Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
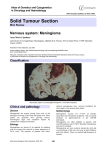
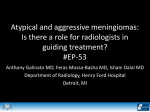
Tentorial Meningiomas Meningiomas of the posterior cranial fossa account for ~9% of all intracranial meningiomas. Approximately 3 to 6% of all intracranial meningiomas and ~30% of posterior fossa meningiomas originate from the tentorium cerebelli. Classification 1)Meningiomas arising from the free tentorial notch(T1-T2) anterior middle posterior 2)Meningiomas originating from the intermediate tentorial surface(T4) 3)Meningiomas involving the torcular Herophili(T5) 4)Meningiomas arising from the lateral outer tentorial ring(T6-T7) posterior anterior 5) falcotentorial meningiomas(T3-T8) Superior Petrosal Sinus 1 5 Transverse Sinus 2 3 4 Straight Sinus The straight sinus receives the vein of Galen and the inferior sagittal sinus at the tentorial apex and runs posteriorly to meet the transverse sinuses from both sides and the superior sagittal sinus from above at the torcular Herophili. The tentorial incisura is divided into an anterior incisural space located in front of the brain stem, a middle incisural space situated lateral to the brain stem, and a posterior incisural space located behind the brain stem At the anterior incisural space, the most important neurovascular structures in close proximity include the oculomotor nerve, the basal vein, the posterior communicating artery, the anterior choroidal artery, the P1 and proximal P2 segments of the posterior cerebral artery, and the superior cerebellar artery. Less often, the optic nerve and the optic chiasm may be involved. The trochlear nerve, the anterior choroidal artery, the P2 segment of the posterior cerebral artery, the superior cerebellar artery, and the basilar vein constitute the neurovascular contents of the middle incisural space. The ambient cistern continues posteriorly into the quadrigeminal cistern, which is the main cistern of the posterior incisural space. This space forms the pineal region and is related to anterior falcotentorial meningiomas. It contains the trunks and branches of the posterior cerebral and superior cerebellar arteries, and the vein of Galen, which receives the paired internal cerebral and basal veins. The trochlear nerve exits from below the inferior colliculi, curves around the dorsal midbrain, and enters the ambient cistern in the middle incisural space Clinical Presentation Patients harboring a infratentorial meningioma, the most often encountered subtype, commonly present with headache, dizziness and gait unsteadiness. Clinical examination usually reveals a gait ataxia and occasionally impairment of the vestibulocochlear nerve. Hearing loss may be caused by direct involvement of the eighth cranial nerve (CN), or it may be the result of distortion of the central auditory pathways, such as the lateral lemniscus or the inferior colliculi. Supratentorial meningiomas, particularly those closely related to the medial temporal lobe, may present with seizures. T1–T2 meningiomas may intimately involve the brain stem and the fifth CN. Accordingly, patients may present with hemiparesis, trigeminal neuralgia, and facial numbness Patients with T3–T8 meningiomas often present with headache. Mental changes are reported in up to 46% of patients and a gait ataxia in 43 to 62% of cases. A homonymous hemianopsia is present in 20 to 46% of these patients. Diagnostic Workup and Preoperative Considerations Triplanar contrast-enhanced T1-weighted MRI gives the most accurate information for planning the surgical approach. The dural attachment zone and extent of the tumor, displacement of the brain stem, displacement or engulfment of vertebrobasilar arteries, invasion of the cavernous sinus, and patency of the straight, transverse, and sigmoid sinuses can be sufficiently studied. A nonvisible venous sinus on MRV(magnetic resonance venography) or catheter angiography may prove to be patent during surgery. Surgical Approach The lateral suboccipital retrosigmoid approach is suitable for most infratentorial T1–T2 and T6–T7 tumors The supracerebellar infratentorial route may be more appropriate in more medial infratentorial T1–T2 tumors and in infratentorial T3–T8 tumors, and it is the approach of choice in infratentorial T4 tumors The usual avenue for resection of T3–T8 meningiomas is the occipital transtentorial approach Supratentorial T1–T2 and T6–T7 tumors can usually be resected via a subtemporal route. Clinical case 1 Preoperative T1-weighted contrast-enhanced magnetic resonance imaging (MRI) in the axial and coronal plane demonstrates an infratentorial T6–T7 meningioma in a patient with gait unsteadiness and rightsided impairment of hearing. Note patency of the transverse sinus (white arrow) Before Intraoperative photograph after resection of the tumor via a retromastoid craniotomy. Note the trochlear nerve (white arrow) as viewed through the tentorial incisura. Also shown are the cerebellum (black asterisk), hyperemic tentorium after tumor resection (white asterisk), and surgical cotton (black plus sign). After Postoperative T1-weighted contrast-enhanced MRI shows unintended occlusion of the transverse sinus in the axial view (white arrow) and contrast enhancement of the hyperemic tentorium. In the coronal view (white arrow). Occlusion of the venous sinus was without sequelae, and preoperative symptoms and signs, including hearing impairment, resolved Clinical case 2 T3–T8 meningioma displayed in preoperative sagittal contrast-enhanced T1-weighted magnetic resonance imaging (MRI) in a patient presenting with gait ataxia and slight mental deficits. Note the patency of the straight sinus and accompanying obstructive hydrocephalus due to occlusion of the aqueduct Before An intraoperative photograph shows the tumor as viewed via the supracerebellar infratentorial approach. After A second intraoperative photograph reveals the pineal region above the cerebellum (black arrows) and below the tentorium (black asterisk) after resection of the meningioma. Three months postoperative sagittal contrast-enhanced T1-weighted MRI demonstrates removal of tumor. Note patency of the aqueduct, straight sinus, inferior sagittal sinus, vein of Galen, and internal cerebral veins. Obstructive hydrocephalus and preoperative neurological symptoms resolved. Literature: Thieme-Al-Mefty’s Meningiomas- page(168-176)