Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Diagnostic pitfalls mimicking meniscal tears: MR imaging
evaluation with arthroscopic correlation
Poster No.:
C-611
Congress:
ECR 2009
Type:
Educational Exhibit
Topic:
Musculoskeletal
Authors:
I. Tsifountoudis, I. Kalaitzoglou, A. Haritanti, I. Economou, A. S.
Dimitriadis; Thessaloniki/GR
Keywords:
MRI, Meniscus, Diagnostic pitfalls, Postoperative meniscus
DOI:
10.1594/ecr2009/C-611
Any information contained in this pdf file is automatically generated from digital material
submitted to EPOS by third parties in the form of scientific presentations. References
to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in
any way constitute or imply ECR's endorsement, sponsorship or recommendation of the
third party, information, product or service. ECR is not responsible for the content of
these pages and does not make any representations regarding the content or accuracy
of material in this file.
As per copyright regulations, any unauthorised use of the material or parts thereof as
well as commercial reproduction or multiple distribution by any traditional or electronically
based reproduction/publication method ist strictly prohibited.
You agree to defend, indemnify, and hold ECR harmless from and against any and all
claims, damages, costs, and expenses, including attorneys' fees, arising from or related
to your use of these pages.
Please note: Links to movies, ppt slideshows and any other multimedia files are not
available in the pdf version of presentations.
www.myESR.org
Page 1 of 40
Learning objectives
MRI has been established as a very sensitive method for the diagnosis of
meniscal tears. To maintain high accuracy, radiologists should be aware of
potential pitfalls in interpretation. Our purpose is to review these potential
causes of confusion, to describe the mechanisms by which they may create
foci of pathologic signal intensity similar to meniscal tears and to recommend
methods to avoid false-positive and false-negative interpretations.
Background
The findings from MRI examinations of 310 knees were retrospectively
interpreted and correlated with prospectively recorded results from
arthroscopic examinations performed between 2006 and 2008.
The imaging protocol consisted of: a) T1-weighted fast spin-echo (FSE), b)
proton density (PD)-weighted and T2-weighted FSE, c) T2 gradient (GRE)weighted and d) short-tau inversion recovery (STIR) sequences.
Of the knees examined, 255 meniscal tears were identified. Furthermore, 27
false-positive and 14 false-negative findings were detected.
Imaging findings OR Procedure details
False-positive and false-negative findings were attributed to pitfalls in
interpretation which may be caused by: (a) normal structures of the
knee which project in close relationship to the menisci, such as anterior
transverse ligament, meniscofemoral ligaments, oblique menisco-meniscal
ligament and popliteal tendon and bursa, (b) normal variants of the
menisci such as meniscal flounce, speckled anterior horn of the lateral
meniscus and Wrisberg's variant of a discoid lateral meniscus, (c) MRI
artifacts created by the pulse sequences used, such as magic angle
phenomenon, volume averaging, motion and truncation artifacts, (d) various
pathologic conditions of different etiology, such as chondrocalcinosis,
meniscal ossicles and gas within the joint and (e) postoperative changes
of the menisci.
Page 2 of 40
NORMAL ANATOMIC STRUCTURES
Normal anatomic structures that lie in close proximity to the meniscus and
show similar MR signal intensity to the meniscus are common mimickers of
meniscal pathology.
The anterior transverse ligament attaches the anterior margin of lateral
meniscus to the anterior horn of medial meniscus (Fig.).
Fig.: The anterior transverse ligament is clearly demonstrated on coronal PD-W fat
sat (a) and T1-W images (b) and on axial PD-W fat sat (c) and T1-W images (d) as
it courses from the anterior margin of lateral meniscus to the anterior horn of medial
meniscus.
On sagittal images, a linear band of increased signal is present between
the anterior horn of lateral meniscus and the anterior transverse ligament,
occasionally simulating an oblique meniscal tear (Fig.) [1].
Page 3 of 40
Fig.: A linear band of increased signal intensity (arrowhead) is noticed on a sagittal
PD-W fat sat image (j), between the anterior horn of lateral meniscus and the anterior
transverse ligament (arrow), simulating an oblique meniscal tear. The course of
the ligament is clearly demonstrated on adjacent sagittal PD-W fat sat images (ej). Osgood-Schlatter disease is also present with patellar tendon thickening, deep
infrapatellar bursitis and tibial tubercle fragmentation.
