur in people after 60 years of age; therefore PYLL indicator is
lower as opposed to a higher mortality rate.
Early Detection of Cancer by Screening
27 of 50
Problem Description
Figure 27. Comparison of mortality and PYLL indicators for cancers
detectable by screening in 2005 (per 100 000 inhabitants)
(Data from Latvian Cancer Registry and PHA)
250
35
Mortality
30
PYLL
200
25
150
20
100
15
10
PYLL
Mortality
40
50
5
0
0
Breast cancer
Colorectal cancer
Cervical cancer
In the next figure, comparison of proportion of late diagnoses for all
the three cancer types is made.
Figure 28. Late diagnosis of cancers detectable by screening (III-IV
stage) (percentage)
(Data of Latvian Cancer Registry)
70
60
Percentage
Colorectal cancer
50
Cervical cancer
40
Breast cancer
30
20
10
1999
2000
2001
2002
2003
2004
2005
Year
Colorectal cancer is detected at advanced stages in more than half of
patients (see Figure 28), which ranks it in the stable 4th place in the cancer
mortality structure during last ten years: in men — 2nd–4th place (see
Figure 5), in women — 2nd place (see Figure 7).
During the last ten years, cervical cancer has been detected at
advanced stages in more than 40% of women, and only one third of women
have a five-year survival rate from this cancer in III-IV stage. Thus, timely
detection or screening of this cancer type should be emphasized once
again.
Early Detection of Cancer by Screening
28 of 50
Problem Description
The studies have proven that by implementing organized screening
programmes, i.e., by improving detection survival rates may be increased,
and lethality and mortality decreased7;8. For instance, in states where
organized screening is being implemented for several years, five-year
survival rates are higher than in states where the screening is not
implemented and reach 80% (Finland, Sweden) for breast cancer and 70 %
for cervical cancer (Finland, the Netherlands, Norway)9.
Figure 29. Five-year survival rates in patients with cancers detectable
by screening in all stages (percentage)
(Data of Latvian Cancer Registry)
90
Percentage
70
Breast cancer
Cervical cancer
50
Colorectal cancer
30
10
1999
2000
2001
2002
2003
2004
2005
Year
In comparison with indicators of other European states, Latvia has a
low five-year survival rate in patients with cancers detectable by screening.
This indicator is influenced by the high proportion of late diagnoses
of cancer. Five-year survival rate for breast cancer in IV stage does not
reach even 15%, for cervical and colorectal cancer — almost 5% (see
Figure 8 in the Annex).
According to the data obtained from HCISA, treatment expenses for
breast and cervical cancer due to late detection are 2–10 times higher than
in the case of timely treatment.
The high proportion of late diagnoses affects not only survival rates
but also first-year lethality indicators.
As it can be seen in Figure 30, first-year lethality due to colorectal
cancer is the highest and survival is the lowest (of the three cancers
detectable by screening), because this cancer type has the highest
proportion of late diagnoses (see Figure 28). Cervical cancer takes the
second place according to these indicators.
Early Detection of Cancer by Screening
29 of 50
Problem Description
Figure 30. Lethality during the first year following diagnosis for
cancers detectable by screening (percentage)
Percentage
(Data of Latvian Cancer Registry)
50
45
40
35
30
25
20
15
10
5
0
Colorectal cancer
Cervical cancer
Breast cancer in
women
1999
2000
2001
2002
2003
2004
2005
Year
The cause for late detection of cervical cancer in more than 80%
cases is belated attendance of a physician.
Figure 31. Late attendance of a physician as the main cause for late
detection of timely detectable cancers (percentage)
(LOC data – Report 2005)
90
Cervical
cancer
80
Percentage
70
Breast
cancer
60
50
40
Rectal
cancer
30
20
10
0
2002
2003
2004
2005
Year
Situation illustrated by Figure 30 specifically points to the necessity
of inviting women to visit a physician in a timely manner as, for instance,
cervical cancer can be prevented by timely detection of pre-cancer
illnesses.
