Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
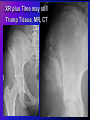
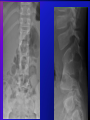
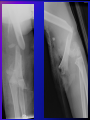
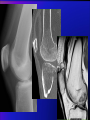
Introduction to MSK Imaging Studies: “Don’t Panic” Donna Magid, MD, M.Ed Director, Horizontal Strand in Diagnostic Imaging Professor, Radiology, Orthopaedic Surgery, and Functional Anatomy and Evolution Objectives Introductory concepts of MSK Imaging ‘REQUESTING’ vs ‘ORDERING’ studies Sequencing MSK studies: what to do when ACR Appropriateness Criteria to the rescue! Give you life-long fishing skills rather than handing over fish. Common errors: Forgetting “One view is no view” Skipping usual steps Not reviewing older studies Pro/cons of common imaging modalities: XR, CT, MR, US YOU: Intelligent Consumers of Medical Resources (not optional) Common indix. head CT = “R/o stroke, dizzy” Legitimate concern for stroke (but overinclusive). Inner-ear-pt. subset: benign, conservative tt. Better clinical ED screen for benign ear etiologies could reduce CT in US by $500 million/year. Newman-Toker et al, Academic Emergency Medicine July 2013 “ Intelligent Consumer” may mean NOT utilizing imaging (unnecessarily…$, dose) ED(USA) 2006: 34% radiographed (more, JHH) 12% CT Pitts, Niska et al National Health Statistics report (7)2006 CT tripled, 19962010 Smith-Bindeman, JAMA June 2012 “KISS” : Import old studies! Outside studies reduce new by: 17% overall CT: 29% Sodickson, Opraseuth, Ledbetter; RADIOLOGY 2011:260 (2) Remember one does not ‘ORDER an exam’, one ‘REQUESTS a CONSULT’ Consulting Radiologist needs info. to confirm: Correct study requested Correct Pt. Meds, allergies, status, caveats Cost/benefit ratio favors the patient: Risk, dose, pain, complications, sometimes $$ ‘Will it alter management?’ If not—NO! DNR, religious beliefs, life expectancy… Info already known or available (old images) The Imaging Requisition Electronic, faxed, written….. Varies, morphs often Pt. Name – MRN – DOB – Location (wrist band, paperwork, chart) Deal-breakers = Misspelling, mismatches Contact/Requesting Clinician, ACCURATE phone, page: Questions before test performed URGENT findings, emergencies Females of child-bearing age (~9 to 90): Pregnancy status Known allergies Known caveats or contraindications (dialysis stent, implants, metal, 1 day post-op, deaf, non-English speaking…) Imaging Request asks a question “Worry/Don’t Worry” “Normal/Abnormal” (old images!) “Better/Worse” (size, radiodensity, signal, fluid…) “Bigger/Smaller/Unchanged” Narrow or confirm initial DDx Better localize a finding (in 3D, organ, tissue, …) Better characterize a finding (cystic, solid,…) Requistion: Clinical Info Concise and Precise (“G.I.G.O.”) “Fx”,“R/O”,“Pain”,“Fell” … inadequate! Localize with ONE finger Describe mechanism/force if trauma: “MVC” “Belted passenger, T-boned on R high veloc.’ or ”Pedestrian, struck laterally in parking lot, landed on/pain R hip” vs Time frame: new; older; chronic ‘Today…5 days ago…4 months…..5 years……’ Give us adequate info and query, not a protocol Clinical info, DDx, concerns, clues, labs, query Let us protocol the technical details of exam Let us decide on which machine (esp. CT, MR) CT: “R/O intracranial bleed, fell 8 ft, LOC”, not just “Dry head CT, reformats” w/o clinical info MR: “Adenoca lung, confusion, R/O brain mets”; not ‘T1, T2, brain w/, w/o, contrast”, no other info INTRODUCTORY MSK IMAGING: ‘Don’t Panic’ Musculoskeletal Imaging: Bones (cortical, articular, marrow, physis) Joints (cartilage, ligament, tendon, fluid) Ligaments, Tendons (XR, MR) Cartilage (articular, meniscal, fibro-: XR, MR, CT,) Soft tissue (muscle, fascia, fat: XR, CT, MR, US) Vascular (vessels, blood supply: XR,CT, MR, US) Neurography (MR) MSK Imaging: cost/benefit Pediatric vs Adult (hip, appx, brain: Fertility, Life expectancy DDx (differential diagnosis) Trauma Infectious/inflammatory Neoplastic Vascular Iatrogenic Arthritis, connective tissue Metabolic Developmental/congenital/genetic Normal or Nl. Variant US v CT) MSK Imaging Tx- and Dx-Specific DDx (differential diagnosis) Trauma (acute, chronic, velocity or force) Infectious/inflammatory (acute, chronic, immunocomp.) Neoplastic (new, treated, recurrent) Vascular Iatrogenic (surgery, foreign matter, Rx) Arthritis, connective tissue Metabolic Developmental/congenital/genetic Give us adequate info, query; not a protocol Imaging techniques, equipment, changing rapidly. Unlikely a non-Radiologist can keep up; even Radiologists are scrambling. On-line Mind Palaces…. Modalities: ‘First