By the same mechanism, increased linear MR signal in the medial aspect
of the posterior horn of lateral meniscus at the attachment site of the
meniscofemoral ligament can mimic the appearance of a vertical meniscal
tear. The meniscofemoral ligament originates from the lateral meniscus
posteriorly and inserts on the medial aspect of medial femoral condyle. The
ligament is composed of 2 separate branches, the ligament of Humphry and
the ligament of Wrisberg (Fig.).
Page 4 of 40
Fig.: Diagram showing the origin of meniscofemoral ligaments from the medial aspect
of the posterior horn of lateral meniscus.
On sagittal MR images, these are seen as low signal intensity ovoid
structures anterior and posterior to the posterior cruciate ligament (PCL) and
may be mistaken for meniscal fragments (Fig.) [2].
Page 5 of 40
Fig.: A linear band of increased signal intensity (arrowheads) is noticed on sagittal PDW fat sat images (e, f), between the posterior horn of lateral meniscus and the ligament
of Humphry, simulating a vertical meniscal tear. The anterior meniscofemoral ligament
(arrows) is clearly demonstrated on adjacent sagittal PD-W fat sat images (a-f).
Page 6 of 40
Fig.: The anterior meniscofemoral ligament (arrows) is depicted on adjacent coronal
PD-W fat sat images (g, h) as it courses from the medial aspect of medial femoral
condyle to the medial aspect of the posterior horn of lateral meniscus. A horizontal tear
of the posterior horn of medial meniscus (arrowheads) is also noticed.
Page 7 of 40
Fig.: The ligament of Humphry (arrows) is demonstrated on adjacent axial PD-W fat
sat images (i-l) as it courses from the medial aspect of medial femoral condyle to the
medial aspect of the posterior horn of lateral meniscus.
Page 8 of 40
Fig.: A linear band of increased signal intensity (arrowhead) is noticed on a sagittal
PD-W fat sat image (e), between the posterior horn of lateral meniscus and the
ligament of Wrisberg, simulating a vertical meniscal tear. The posterior meniscofemoral
ligament (arrows) is clearly demonstrated on adjacent sagittal PD-W fat sat images (ae).
Page 9 of 40
Fig.: The ligament of Wrisberg (arrows) is depicted on adjacent coronal PD-W fat
sat images (f, g) as it courses from the medial aspect of medial femoral condyle to
the medial aspect of the posterior horn of lateral meniscus. A horizontal tear of the
posterior horn of medial meniscus (arrowheads) is also noticed.
The medial and lateral oblique menisco-meniscal ligaments have a reported
incidence of 1% to 4% and are an uncommon source of diagnostic difficulty.
These ligaments extend obliquely from the anterior horn of one meniscus to
the posterior horn of the opposite meniscus (Fig.).
Page 10 of 40
Fig.: Diagram showing the medial oblique menisco-meniscal ligament as it
courses from the anterior horn of medial meniscus to the posterior horn of
lateral meniscus.
As the ligament traverses the intercondylar notch, it passes between anterior
cruciate ligament (ACL) and PCL, mimicking the appearance of a "double
PCL sign" (Fig.).
Page 11 of 40
Fig.: Sagittal T1-W (a) and PD-W fat sat images (b) through the intercondylar notch
at the level of PCL demonstrate the medial oblique menisco-meniscal ligament as a
thin linear structure of low signal intensity (arrows) mimicking a displaced meniscal
fragment. A Baker's cyst is also noticed (arrowheads). Coronal PD-W fat sat image (c)
shows the ligament as it passes through the intercondylar notch.
Knowledge of the normal course of these ligaments, as well as the ability to
trace them on consecutive MR images, allows distinction of these ligaments
from a meniscal bucket-handle tear (Fig.) [3].
Page 12 of 40
Fig.: Bucket-handle meniscal tear of medial meniscus. The thin linear structure of low
signal intensity (arrow) which courses under the PCL (arrowheads) on a sagittal T2-W
image (a) represents a displaced meniscal fragment ("double PCL sign"). The meniscal
fragment (arrow) is also demonstrated as it passes through the intercondylar notch
under the PCL (arrowheads) on a coronal PD-W fat sat image (b).
