Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
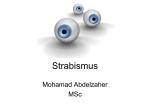
BMJ 2015;351:h5385 doi: 10.1136/bmj.h5385 (Published 18 November 2015) Page 1 of 3 Practice PRACTICE 10-MINUTE CONSULTATION Double vision 1 Liying Low academic clinical fellow in ophthalmology , Waqaar Shah general practitioner and RCGP 2 3 clinical champion in eye health , Caroline J MacEwen professor of ophthalmology Academic Unit of Ophthalmology, University of Birmingham, Birmingham B18 7QH, UK; 2Clinical Innovation and Research Centre, Royal College of General Practitioners, London, UK; 3Ophthalmology Department, University of Dundee, UK 1 A 70 year old woman presents with a three day history of painless double vision. What you should cover Double vision, or diplopia, may be the first sign of life threatening pathology, or it may be completely benign. A rapid and systematic assessment is, therefore, crucial.1 Assessment • Is the diplopia is monocular or binocular? The latter may indicate a life threatening cause1 Monocular—Diplopia persists when one eye is covered. “What does the extra image look like?” The extra image typically appears as a ghost or shadow. Generally indicates abnormalities of the eye itself, including dry eyes, corneal pathology or scarring, cataracts, and non-organic causes. Binocular—Diplopia occurs with both eyes open and disappears when either eye is covered. – Are the images separated vertically (on top of each other), or horizontally (side by side)? Vertical diplopia indicates impaired elevation or depression of the eye (such as decompensated squints, thyroid eye disease, fourth nerve palsies (figure⇓), orbital trauma), whereas horizontal diplopia suggests impaired adduction or abduction of the eye (such as decompensated squints, sixth nerve palsies (figure⇓), multiple sclerosis). – Is the double vision constant, intermittent, or variable? Patients with intermittent diplopia should be asked about timing, duration, and frequency of symptoms, and exacerbating and relieving factors. Intermittent diplopia worse in the evenings or with fatigue suggests myasthenia gravis or decompensating squint. Diplopia worse with spectacle prescription change suggests an accommodative or spectacle induced cause (both benign). – Is the double vision worse with any particular direction of gaze? (see figure⇓) • Onset of symptoms—Sudden onset of diplopia usually indicates acute aetiology, such as ischaemia or vascular compression. Gradual or intermittent onset may indicate decompensation of a latent or longstanding squint. Vague onset may be seen in thyroid eye disease. • Associated features—Are there any associated headaches or pain around the eyes? May indicate ischaemia, inflammation, infection, raised intracranial pressure, or aneurysm. • Weakness or fatigue—Is there any associated weakness or fatigue, particularly in the evenings, droopy eyelids, or difficulty swallowing? Possible myasthenia gravis. • Trauma—Is there any recent head or facial trauma? Blow-out orbital fractures may cause extraocular muscle entrapment or damage. • Other features—Is there any new onset headache, scalp tenderness, unexplained weight loss, or pain when chewing? Possible giant cell arteritis. • Ocular history—Childhood squint or amblyopia, eye muscle surgery, or new glasses may suggest a longer term aetiology. • Medical history—Diabetes, hypertension, and vasculopathic risk factors are associated with cranial nerve microvascular ischaemia. Include history of thyroid disease, cancer, and multiple sclerosis. • Drug history—Drugs such as lamotrigine, topiramate, gabapentin, fluroquinolones, and citalopram have been associated with diplopia, but it is a rare adverse effect. Correspondence to: L Low [email protected] This is part of a series of occasional articles on common problems in primary care. The BMJ welcomes contributions from GPs. For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h5385 doi: 10.1136/bmj.h5385 (Published 18 November 2015) Page 2 of 3 PRACTICE What you need to know • Binocular diplopia may indicate a life threatening condition, and a stepwise approach is needed to distinguish this sort of diplopia from benign monocular diplopia • Red flags for urgent referral: new headache or ocular pain, unilateral pupil dilation, neurological features or fatigability, ptosis, facial trauma, papilloedema • Advise all patients with diplopia to stop driving Examination Urgent, same day referral • Observe any abnormal head position (tilt or face turn) and