Early Detection of Cancer by Screening
30 of 50
Underlying Causes and Risk Factors
UNDERLYING CAUSES AND RISK FACTORS
Oncological morbidity depends on a number of factors, including
social, economic, geographical and demographic, which, in their turn, are
closely connected with quality and availability of health care services at all
levels as well as efficiency of health promotion measures.
All the three cancers analyzed in this report have a complex
aetiology: they share a number of risk factors (genetic factors, age,
unhealthy sustenance, lack of physical training, overweight, smoking).
Each of them, however, also has some specific risk factors:
Breast cancer: menopause, hormonal contraception, late first
delivery.
Colorectal cancer: chronic inflammations, intestinal polyps.
Cervical cancer: pre-cancer cervical diseases, mainly caused by
human papilloma virus.
The aim of this report is to emphasize the importance of early
detection and screening in decreasing mortality from cancer, therefore
biological risk factors and their role will not be described in detail in the
report.
As late detection is one of the most substantial problems influencing
mortality increase and making Latvia’s indicators differ from the average
EU indicators, it is necessary to study and eliminate its underlying causes.
In more than a half of cases the cause for late detection is late
attendance of a physician. This could be possibly influenced by a negligent
attitude towards health, lack of information and understanding of the
necessity of preventive examinations and symptoms of a disease10.
One of the causes for late detection of oncological diseases is
insufficient availability of health care services.
Many recent studies have stressed that inhabitants rate the
availability of health care services as poor, especially from the financial
point of view11. In accordance with WHO data, Latvia has one of the
highest patient co-payments in Europe. In addition, the amount of copayment is not proportionate to person’s income; as a result, co-payments
substantially restrict the availability of health care services for low-income
inhabitants12.
The implication of limited financial availability is also revealed by
the results of the study "Availability of health care services in Riga and
Early Detection of Cancer by Screening
31 of 50
Underlying Causes and Risk Factors
Vidzeme" performed by Latvia University13. The study analyzed the
following availability problems: geographic availability, especially in rural
areas (distance to health care facilities, provision of public transport), as
well organizational availability (consultation hours of physicians, long
time waiting, unsuitable visiting hours).
Also, many inhabitants are not informed about the state-paid
prevention and screening programmes. General practitioners often do not
inform patients, for instance, on the possibility of attending a gynaecologist
free of charge once a year.
The problem of health care availability, compared with other EU
states, is revealed also by EU-SILC study ("Survey on Income and Living
Conditions"). It has analyzed the following aspects of health care service
availability: health care coverage, expenses, geographical availability,
queues, lack of information.
Figure 32. Reasons for limited availability of medical examinations14
Reasons for limited availability of medical examinations
20
18
16
14
12
10
8
6
4
2
0
AT
BE
CY
CZ
DE
DK
EE
ES
FI
FR
GR
HU
IE
IS
IT
LT
LU
LV
MT
NL
NO
PL
PT
SE
could not afford (1) waiting (2) too far (4)
As it can be seen in Figure 32 (data for 2005), Latvia has the greatest
proportion of inhabitants among the EU states who were forced to refuse
medical aid. Proportion of inhabitants who responded that they could not
afford the relevant medical examination because of limited financial
availability is especially high. Reasons mentioned by Latvian inhabitants
were divided as follows: slightly more than 16% of the population cannot
Early Detection of Cancer by Screening
32 of 50
SK
UK
Underlying Causes and Risk Factors
afford medical examinations financially; almost 2% — due to waiting lists
(queues), and a very small part (~0.5%) mentioned too long a distance or
inconveniences in reaching the place where health tests could be performed
or medical aid could be received (transport). Another reason that was
mentioned was a wish to wait and see whether their condition improves in
the course of time, which attests to a rather negligent attitude towards
one’s health.
The summarized data of the study show a close relation between the
income level and the ability to cover expenses for consultations with a
medical specialist or medical aid. In other words, low-income households
are to a greater extent subject to the risk of non-obtaining the necessary
medical aid. At the same time, as income level increases, the proportion of
reasons of non-attendance related to the lack of time also increases.