The bursa of the popliteus tendon, which lies close to the posterolateral
meniscus, may also be mistaken for a meniscal tear. Fluid within the bursa
appears as high-signal intensity on T2-weighted MR images and gives the
appearance of a vertical or slightly diagonal tear in the posterior horn of
lateral meniscus (Fig.) [4, 5].
Page 13 of 40
Fig.: Fluid within the bursa (arrowhead) appears as high-signal intensity on a sagittal
PD-W fat sat image (e) and gives the appearance of a vertical or slightly diagonal tear
in the posterior horn of lateral meniscus. The popliteus tendon and bursa (arrows) are
clearly demonstrated on adjacent sagittal PD-W fat sat images (a-e).
Page 14 of 40
Fig.: Fluid within the bursa (arrowhead) appears as high-signal intensity on a coronal
PD-W fat sat image (f) and resembles a vertical or slightly diagonal tear in the posterior
horn of lateral meniscus. The popliteus tendon and bursa (arrows) are demonstrated
on adjacent coronal PD-W fat sat images (f, g).
The lateral inferior genicular artery arises from the popliteal artery at the level
of the tibiofemoral joint and courses laterally to the anterior aspect of the
knee where it and other arteries compose the genicular anastomosis. Unlike
the superior genicular arteries and the inferior medial genicular artery, the
lateral inferior genicular artery is closely applied to the meniscus as it wraps
around the knee, lying in a periarticular fat pad between the meniscus and
lateral collateral ligament (LCL) (Fig.).
Page 15 of 40
Fig.: Diagram showing the arteries of the knee.
When the lateral inferior genicular artery lies immediately adjacent to the
anterior horn of lateral meniscus, the space between the artery and the
meniscus can produce the appearance of a tear in the meniscus on sagittal
images. Comparison with a coronal image through the area of suspected
tear may be helpful since the artery does not mimic a tear when viewed in
the coronal plane (Fig.) [6].
Page 16 of 40
Fig.: Adjacent sagittal T1-W images through the lateral meniscus (a-d) demonstrate
the course of the lateral inferior genicular artery (arrows). A narrow separation
(arrowhead) between the anterior horn of lateral meniscus and the lateral inferior
genicular artery (c) can sometimes be mistaken for a meniscal tear.
NORMAL VARIANTS
In addition to normal meniscal structures previously demonstrated
radiologists should be familiar with several normal variants of the menisci
that have been described in recent years.
Meniscal flounce is an uncommon variant that can simulate meniscal
pathology. It occurs in the absence of a tear and is a single symmetric fold
along the free edge of the meniscus. It is a normal finding that is said to
be present with ligamentous laxity, although it is not necessarily indicative
of a tear in the ligament. The appearance is like that of a carpet that has a
wrinkled edge and, in fact, presumably has a similar cause-that is, sliding
of the tibia on the femur because of ligamentous laxity with resultant folding
or buckling of the inner edge of the meniscus. It has no known significance.
Page 17 of 40
A flounce results in a wavy S-shaped appearance along the free edge of
the meniscus on sagittal images and a truncated meniscal appearance on
coronal images that may be mistaken for a meniscal tear or degeneration
(Fig.) [7].
Fig.: Meniscal flounce of medial meniscus (arrows) which results in a slight wavy Sshaped appearance along the free edge of the meniscus on adjacent sagittal PD-W fat
sat images (a, b).
A speckled appearance of the anterior horn of lateral meniscus is a frequent
finding that has been explained by fibers of the anterior cruciate ligament
inserting into the meniscus. It can be seen on one or two of the most medial
sagittal images. The appearance can be mistaken for a torn lateral meniscus
(Fig.) [8].
Page 18 of 40
Fig.: A speckled appearance (white arrows) of the anterior horn of lateral meniscus
on adjacent sagittal PD-W fat sat images (a, b), which is caused by the insertion of the
fibers of anterior cruciate ligament (black arrow) into the meniscus (c). The finding can
easily be mistaken for a torn lateral meniscus.