compare with old photographs, which would support a longstanding problem. • Painful third nerve palsy with ipsilateral dilated pupil or sixth nerve palsy with papilloedema—Refer to either acute medical or neurosurgical team for same day neuroimaging. • Observe the eyelid position—Ptosis of the upper eyelid may indicate third nerve palsy or myasthenia gravis, lid retraction may indicate thyroid eye disease. • Suspected giant cell arteritis—Refer to either the rheumatology or acute medical team or the ophthalmology team for urgent tests (including erythrocyte sedimentation rate and C reactive protein) and high dose corticosteroid treatment. • Inspect for strabismus (misalignment of the eyes)—For example, in third nerve palsy the affected eye turns “down and out” (figure⇓). • Acute onset diplopia associated with facial trauma—Refer to the maxillofacial or ophthalmology team. • Inspect for proptosis (protrusion of the eyeball)—Suggests orbital cellulitis, orbital tumours, thyroid eye disease, or carotid cavernous fistula. • Is the diplopia is monocular or binocular?—Cover each eye in turn and ask if the diplopia persists with either eye covered. • Assess visual acuity in each eye—Longstanding reduced vision in one eye suggests amblyopia, while new onset reduced vision suggests orbital or neurological lesion. • Pupil size and responses—A unilateral dilated pupil in association with headache and diplopia highly suggests an intracranial aneurysm (third nerve palsy), a neurosurgical emergency. Unilateral lid ptosis with pupillary miosis and unilateral cranial nerve palsies suggests Horner’s syndrome secondary to cavernous sinus pathology. These are red flag signs. • Examine eye movements in nine positions of gaze—Ask if double vision worsens with different positions of gaze (figure⇓). • Cranial nerve and peripheral nervous system examination should be completed in all cases of suspected extraocular muscle weakness. Multiple cranial nerve palsies indicate intracranial or meningeal based tumours, meningitis, polyneuropathy, multiple sclerosis, or cavernous sinus lesion. • Papilloedema must be excluded in all cases of sixth nerve palsy (reduced abduction) as it can be a false localising sign of increased intracranial pressure. • Red flag symptoms need referral to the acute medicine or ophthalmology team. Routine referral to ophthalmology department Patients with: • Any painless monocular diplopia or longstanding diplopia. • Isolated fourth and sixth cranial nerve palsies. They should have cardiovascular risk factor work up.3 • Suspected thyroid eye disease. They should have thyroid function tests performed and be advised to stop smoking. We thank Caitlin Monney for the illustration provided in this article. Contributors: LL conceived and designed the manuscript. LL and CJM wrote the first draft. All authors revised and critically appraised the manuscript and gave final approval for publication. Competing interests: We have read and understood BMJ policy on declaration of interests and have no relevant interests to declare. 1 2 3 O’Colmain U, Gilmour C, MacEwen CJ. Acute-onset diplopia. Acta Ophthalmol 2014;92:382-6. Drivers Medical Group. For medical practitioners: at a glance guide to the current medical standards of fitness to drive . DVLA, 2014. Tamhankar MA, Biousse V, Ying GS, et al. Isolated third, fourth, and sixth cranial nerve palsies from presumed microvascular versus other causes: a prospective study. Ophthalmology 2013;120:2264-9. Accepted: 26 Aug 2015 Cite this as: BMJ 2015;351:h5385 © BMJ Publishing Group Ltd 2015 What you should do Advise patients with diplopia not to drive.2 For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h5385 doi: 10.1136/bmj.h5385 (Published 18 November 2015) Page 3 of 3 PRACTICE Red flags. Signs of serious causes of binocular diplopia that require urgent, same day referral • New onset of headache or ocular pain • Unilateral pupil dilation • Associated neurological features or fatigability • Ptosis • Facial trauma • Papilloedema Further reading • Lee MS. Diplopia: diagnosis and management. focal points. Vol 25. American Academy of Ophthalmology, 2007—A detailed description of diagnosis and management of diplopia • Rucker JC, Tomsak RL. Binocular diplopia. A practical approach. Neurologist 2005;11:98-110—A logical stepwise approach to assessing patients with diplopia Figure Interpretation of incomitance (that is, angle of squint varies with direction of gaze) For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe