Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
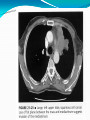
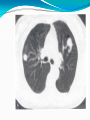
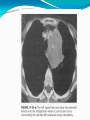
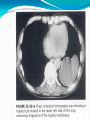
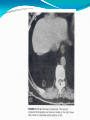
Tomasz Szczęsny, MD, PhD Janusz Kowalewski, MD, PhD Department and Clinic of Thoracic Surgery Faculty of Medicine Nicolaus Copernicus University in Toruń Lung cancer invading vertebral body Mediastinal Schwannoma Thymoma? Hodgkin Lymphoma? Non-Hodgkin Lymphoma? Yolk sac tumour? Other? Pre-invasinve lung cancer Disseminated cystadenocarcinoma Clinical features, diagnosis and treatment Neuroendocrine tumours Warren and Gould classification Typical carcinoid (TC) Atypical carcinoid (ATC) Large cell neuroendocrine carcinoma (LCNEC) Small cell lung cancer (SCLC) Typical carcinoid Mitotic index < 2/10 HPF No necrotic focuses Any age (max 60<x<70) Cushing and carcinoid syndrome Good prognosis: OS 5 y. – 90-98% 10 y. – 82-95% Atypical carcinoid Mitotic index < 2-10/10 HPF Necrotic focuses Peripheral location Poorer prognosis than TC: OS 5 y. – 61-73% 10 y. – 35-59% Large cell neuroendocrine carcinoma (LCNEC) Cytological features like in NSCLC (nucleolus) Mitotic index >10/10 HPF + necrosis Older age, advanced stage. Poor prognosis, similar to SCLC. Carcinoid: central location Main, lobar or segmental bronchus, Cough, hemoptysis, wheezing, Recurrent pneumonia, Dyspnoea, Cushing syndrome. Carcinoid: peripheral location Lung parenchyma, Asymptomatic course. Carcinoid syndrome Secondary to carcinoid tumour (rare: 1/10) Serotonin, kallicrein Big tumour, distant metastases (liver), Flushing, Heart failure, diarrhea, Bronchoconstriction. , Carcinoid: treatment 1. Surgical treatment Typical carcinoid Radical anatomical resection (lobectomy, segmentectomy, wedge resecton). Bronchoplastic procedures. Laser therapy (ablation, cautery). Atypical carcinoid The same like NSCLC Carcinoid: treatment 2. Radiotherapy Efficacy of radical and paliative radiotherapy has not been proven yet. Carcinoid: treatment 3. Chemotherapy. Cisplatin, etoposide, cyclophosphamide, doxorubicin, vincristine. Low chemosensitivity. Partial response (PR) 10-20% - only AC Mean Survival Time = several months. Benign pulmonary neoplasms: 1. Hamartoma, 2. Cylindroma, 3. Fibroma, 4. Chondroma, 5. Fibroneuroma, 6. Cystadenoma, 7. Lipoma. Bronchial lipoma Solitary pulmonary nodule SPN - definition Round or oval, Central or peripheral, Smaller than 3 cm in diameter, No pleural effusion, thoracic wall or mediastinum invasion, lymph nodes enlargement. SPN: statistics 1. Primary lung cancer: 2. Tuberculoma: 35%, 23%, 3. Hamartoma: 14%, 4. Other benign ndules: 13%, 5. Metastasis: 8%, 6. Inflammatory nodules: 7%. Solitary Pulmonary Nodule: benign or malignant ? Age (<30 b., > 50 =% m.) Diameter: 2-3 cm – mostly malignant, ≤ 0,5cm – mostly benign (observation), 0,6-1,9 cm ??? Calcifications. Margins. Stability. Computed tomography - CT CT – enhancement Benign lesions: average 12 HU, Malignant lesions: average 40 HU, 20 HU – threshold of malignancy 100% sensitivity, 77% specificity, 93% accuracy. Radiology 2009; 194; 393-98 Positron Emission Tomography PET - CT Sensitivity for malignant lesions: 0,9 Sensitivity for benign lesions : 0,72 Eur. J. Cardiothorac. Surg.: 2001; 20; 324-29 Solitary Pulmonary Nodule: treatment Surgical treatment (complete resection) ? 1. If surgery: - thoracotomy or VT ? - how to find a nodule during VT ? - what type of resection if you detect NSCLC ? 2. If no surgery, what next ? - no further follow up ? - follow up (what kind of folow up ?) - FNAB, bronchoscopy, PET-CT (cost, safety?). Treatment of SPN depends on: 1. Risk of surgical procedure. 2. Probability of malignancy. 3. Well informed patient’s opinion. 