A discoid lateral meniscus is a normal variant seen in about 3% of knees.
An uncommon variant of a discoid lateral meniscus is a Wrisberg's variant,
in which the posterior horn is not attached to the capsule and is, therefore,
mobile enough to move freely and sublux into the joint, causing pain and,
occasionally, locking. The MR imaging appearance is a discoid lateral
meniscus with no posterior horn attachment or a free-floating posterior
horn. Unlike the incidental discoid meniscus, which should be asymptomatic
unless torn, a Wrisberg's variant can be a source of pain and require surgery.
It is most commonly found in children, although it can be seen in patients
at any age [9].
The moderate to high signal intensity seen at the normal capsular attachment
of the posterior horn of medial meniscus may be due to tissue inhomogeneity
or peripheral vessels that can mimic a meniscocapsular detachment (Fig.).
Page 19 of 40
Fig.: The high signal intensity seen at the periphery of the posterior horn
of medial meniscus (arrows) on adjacent sagittal (a, b) and coronal PD-W
fat sat images (c) was diagnosed as meniscocapsular detachment. The
following arthroscory for anterior cruciate ligament reconstruction (ACLR),
because of torn ACL, revealed absence of meniscal tear.
Usually, the signal intensity of this normal connective tissue at the
meniscocapsular junction is less conspicuous, whereas in cases of
meniscocapsular detachment, there is markedly increased signal intensity
(Fig.) [10].
Page 20 of 40
Fig.: Peripheral tear-meniscocapsular detachment (arrows) of the posterior horn of
medial meniscus on sagittal (a) and coronal PD-W fat sat images (b). Bone contusions
of the posterior tibial epiphysis are also noticed.
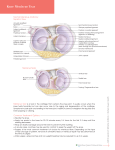
The most significant characteristic in the appearance of pediatric meniscus
is the presence of intrasubstance signal that represents perforating vessels
within the meniscus. This signal has been described in 82% of menisci
in children and is considered to be a normal finding that should not be
misinterpreted as mucinous or myxoid degeneration like in adults. The MR
criteria for establishing the diagnosis of a meniscal tear are the same in
children and adults. The 2 most important criteria are intrameniscal signal
that extends to the surface and abnormal meniscal morphology (Fig.) [11].
Page 21 of 40
Fig.: The presence of intrasubstance signal in the posterior horns of medial (arrows)
and lateral (arrowheads) meniscus represents perforating vessels within the menisci.
This signal is considered a normal finding and should not be misinterpreted as
mucinous or myxoid degeneration like in adults.
MRI ARTIFACTS
MRI artifacts created by the pulse sequences used can result in image
degradation and errors in diagnosis.
The magic angle phenomenon occurs on short TE images in fibers that are
orientated 55° relative to the static magnetic field. This MRI artifact is a cause
of increased signal in the medial segment of the posterior horn of lateral
meniscus. Imaging the knee joint in slight abduction can alter the orientation
of the fibers in the posterolateral meniscus and eliminate this artifact [12].
Partial volume averaging is a type of artifact that occurs when 3-dimensional
volumetric data is used to create a 2-dimensional image. The attachment
of the capsule produces a concavity at the outer margin of the meniscus
Page 22 of 40
that is filled with periarticular fat and neurovascular structures. When the
signal from a normal dark meniscus is averaged with the bright, fatty tissue
adjacent to the outer concave margin of the meniscus, high-signal intensity
linear artifacts that may simulate a tear are created through the periphery of
the meniscus on sagittal images (Fig.).
Fig.: Diagram of the meniscus showing the concave meniscal edge. A
sagittal section through the edge of the meniscus (B) produces a partial
volume averaging linear artifact in the body of the meniscus. A section
located more medially (A) may produce a similar linear artifact in the
anterior and posterior horns when the curvature of the meniscus is placed
at the edge of the section.
This linear defect is seen only on sagittal images obtained through the
periphery of the meniscus. A coronal image obtained through the meniscus
will show no abnormality and can be used to exclude the presence of a tear
(Fig.) [6].