As the problem of cancer becomes most urgent at the age over 50,
and the income level of inhabitants of this age is relatively low, limited
financial availability is a substantial reason for late attendance of a
physician.
Early Detection of Cancer by Screening
33 of 50
Policy Initiatives
POLICY INITIATIVES
Several policy planning documents providing for the improvement
of the health status of Latvian inhabitants, inter alia with regard to
problems related to oncological diseases, have been developed in the state.
One of the most important documents in the field of public health is Public
Health Strategy approved by the Cabinet of Ministers on March 6, 2001.
One of its objectives is to decrease the prevalence of noncommunicable
diseases and to achieve a decrease in disability and premature mortality
caused by the most widespread noncommunicable diseases in Latvia to the
lowest possible level by 2010.
Other policy planning documents address the issues of oncology
from the health care point of view. For instance, in order to ensure the
quality, availability and rational use of resources of health care services,
including oncological health care services, the following programmes have
been developed:
Development Programme for Ambulatory and Hospital Health
Care Service Providers (approved by the Order of the Cabinet of
Ministers No. 1003 of 20.12.2004.), stipulating the planned number and
location of medical treatment institutions;
Basic Guidelines for Human Resources Development in Health
Care (approved by the Order of the Cabinet of Ministers No. 326 of
18.05.2005.) and programme “Human Resources Development in
Health Care 2006–2015” (approved by the Order of the Cabinet of
Ministers No. 870 of 06.11.2006.).
One of the main steps towards improving early detection of
oncological diseases is a programme of free preventive examinations for
risk groups launched on April 1, 2005: Regulations of the Cabinet of
Ministers No. 1036 of 21.12.2004 “Procedure for organization and
financing of health care” and Annex 5 “Programme of preventive
examinations” of Regulations of the Cabinet of Ministers No. 1046 of
19.12.2006 “Procedure for organization and financing of health care”,
which provides for examinations included in cancer screening:
cervical cancer detection with oncocytological smear from the cervix
of uterus in women aged 25-70 once in three years,
examination of faeces for hidden blood once a year for persons over
50,
breast cancer screening with mammography in women aged 50-69
once in two years.
Early Detection of Cancer by Screening
34 of 50
Policy Initiatives
Also international documents have been developed in the field of
cancer.
In 2006, the European Commission published the 4 th edition of
European guidelines for quality assurance in breast cancer screening and
diagnosis, and approved the guidelines issued by the World Health
Organization for organization of cervical cancer screening. On the basis of
the above-mentioned guidelines, a draft guideline “National cancer control
programme for 2007–2017” was developed in Latvia, stipulating planned
development directions in the field of oncology in Latvia, including
proposals for the implementation of organized screening.
Practical screening implementation in Latvia
According to its organizational principles, the present programme of
preventive examinations in Latvia would be characterized as nonorganized, or opportunity screening (other names: decentralized, ondemand screening). In accordance with the European Council
recommendations on cancer screening, this approach is considered
ineffective for early detection; it does not provide for the improvement in
detection time and mortality indicators on a national level and is not
recommended for the implementation in the EU Member States15.
In Latvia, implementation of opportunity screening is delegated to
general practitioners (a single payment is made for each preventive
examination and for each patient who has received preventive examination
after referral from the general practitioner). The experience gained during
the past years shows that financial motivation of general practitioners alone
without the change of organizational principles will not ensure the
expected results (coverage of at least 15%), because response of
inhabitants to screening activities is very low according to information
obtained from HCISA (see the Table below)16.
Table 1. Indicators of screening examination coverage in 2005 and
2006
Type
manipulations
of Amount of Actual
Amount
of Actual
manipulati coverage (%) manipulation coverage (%)
ons in 2005 in 2006
s in 2006
in 2006
Mammography as part of
health
prevention
examinations
8066
Early Detection of Cancer by Screening
2.6%
16616
5.41%
35 of 50
Policy Initiatives
Cervical cancer screening
(in the age group 20-35);
(in the age group 36-70)
77379
Prostate cancer screening
Colorectal
cancer
screening
2942
5033
9.52%
8.62%
36656
78612
10.04%
10.42%
1.2%
0.6%
5709
9937
2.75%
1.21%
In analysing the two-year screening in Latvia, attention should be
paid to the low proportion of examinations (see Table 1). This clearly
attests to insufficient involvement of inhabitants in screening programmes.