4. Capabilities of the unit (hospital). Approximate probability of malignancy p Clinical and radiological characteristics Low (< 5%) Moderate (5%-65%) High (>65%) Young age, No smoker, No previous malig., Small nodule, Smooth edge, Lower or meedle lobe. Combination of the Older age, characteristics from Smoker, both groups Previous cancer, Big nodule, Irregular (rugged) edge Upper lobe. Exact probability of malignancy P = x = - 6.8272 + (0.0391 x age) + (0.7917 x smoking) + (1.3388 x previous malign) + (0.1274 x diameter) + (1.0407 x rugged edge) + (0.7838 x upper lobe) e base of natural logarithm = 2.72. N Engl J Med. 2011; 365(5): 395-409. Thorax 2012; 67(4): 296-301. Exact probability of malignancy P = x = - 6.8272 + (0.0391 x 70) + (0.7917 x 1) + (1.3388 x 1) + (0.1274 x 20) + (1.0407 x 1) + (0.7838 x 1) = 2.413 e= 2.72; x= 2.413; P = 0.917 = 92% 58 y. female smoker, no history of malignancy, good general condition, diameter of the nodule 12 mm. A. CT scan after 6 mths. B. PET - CT C. FNAB. D. Resection. E. Others. PET-CT was performed: SUV 6,7 A. CT scan after 6 mths. B. FNAB. C. Resections. D. Others. Solitary pulmonary nodule in patient with malignancy. Problem for the doctor and for... the patient Exact staging of the disease, - metastases ? Correct strategy of cancer treatment. Prognosis ? Solitary pulmonary nodule in patient with malignancy 70% metastasis. 20% benign lesion. 9% primary lung cancer. 1% metastasis of unknown cancer. Pulmonary metastases (PM) In 30% of cancer patients PM occur. Pulmonary Metastases Hematogenous way: Brest cancer, Sarcomas, Genitourinary tumours, Colon cancer. Pulmonary Metastases Air way: Laryngeal cancer, Tracheal cancer, Bronchioalveolar carcinoma. PM - diagnosis Accidental 80-90% cases, - Chest X-Ray, - Often the first sign of extrapulmonary neoplasm PM - classification I: Time synchronous, metachronous, II: Number single, multiple, unilateral, bilateral. Pulmonary Metastases Is it justified to perform radical metastasectomy or it is useless. Selection of patients for pulmonary resection The primary tumour is controlled or is controllable, No extrapulmonary tumour exists, No better method of proven treatment value is available, Adequate medical status for the planned resection exists, Complete resection is possible on CT (PET) scan evaluation. Long DFI . Dtsch Arztebl Int 2012; 109(40): 645-51 P.M. Wedge resection, Anatomical resections, segmentectomy, lobektomy, pneumonectomy Approach for bilateral lesins? History Weinlechner J. Wien Med Wochenschir 1882; 32: 598-591. Resection of two metastatic lesions accidentally detected during operation of sarcoma of the thoracic wall. History Divis G. Acta Chir Scand 1927; 62: 329-334. The first planned resection of pulmonary metastases Right lung metastasis (CT, PET) Surgical approach Sternotomy, clamshell, thoracotomy, VT/VATS: - Thoracotomy or VATS ? - How to find a nodule during VATS ? Clamshell incision Thoracotomy or VATS How to find a nodule ? Palpation, Hook wires, Metalic coils, Itraoperative ultrasound, Image-guided stereotactic navigation, Technetium radiotracer scintigraphy. Clinics in Colon and Rectal Surgery 2009; 22(4):233-41 Metalic coils and hook wire Wedge resections Reinforced wedge resection Laser resection P.M: Breast cancer Very good response to chemotherapy, but: Precise diagnosis of pulmonary nodules ??? In 50% of breast cancer patients new pulmonary nodule is a primary lung cancer (DFI>3 years). Hormons’ receptor status. P.M: Colon cancer 50% of patients with PM develope liver metastases. Different approaches: liver –lung, lung-liver, simultaneous procedure ? Poor prognosis if: nodal involvement, CEA elevation. P.M: Sarcomas Isolated PM very often. Recurrent PM very often. Chemoresistance. Complete resection: strong prognostic factor. Chemotherapy alone – poor prognosis. Multidiscyplinary approach is essential. P.M: Malignant malanoma Isolated p.m. very rare. Complete resection questionable. Mean survival time : 6 mths. 5 years OS : 5%. Resection of P.M: effectiveness. (Munich score): 202 patients with renal cancer Complete resection: 87%. Median survival time: 43 msc. Poor prognostic factors (multivariate analysis): - incomplete resection, - diameter of the lesion (s) > 3 cm, - nodal involvement detected during nephrectomy, - synchronous metastases, - pleural infiltration, - hilar and mediastinal lymph nodesinvolvement. The American Journal of Surgery 2011; 202: 158-67. Alternative methods SBRT: Stereotactic Body Radiation Therapy RFA: Radiofrequency Ablation Microwave Ablation Cryoablation RFA: Radiofrequency Ablation Take home message 1. Complete resection of PM is an effective method of treatment. 2. The most important prognostic factors are: type of primary tumour and complete PM resection. 3. Multidisciplinary approach is essential.