Page 23 of 40
Fig.: Partial volume averaging produces linear artifacts mimicking horizontal tears
(arrows) in the anterior and posterior horns and in the body of lateral meniscus on
adjacent sagittal PD-W fat sat (a-c) and T1-W images (d-f).
Motion artifact can be particularly problematic in MRI because of the
long image acquisition times. If a structure moves to different positions
during image acquisition, the image appears blurred or double exposed.
Intrameniscal signal resembling a tear may result. If motion artifact is present
on an MRI scan and a meniscal tear is suspected by imaging criteria, the
sequence should be repeated without motion (Fig.) [5].
Page 24 of 40
Fig.: Motion artifact mimicking a tear (arrow) in medial meniscus on a coronal PD-W
fat sat image (a). The meniscus appears normal on a coronal T1-W image at the same
level (b), which is obtained without motion.
Truncation error is a type of MRI artifact that occurs at high-contrast
boundaries, such as between the articular cartilage and the menisci.
Truncation artifact is a result of inherent errors in the Fourier transformation
method of image reconstruction. It appears as a series of alternating parallel
bands of bright and dark signal. When a line of high-signal intensity projects
over a low-signal meniscus, a pseudotear is created [13].
VARIOUS PATHOLOGIC CONDITIONS
Certain pathologic conditions of different etiology may mimic a meniscal tear.
Most of them are rare entities and their recognition may help to explain areas
of abnormal signal that do not fit well into previously recognized patterns and
may improve interpretation accuracy.
Page 25 of 40
A meniscal contusion occurs when the meniscus gets trapped between the
tibia and the femur during a traumatic event-usually involving ACL tears.
Increased signal in the periphery of the meniscus can resemble a tear;
however, the signal intensity of a contusion is indistinct and amorphous
rather than sharp and discrete. An adjacent bone contusion should alert one
to the possible presence of a contusion rather than a meniscal tear (Fig.)
[14].
Fig.: Meniscal contusion with amorphous and indistinct signal in the periphery of the
posterior horn of medial meniscus (arrows) on adjacent sagittal (a-c) and coronal PD-W
fat sat images (d-f) after an acute traumatic event with bone contusions, complete ACL
and partial medial collateral ligament (MCL) tear. Follow-up MRI 5 months after initial
imaging revealed resolution of abnormal meniscal signal.
Grade 2C meniscal signal is an extensive triangular or wedge-shaped signal
that does not reach the surface of the meniscus on more than one images on
MRI. It has a low incidence (1,5%) and has been proved to represent a tear
in 50% of cases. Most patients with grade 2C meniscal signal are not treated
Page 26 of 40
with arthroscopy because they do not have symptoms at the site of grade
2C signal. Thus, when grade 2C signal is seen on MR imaging, arthroscopic
follow-up is indicated if symptoms referable to the site of abnormal signal
are also present (Fig) [15].
Fig.: Grade 2C signal in the posterior horn of medial meniscus (arrows) on adjacent
sagittal PD-W (a, b) and coronal PD-W fat sat images (c, d), confirmed as intact
meniscus on arthroscopy.
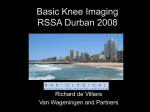
Chondrocalcinosis is defined as a radiographically visible calcification in the
cartilage of a joint. It can occur in the hyaline articular cartilage lining the
articular surface or in the fibrocartilage of a meniscus. Although it can
occur from many types of calcium crystals, the most commonly seen is
from calcium pyrophosphate dihydrate crystal deposition in pseudogout,
which is also known as calcium pyrophosphate dihydrate deposition disease.
When MR imaging is performed on a meniscus with chondrocalcinosis, the
T1-weighted or PD-weighted sequence shows high signal, which can be
mistaken for a meniscal tear. Differentiating a meniscal tear from the high
Page 27 of 40
signal of chondrocalcinosis can be difficult, if not impossible. Most meniscal
tears have a more linear appearance than the globular high signal seen in
chondrocalcinosis. Comparison with a conventional radiograph of the knee
will help avoid this pitfall. However, chondrocalcinosis can also obscure a
tear and result in a false-negative report (Fig) [16, 17].