Moreover, in accordance with HCISA data, in 2006 only 23% of funds
assigned for preventive examinations were spent.
After analysis of the amount of performed mammographies it has
been concluded that a number of health care facilities offer a very small
amount of services, which according to the EU guidelines17 is not
acceptable to the providers of screening services. Also, the provision of
mammography equipment and the equipment itself is not fully adequate
and sufficient (over the last ten years the number of mammographs has not
significantly changed, in 2005 there were 33 mammographs, half of them
in Riga, but there are regions where such equipment is not available).
None of the medical treatment institutions in Latvia performs double
reading of mammograms, which is advisable for centralized screening and
compulsory under circumstances of decentralized or opportunity screening,
which is carried out in Latvia).
Coverage of oncocytological screening or equal examinations may
be slightly greater, because HCISA does not receive information on
patients and manipulations performed by gynaecologists in private offices
and paid by inhabitants themselves; however, the stable rates of late
primary diagnosis of cancer (see Figure 28) attest to absolutely insufficient
coverage of inhabitants.
Figure 33 illustrates the relation between the proportion of women
who have passed cytological examination and proportion of lately
diagnosed cervical cancer.
Early Detection of Cancer by Screening
36 of 50
Policy Initiatives
Figure 33. Preventive examinations — cytological examinations in
women
Percentage
(LOC data – Report 2005)
55
50
45
40
35
30
25
20
15
10
5
0
Cervical cancer in IIIIV stage
Proportion of women
having performed
cytological examination
1996
1997
1998
1999
2000
2001
Year
2002
2003
2004
2005
Cervical cancer
detected in preventive
examinations
The figure shows that with the increase of proportion of women who
have performed cytological examinations in late 90s, the proportion of late
detection of cervical cancer has decreased. Since 2001, as the proportion of
women who have performed cytological examinations has decreased, the
proportion of late detection of cervical cancer has increased. These
changes may be possibly affected by the reforms of health care
organization.
Involvement or non-involvement of inhabitants in screening largely
depends on individual awareness and initiative, as well as the availability
of services and other aspects. For instance, screening examination is often
available only as paid service.
The small number of gynaecologists who have concluded a contract
with HCISA and provide state-paid services also provides an indication of
limited availability. This means that in most cases women are forced to pay
for a state-guaranteed examination from their personal budget.
Women also have to pay for additional examinations or a repeated
visit to a gynaecologist, because state-guaranteed examinations often are
not sufficient for obtaining credible results for cervical cancer diagnosis
and often women discontinue examinations even without learning the
results, because it takes additional financial resources and time.
Colorectal cancer screening has had the lowest coverage during
these two years. It should be mentioned that in Latvia not all physicians
have been trained in performing colorectal cancer screening. Moreover,
there are no confirmed EU guidelines for colorectal cancer screening.
In continuing the analysis of existing situation, it should be noted
that presently in Latvia there are no institutions collecting data on clinical
results of performed examinations, controlling the quality of screening
Early Detection of Cancer by Screening
37 of 50
Policy Initiatives
examinations and summarizing data on the impact of the screening
programme on oncological morbidity data. HCISA receives information on
the number of screening manipulations performed and identification of the
examined persons for service payment, whereas substantial information on
clinical results of the screening remains in individual medical documents in
charge of general practitioners or gynaecologists and are not summarized
by any institution or a database.
Consequently, information on the general situation in the state is
incomplete and inadequate; there is no possibility to evaluate the clinical
and economical efficiency of screening system in Latvia and its impact on
incidence and mortality indicators, as well as to perform an analysis of
indicative screening indicators adopted internationally and their
comparison with indicators of other states.