Things First’ Short-cuts counterproductive RADIOGRAPHY (conventional images) remains the gateway to (MSK) imaging assessment. It is NOT going away. XR plus Time may still Trump Tissue, MR, CT RADIOGRAPHY: “One View Is No View” Once a study indicated – no shortcuts. Not for age, gender, cost, dose……. Many findings underwhelm on one view Complex 3D structures need 2 Views Fractures, Dislocations Toddler’s Fracture Slipped Capital Femoral Epiphysis CT vs MR: CT: Rapid (7 seconds) movement, cooperation pro/com MR: No radiation Contrast rxn. v. rare Superb soft tx. info. Freely reformattable Windows ex post facto Superb resolution “WYSIWYG” per sequence Contrast rxn. rare Much slower (45-90 min) Metal can be imaged Claustrophobic Metal = abs. contraindx, 2x High-dose radiation Less resolution Metal can degrade image Expensive (~2x CT) Expensive but ~$1/2 MR Weight, size limits: both CT vs MR: What is the Question? CT: “4 Bs” radiodense MR: Soft tx– ligament, muscle, Bone tendon, cartilage, Blood (acute hemorrhage) muscle, neural, tumor Bullets and metal Molecular differences Barium (ie contrast) Better soft tissue detail Lung and chest Direct multiplanar Cancer staging Speed overcomes motion Non-polar materials not visualized ie, bone (calcium). <-- CT MR CT MR US: When and Where? MSK: Currently limited in adults; rapidly changing PRO: CON: Portable Fat, bone, air, metal, Safe (no dose no risk), all block US Far less expensive Low resolution GYN, Doppler flow Highly user-dependent Echocardiograph Non-intuitive (‘weather maps’) RUQ abdomen Bx, line placement,‘taps’ (pleural, abscess, joints) DVT: proximal extremities Breast: cyst vs solid US: Soft tissue, Flow Barriers: Bone, Fat, metal, air… Rheumatoid arthritis. Gutierrez M et al. Ann Rheum Dis 2011;70:1111-1114 ©2011 by BMJ Publishing Group Ltd and European League Against Rheumatism ACR AC American College of Radiology Appropriateness Criteria www.acr.org Evidence-based guidelines to choose imaging 200 Dx with 900 scenarios/variants; referenced Relative Radiation Risk each study Modality guidelines CT, MR, US, Nucs, PET,… Practice Guidelines: When (in what order) to perform: Radiography, CT, MR of the extremities Spine Radiography, CT, MR Scoliosis radiography (Portable chest, Abdominal radiography, hysterosalpingograms, Dxc Ct, Pediatric CT, Ct colonoscopy, MR knee, MR brain, US, …) Varied Clinical Scenarios per DDx 200 Dx with 900 variants (modifiers); eg: Blunt Chest Trauma: 3 variations per clinical/XR Acute hip pain, suspected fx.: 2 variations, 4 pgs discussion Acute shoulder pain Chronic wrist pain Chronic neck pain Imaging after arthroplasty (joint replacement) Non-traumatic knee pain Soft tissue masses Suspected avascular necrosis “Acute Shoulder Pain” Initial =s XR, then branches into detailed specifics Acute shoulder pain (leave choice of initial XR views to us) ‘Any etiology, initial study’: XR=9(best); CT, MR, US=1(worst) ‘XR neg, significant persistant pain’ MR (9); CT (5) ‘XR neg, under 35, suspect labral tear’ MR arthrog(9), MR(7), CT(5) ‘XR neg, prior rotator cuff repair, suspect re-tear ‘ MR (9) w. or w/o ‘XR neg, suspect septic arthritis’ arthrocentesis (9), MR w&w/o (7) Jumping straight to sophisticated imaging = mistake. Short-cuts, ‘time-savers’, pervert accurate diagnosis. Radiography (‘plain film”) NOT going away! “LOW BACK PAIN” 80% of over-45 yo “Uncomplicated, no red flags(explained)”: All imaging = ‘2’ ‘With radiculopathy, surg. candidate” MR w/o (8); CT (5) “Low-veloc trauma, osteoporosis, focal/progressive deficit, prolonged sx, or >70 yo” XR then MR “Possible cancer, infection, and/or known immunosuppression” -> MR w&w/o (8); MR w/o (7); CT(6); “Prior lumbar surgery” MR w&w/o (8); MR w/o (6) CT (6) By the time you straighten this out… Standard of Care (SOC) may have changed again EPIPHANY: One need not understand physics to request proper exam Understand what each modality can/cannot do, not ‘why’, nor ‘how’. Use resources– ACR AC, Radiologists– to confirm appropriate next-step. RESOURCES constant, ANSWERS change often. Commonly used studies will become familiar. Less-common….won’t. Don’t worry. ASK US! http://3rads.jhmi.edu/ All imaging phone numbers When to use contrast, what study to get, can be counter-intuitive and subtle. Include us on the patient care team; we are CONSULTANTS, not lab techs. On-call techs, all modalities/subspecialties: use 3Rads.jhmi.edu Back-up: ask Emed Radiology Resident 7-5442 Dxc. Imaging: TTW 2014 “REPETITION IS THE KEY TO LEARNING” Intro to Chest Radiographs: The Ur-unit of imaging Thank you! Donna Magid, MD, M.Ed