Fig.: Chondrocalcinosis in medial meniscus. Radiograph of the knee (a) reveals
meniscal calcifications in the posterior horn of the meniscus (arrow). Coronal PD-W (b)
and sagittal PD-W images (c, d) show marked high signal throughout the posterior horn
of medial meniscus (arrows) that resembles a tear. No meniscal tear was identified on
arthroscopy.
Page 28 of 40
Fig.: Chondrocalcinosis in lateral meniscus. Anteroposterior knee radiograph (a)
shows meniscal calcifications in lateral meniscus (arrow). Sagittal PD-W image (b)
shows high signal intensity both in the anterior and posterior horn of lateral meniscus
with extension to inferior articular surface (arrowheads), interpreted as meniscal tears.
No meniscal tear was found on arthroscopy.
Meniscal ossification is a rare finding of unknown origin with a prevalence of
0,15% in MR examinations. Meniscal ossicles are frequently asymptomatic
and discovered incidentally. They mimic intra-articular loose bodies and
lead to inappropriate surgical treatment. Imaging is required to confirm the
diagnosis and assess meniscal integrity. The typical appearance is that of
an intrameniscal lesion which shows central high signal on T1-weighted
images, due to normal fat bone marrow, surrounded by low signal on both
T1-weighted and T2-weighted images related to the cortical rim. The high
signal of the inner portion, which is the same as viable medullary bone,
allows differentiation from loose bodies, which may present internal low
signal. However, loose bodies, if ossified, may present with an internal high
signal [18, 19].
Page 29 of 40
Gas within the knee joint may represent a vacuum phenomenon or iatrogenic
placement during arthrography or joint aspiration. The low magnetic
susceptibility of gas produces a discrete signal void. If the gas collects
adjacent to the meniscus, it can simulate a meniscal tear, abnormal meniscal
volume, or a displaced meniscal fragment (Fig.) [20].
Fig.: Gas within the knee joint (arrows) produces a discrete signal void on adjacent
coronal T2 GRE (a, b) and T1-W images (c, d), as well as on sagittal T2-W images (eg), that simulates a radial meniscal tear in medial meniscus (arrowheads).
Articular cartilage damage is another potentially confounding pathological
condition that can resemble a tear. Articular cartilage defects and chondral
fractures of the tibial, femoral, and patellar cartilage in children may mimic
a bucket-handle meniscal tear on MRI [21].
POSTOPERATIVE CHANGES
Page 30 of 40
In recent years, there has been increasing demand for postoperative
evaluation of the meniscus because of the increased number of patients
who undergo meniscal surgery. The most common surgical procedures
include partial meniscectomy and meniscal repair. Recognition of the normal
postoperative MRI appearance of the meniscus and of abnormalities is
essential for the accurate assessment of symptomatic patients [22].
After partial meniscectomy, meniscal morphology may differ from that of a
nonoperative meniscus with its postoperative appearance depending on
the amount and anatomical location of meniscal tissue resected and the
morphology of the previous meniscal tear. On MR imaging, such postsurgical
variations in meniscal shape typically include diminution in the overall size
of the meniscus or meniscal horns, blunting of the meniscal apical margin,
or variable degrees of meniscal truncation (Fig.) [23].
Fig.: Diagram of medial meniscus (a) illustrating the two types of partial
meniscectomy: circumferential (b)-where the posterior horn and anchor, and therefore
Page 31 of 40
the meniscal "hoop" has been preserved and segmental (c)-where the posterior
attachment has been resected and the load transmitting function has been sacrificed.
Fig.: Normal appearance of a partially resected meniscus. Adjacent coronal PD-W fat
sat images from anterior to posterior (a-c) demonstrate a small blunted body of medial
meniscus (arrow) following circumferential partial meniscectomy.
Page 32 of 40
Fig.: Normal appearance of a partially resected meniscus. Adjacent coronal PD-W fat
sat images from anterior to posterior (a-c) demonstrate a resected posterior horn of
medial meniscus (arrows) following segmental partial meniscectomy.
Increased short TE intrameniscal signal extending to the meniscal articular
surface after the operation may also be seen as a normal finding on MR
imaging and may not be indicative of a recurrent tear (Fig.) [24].