It is common experience in many EU countries that implementation
of a well-designed, comprehensive national cancer control programme,
adjusted to local conditions, can improve the situation in oncology in a few
years' time by decreasing cancer mortality, proportion of late diagnoses
and the general prevalence of cancer, even in circumstances of limited
financial resources.
Also the draft National Cancer Control Programme developed in
Latvia stipulates the following policy results to be reached:
raised level of public awareness about factors that may potentially
prevent cancer (healthy sustenance, avoiding known carcinogens,
giving up addictive habits, enhancing physical activities, leading
healthy lifestyle, timely treatment of chronic infections);
implemented organized cancer screening programme based upon the
data provided by the Register of Inhabitants and established cancer
screening management and control institution ensuring a centralized
database, data monitoring and analysis of basic screening indicators,
reaching screening coverage of 75% in three years’ time;
general practitioners actively inviting and examining patients for a
timely diagnostics of visually detectable cancer, reaching general
improvement of early detection and decrease in the number of
neglected cases by 12%;
developed and implemented guidelines of minimal recommendations
for detection and treatment of oncological diseases, thus providing
an appropriate, cost-effective and available detection of oncological
diseases and their treatment for all inhabitants of Latvia.
Early Detection of Cancer by Screening
38 of 50
Policy Initiatives
It should be mentioned that the draft National Cancer Control
Programme has been submitted to the Ministry of Health for evaluation.
Considering the present state in the field of oncology, discussions at
various levels about this draft programme are expected that will help
professionals in cooperation with decision-makers find solutions that are
best adjusted to the situation in Latvia. For instance, policy results defined
in the mentioned draft programme should be adjusted to the current
situation.
Early Detection of Cancer by Screening
39 of 50
Conclusions and Recommendations
CONCLUSIONS AND RECOMMENDATIONS
Conclusions
Mortality due to cancer is the second leading cause of death in Latvian
inhabitants, after cardiovascular diseases (almost 18% of all deaths),
and it shows an increasing trend.
Oncological morbidity has an increasing trend.
Cancer incidence indicators in Latvia are lower compared to other EU
countries, while mortality indicators are higher. This is evidence of late
detection of cancer.
Coincident increase of incidence and mortality is evidence of possibly
late detection.
Almost 60% of first diagnoses are made at advanced stages — III–IV
stages (25% — in IV stage).
Recently, a slight improvement of situation is seen in timely detection
of cancer (the number of cancers detected in I–II stage has slightly
increased), as evidenced by a slight increase in the five-year survival
rates and a decrease in first-year lethality.
In comparison with the indicators of the EU-15, in Latvia first-year
lethality is very high (34%) and five-year survival — low (45%).
Breast cancer in women occupies the first place in the structure of
cancer incidence and mortality.
In comparison with other EU states, breast cancer incidence and
mortality in Latvia is lower. However, indicators of premature (at the
age 0-64) standardized mortality indicators in Latvia are among the
highest in the EU.
Breast cancer incidence and mortality in dynamics shows an increasing
trend. During the past ten years, incidence has increased by 23% and
mortality — by 15%. The highest breast cancer incidence is in the age
group over 50.
One third of breast cancers are detected at an advanced stage (III–IV
stage), even though timely detection of breast cancer within screening
programmes with mammography examinations allows for effective
treatment and even recovery.
Colorectal cancer is one of the most frequently detected cancers in men
and in women, especially after the age of 60. Incidence and mortality
indicators are almost two times higher in men than in women.
Colorectal cancer incidence and mortality has an increasing trend,
which is related to late detection (in more than a half of patients), thus
outpacing late detection rates for breast and cervical cancer, and also to
Early Detection of Cancer by Screening
40 of 50
Conclusions and Recommendations
ageing of population (the majority of incidence and mortality cases
occur in the age group over 60).
Also in the case of colorectal cancer, by detecting pre-cancer conditions
or an early stage of this cancer with screening the treatment is easier
and complete recovery rates are higher. If these cancer types are
detected at advanced stages, survival rate will be low, for instance, in
IV stage it does not reach even 10%.
Cervical cancer is one of the cancer types affecting women at an earlier
age than cancers of other localizations (almost half of women are aged
under 60), and it is preventable by timely detection of pre-cancer
diseases.
Cervical cancer incidence has an increasing trend. Mortality remains
almost at the same level.
In comparison with other EU states, cervical cancer incidence rates in
Latvia are similar to those of other “new” member states and are higher
than in the “old” member states; mortality indicators are noticeably
higher than on average in the EU-27.
Although oncocytological screening for cervical cancer allows for
detection of pre-cancer diseases that can be treated, thereby decreasing
cervical cancer incidence and mortality, in Latvia mortality and firstyear lethality is high (25%), which, in its turn, is influenced by late
detection of more than 40% of cases (in III–IV stages). Decrease in
five-year survival rates is a negative trend (in 2005 — 46%).
Comparison of incidence indicators for cancers detectable by screening
reveals that breast cancer has the highest incidence. Accordingly, breast
cancer has the smallest (compared with the other two cancer
localizations) proportion of late detection (in III–IV stages) and firstyear lethality.
Even though high mortality, compared to incidence, attests to late
detection and low survival, it also shows a noticeable potential for the
improvement of these indicators.
Early Detection of Cancer by Screening
41 of 50
Conclusions and Recommendations
Conclusions on screening implementation in Latvia
Despite the state-paid service, screening coverage is very low and stateguaranteed financing for preventive services is not spent.
Possible causes for insufficient use of screening services are nonawareness of inhabitants, lack of motivation of physicians and
inhabitants, and limited availability of health care services.
Quality requirements (quality control exists only in laboratories) and
screening implementation guidelines are not developed.
Existing system is aimed at young, energetic people capable of paying
and mainly residing in towns (this means that prevention reaches
educated, responsible and active patients), and it is ineffective for the
improvement of the situation, because it involves either individuals with
lower risk or symptomatic patients, thus making screening a diagnostic
procedure.
Capacity and technical equipment evaluation has not been performed in
correspondence with the needs of current screening, existing capacity is
to be evaluated as insufficient;
Lack of unified accounting impedes the evaluation of the situation in
the state and does not provide objective information on actual screening
coverage.
Decentralized or opportunity screening system is low-efficient, because
late detection and high mortality remains unchanged.
Early Detection of Cancer by Screening
42 of 50
Conclusions and Recommendations
Recommendations
To improve primary and secondary cancer prevention measures.
To improve early detection of cancer in order to decrease cancer
mortality and incidence of potentially preventable cancers, thus
improving treatment efficiency and life quality of cancer patients in
Latvia:
- to plan the development of a centralized and organized screening
system — to develop guidelines for cancer screening adjusted to
situation in Latvia and available financial resources, using guidelines
of the European Union and recommendations of WHO.
- to improve efficiency of existing screening by motivating doctors,
actively informing and inviting inhabitants, increasing the capacity
of health care institutions (for instance, employed registrar joining
the team of a general practitioner), summarizing and analyzing
screening data etc.
To solve questions related to health promotion by performing
comprehensive informative and educational activities related to cancer
prevention (including the use of screening services).
To evaluate and discuss the draft National Cancer Control Programme
among professionals and decision-makers and approve it.
Early Detection of Cancer by Screening
43 of 50
Comments on Data
COMMENTS ON DATA
Data of Latvian Cancer Registry have been used for the preparation
of the report. For the calculation of relative indicators (per 100 000
inhabitants), CSB demographic data were used.
For international comparisons, WHO Health for All database and
information from EUROSTAT databases available over the Internet were
used. Mainly standardized indicators were used for drawing comparisons
among the states in order to avoid discrepancies due to different age
structure of inhabitants in different states.
For data analysis, mainly relative indicators — per 100 000
inhabitants of the relevant age, gender and place of residence — were used.
The draft guidelines “National Cancer Control Programme for 2007–
2017” were also used for the analysis of indicators.
DEFINITIONS
Incidence (morbidity) — an indicator characterizing a number of
new cases of cancer within a unit of time in a certain risk population.