Page 33 of 40
Fig.: Diagram illustrating the potential of creating an intrasubstance grade 3 signal
intensity abnormality after meniscectomy. The dotted lines (a) show the planned
incision in a torn meniscus. The surgeon resects the torn portion of the virgin meniscus
after probing it. The resected fragment usually does not contain the entire linear area
of abnormal signal intensity (straight line) seen on MRI. A grade 3 signal intensity
abnormality extends to the articular surface after the operation (b) and mimics a tear in
the untorn postoperative meniscus.
Page 34 of 40
Fig.: Diminutive morphology of the posterior horn of medial meniscus on adjacent
coronal PD-W fat sat (a, b) and sagittal PD-W images (c, d) following prior
meniscectomy with intrameniscal increased signal intensity extending to the
inferior meniscal surface (arrows), which was interpreted as new tear. Second-look
arthroscopic evaluation revealed an intact meniscus.
Page 35 of 40
Fig.: Intrameniscal increased signal intensity (arrows) on adjacent coronal PD-W
fat sat (a-c) and sagittal PD-W images (d, e) in the resected posterior horn of medial
meniscus after partial meniscectomy was interpreted as new tear. Second-look
arthroscopy revealed normal signal postoperative changes.
What is more, studies on meniscal repair have shown that linear increased
signal intensity extending to the surface, which is indicative of healing
process, can persist at the site of surgery for at least 1 year after repair (Fig.)
[22].
Page 36 of 40
Fig.: Coronal PD-W fat sat image demonstrates linear increased signal
(but not synovial fluid) (arrow) corresponding to a scar mimicking a new
tear, 2 years after repair of a peripheral vertical tear in lateral meniscus.
Thus, diagnosis of meniscal tears by using the usual criterion of linear
increased signal intensity extending to the surface on conventional short
echo time MR images may lead to a false-positive diagnosis in patients after
meniscal repair. Use of the stricter criterion of fluid signal intensity within a
linear defect in the meniscus on T2-weighted images has been shown to
provide high specificity (88%-92%) but low sensitivity (41%-69%) for tears.
Thus, the use of this stricter criterion with conventional MR imaging will result
in fewer false-positive diagnoses; however, many tears will be missed [25].
For patients who have undergone partial meniscectomy, the accuracy of
conventional MR imaging for detection of a tear is 66%-82%. Studies
have shown accuracy similar to that found for evaluation of preoperative
menisci in cases when only a small resection (less than 25%) is performed.
Unfortunately, most resections are not small [25].
In an attempt to improve the accuracy of MR imaging for diagnosing retorn
menisci, the use of direct MR arthrography, which involves the injection
of intraarticular contrast material, has been proposed. MR arthrography
is approximately 90% sensitive and specific for detecting retear of the
postoperative meniscus. Advantages of MR arthrography over conventional
MR imaging include the ability to obtain adequate joint distension, greater
Page 37 of 40
penetration of contrast material and the ability to use T1-weighted images.
On MR arthrograms, meniscal tears are diagnosed as areas of increased
signal intensity (equal to that of intraarticular gadolinium contrast material)
within the meniscus (Fig.) [26, 27].
Fig.: Sagittal T1-W fat-sat MR arthrography image following intra-articular injection of
gadolinium demonstrates contrast extending into a subtle cleft (arrow) in the posterior
horn of medial meniscus corresponding to a peripheral vertical tear, which was
previously missed on conventional MRI.
Conclusion
MRI is a valuable tool for the evaluation of meniscal pathology. A thorough knowledge
of potential pitfalls mimicking meniscal tears is essential if one is to maximize diagnostic
accuracy.
Page 38 of 40
Personal Information
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Aydmgöz Ü, Kaya A, Atay ÖA, et al. MR imaging of the anterior intermeniscal ligament:
classification according to insertion sites. Eur Radiol 2002; 12:824-829.
Lee BY, Jee WH, Kim JM, et al. Incidence and significance of demonstrating the
meniscofemoral ligament on MRI. The British Journal of Radiology 2000; 73:271-274.
Sanders TG, Linares RC, Lawhorn KW, et al. Oblique meniscomeniscal ligament: another
potential pitfall for a meniscal tear-anatomic description and appearance at MR imaging in
three cases. Radiology 1999; 213:213-216.