Mammography — examination of breast tissue using x-rays.
Oncocytology — a test of cytological material for cancer detection,
in practice it usually means a cytological test of cervical smear.
Opportunity screening diagnostics — performance of screening
examinations outside the framework of the organized system of screening
diagnostics without associating it with the data from the Registry of
Inhabitants. It is also referred to as chaotic screening diagnostics, because
inhabitants perform testing on their own initiative or after a
recommendation of a third person (a physician, a friend). Main features of
the opportunity screening are the following: a centralized list of persons to
be screened is not created, a centralized information system is missing, a
central coordination organization for screening procedures does not exist, a
central database of screening examinations is missing, a continuous
analysis of performance indicators of a screening programme is not made,
performance guidelines do not exist.
Organized (centralized) screening diagnostics — a screening
programme based upon the data from the Registry of Inhabitants with a
centralized sending of invitations, establishment of a database of indicators
and clinical data and a continuous monitoring of the results.
Early Detection of Cancer by Screening
44 of 50
Comments on Data
Five-year survival — the percentage of patients who have lived for
five years after diagnosis in relation to all patients who developed a disease
during the relevant time period.
First-year lethality — the ratio between the number of patients who
died during the first year after diagnosis and the number of all patients with
the given diagnosis during the relevant time period.
Potential years of life lost — years of life a person would have
lived before a certain age (in this study — the age of 65) if he or she had
not died in an accident, due to a disease or any other cause.
Primary prevention — a complex of measures aimed at elimination
of potential disease coefficients, thus protecting an individual from
developing a disease. For instance, giving up smoking, promotion of a
healthy lifestyle (diet, physical activity), and vaccination.
Secondary prevention — a complex of diagnostic measures
providing for a possibility of early detection of a disease, when in most
cases a complete recovery or protection of an individual from developing
cancer of the relevant localization by a timely detection and elimination of
a precancerous disease is possible.
Screening diagnostics or screening — a targeted search for a
disease (in this study — cancer) in asymptomatic people included in the
risk group (most often in a certain age group) of the highest incidence of a
certain disease.
Screening indicators — previously defined parameters for objective
evaluation of screening programme efficiency.
Cancer — a general term for malignant tumours, widely used by the
public and medical professionals.
ABBREVIATIONS
CSB
EU
LOC
CM
WHO
PYLL
MoH
HCISA
HSMTSA
Central Statistical Bureau of Latvia
European Union
Latvian Oncology Centre
The Cabinet of Ministers
World Health Organization
potential years of life lost
Ministry of Health
Health Compulsory Insurance State Agency
Health Statistics and Medical Technologies State Agency
Early Detection of Cancer by Screening
45 of 50
REFERENCES
1
Statistical Yearbook of Health Care in Latvia, Health statistics and Medical Technologies State Agency,
Riga 2006
2
National Cancer Control Programmes. Policies and managerial guidelines. 2nd Edition, 2002
3
Draft Guidelines “National Cancer Control Programme for 2007–2017”;
4
National Cancer Control Programmes. Policies and managerial guidelines. 2nd Edition, 2002
5
Wilson & Junger (WHO), 1968
6
Draft Guidelines “National Cancer Control Programme for 2007–2017”
7
National Cancer Control Programmes. Policies and managerial guidelines. 2nd Edition, 2002
8
Draft Guidelines “National Cancer Control Programme for 2007–2017”
9
Eurocare-3; Sant et al., 2003
10
Draft Guidelines “National Cancer Control Programme for 2007–2017”
11
EU-SILC study - Survey on Income and Living Conditions
12
“Transforming the Latvian Health System. Accessibility of health services from pro-poor perspective”
German Develpoment institute, 2004
13
Study “Availability of Health care Services in Riga and Vidzeme” performed by Latvia University
Postgraduation Medical Education Institute and Latvia University Philosophy and Sociology Institute
14
Proposal for an indicator to measure potential and self-reported unmet care needs and barriers to access;
Discussion paper for the ISG meeting 27-28 March 2007
15
Council recomendation on cancer screening, Brussels, 5.5.2003
16
Draft Guidelines “National Cancer Control Programme for 2007–2017”
17
European guidelines for quality assurance in breast cancer screening and diagnosis, 4th edition, 2006
Early Detection of Cancer by Screening
46 of 50
Annexes
Figure 1. Cancer incidence in towns and regions of Latvia in 2005 (per
100 000 inhabitants)
(LOC data – Report 2005)
Per 100 000 inhabitants
600
500
400
300
200
100
Liepaja
Ventspils Kraslava
region
Kuldiga
region
Valmiera
region
Ogre
region
Bauska
region
Balvi
region
Jelgava
region
Riga
region
Figure 2. Proportion of cancer patients in different age groups (percentage)
(LOC data – Report 2005)
100
Percentage
80
60
40
20
0
0 - 20
20 - 40
40 - 60
>60
>70
Figure 3. Potential years of life lost (per 100 000 inhabitants) due to cancer
in men
(PHA data)
Early Detection of Cancer by Screening
47 of 50
PYLL per 100 000 inhabitants
400
350
300
250
200
150
100
50
0
Lung cancer
Gastric cancer
Colorectal cancer
Prostate cancer
1999
2000
2001
2002
2003
2004
2005
Year
Figure 4. Potential years of life lost (per 100 000 inhabitants) due to cancer
in women
Per 100 000 inhabitants
(PHA data)
300
Breast cancer
Cervical cancer
Gastric cancer
Colorectal cancer
Ovarian cancer
250
200
150
100
50
0
1999
2000
2001
2002
2003
2004
2005
Year
Figure 13. Colorectal cancer incidence and mortality in men (per 100 000
inhabitants) in 2005
Per 100 000 inhabitants
(Data of Latvian Cancer
Registry)
500
450
400
350
300
250
200
150
100
50
0
Incidence
M ortality
35 - 39 40 - 44 45 - 49 50 - 54 55 - 59 60 - 64 65 - 69 70 - 74 75 - 79 80 - 84
85 and
older
Year
Early Detection of Cancer by Screening
48 of 50
Figure 6. Colorectal cancer incidence and mortality in women (per 100 000
inhabitants) in 2005
(Data of Latvian Cancer Registry)
Per 100 000 inhabitants
250
Incidence
200
150
Mortality
100
50
0
35 - 39
40 - 44
45 - 49
50 - 54
55 - 59
60 - 64
65 - 69
70 - 74
75 - 79
80 - 84
85 and
older
Year
Figure 7. Five-year survival rates for patients with colorectal cancer
Percentage
(Data of Latvian Cancer Registry)
100
90
80
70
60
50
40
30
20
10
0
I stage
II stage
III stage
IV stage
1999
2000
2001
2002
2003
2004
2005
Year
Figure 8. Five-year survival rates for patients with breast cancer
Percentage
(Data of Latvian Cancer Registry)
100
90
80
70
60
50
40
30
20
10
0
I stage
II stage
III stage
IV stage
1999
2000
2001
2002
Year
Early Detection of Cancer by Screening
2003
2004
2005
49 of 50
Figure 9. Potential years of life lost and mortality from breast cancer (per
100 000 inhabitants) in 2005 by age groups
(Data from Latvian Cancer Registry and PHA)
Per 100 000 inhabitants
80
PYLL
70
60
Mortality
50
40
30
20
10
0
25 - 29
30 - 34
35 - 39
40 - 44
45 - 49
50 - 54
55 - 59
60 - 64
Year
Figure 10. Potential years of life lost and mortality from cervical cancer (per
100 000 inhabitants) in 2005
Per 100 000 inhabitants
(Data from Latvian Cancer Registry and PHA)
20
18
16
14
12
10
8
6
4
2
0
PYLL
25 - 29
Mortality
30 - 34
35 - 39
40 - 44
45 - 49
50 - 54
55 - 59
60 - 64
Year
Early Detection of Cancer by Screening
50 of 50