Watanabe AT, Carter BC, Teitelbaum GP, et al. Normal variations in MR imaging of the
knee: appearance and frequency. AJR 1989; 153:341-344.
Sanders TG, Fults-Ganey KA. Magnetic resonance imaging of knee menisci: diagnostic
interpretation and pitfalls. Operative Techniques in Orthopaedics 2000; 10:169-182.
Herman LJ, Beltran J. Pitfalls in MR imaging of the knee. Radiology 1988; 167:775-781.
Park JS, Ryu KN, Yoon KH. Meniscal flounce on knee MRI: correlation with meniscal
locations after positional changes. AJR 2006; 187:364-370.
Shankman S, Beltran J, Melamed E, Rosenberg ZS. Anterior horn of the lateral meniscus:
another potential pitfall in MR imaging of the knee. Radiology 1997; 204:181-184.
Helms CA. The meniscus: recent advances in MR imaging of the knee. AJR 2002;
179:1115-1122.
Rubin DA, Britton CA, Towers JD, Harner CD. Are MR imaging signs of meniscocapsular
separation valid? Radiology 1996; 201: 829-836.
King SJ, Carty HML, Brady O. Magnetic resonance imaging of the knee injuries in children.
Pediatr Radiol 1996; 26:287-290.
Peterfy CG, Janzen DL, Tirman PFJ, et al. "Magic-angle" phenomenon: a cause of
increased signal in the normal lateral meniscus on short-TE MR images of the knee. AJR
1994; 163:149-154.
Turner DA, Rapoport MI, Erwin WD, et al. Truncation artifact: a potential pitfall in MR
imaging of the menisci of the knee. Radiology 1991; 179:629-633.
Cothran RL, Major NM, Helms CA, Higgins LD. MR imaging of meniscal contusion in the
knee. AJR 2001; 177:1189-1192.
McCauley TR, Jee W-H, Galloway MT, et al. Grade 2C signal in the meniscus on MR
imaging of the knee. AJR 2002; 179:645-648.
Burke BJ, Escobedo EM, Wilson AJ, Hunter JC. Chondrocalcinosis mimicking a meniscal
tear on MR imaging. AJR 1998; 170:69-70.
Kaushik S, Erickson JK, Palmer WE, et al. Effect of chondrocalcinosis on the MR imaging of
knee menisci. AJR 2001; 177:905-909.
Schnarkowski P, Tirman PF, Fuchigami KD, et al. Meniscal ossicle: radiographic and MR
imaging findings. Radiology 1995; 196:47-50.
Martinoli C, Bianchi S, Spadola L, Garcia J. Multimodality imaging assessment of meniscal
ossicle. Skeletal Radiol 2000; 29:481-484.
Page 39 of 40
20. Shogry MEC, Pope TL. Vacuum phenomenon simulating meniscal or cartilaginous injury of
the knee at MR imaging. Radiology 1991; 180:513-515.
21. Kim CW, Jaramillo D, Hresko MT. MRI demonstration of occult purely chondral fractures of
the tibia: A potential mimic of meniscal tears. Pediatr Radiol 1997; 27:765-766.
22. McCauley TR. MR Imaging evaluation of the postoperative knee. Radiology 2005;
23.
24.
25.
26.
27.
234:53-61.
Recht MP, Kramer J. MR imaging of the postoperative knee: a pictorial essay.
RadioGraphics 2002; 22:765-774.
Toms AP, White LM, Marshall TJ, Donell ST. Imaging the post-operative meniscus.
European Journal of Radiology 2005; 54:189-198.
Lim PS, Schweitzer ME, Bhatia M, et al. Repeat tear of the postoperative meniscus:
potential MR imaging signs. Radiology 1999; 210:183-188.
White LM, Schweitzer ME, Weishaupt D, et al. Diagnosis of recurrent meniscal tears:
prospective evaluation of conventional MR imaging, indirect MR arthrography, and direct
MR arthrography. Radiology 2002; 222:421-429.
Sanders TG, Miller MD. A systematic approach to magnetic resonance imaging
interpretation of sports medicine injuries of the knee. The American Journal of Sports
Medicine 2005; 33:131-148.
Page 40 of 40