Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
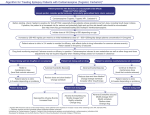
STATUS EPILEPTICUS (INVESTIGATION & MANAGEMENT) Presented By: Dr. Dennis Prabhu Dayal Investigations in Status Epilepticus Initial studies Blood glucose, electrolytes (sodium, potassium, calcium, magnesium),urea Arterial blood gases Anticonvulsant drug levels Full blood count Urinalysis Further investigations after stabilization Liver function tests,lactate,creatine kinase Toxicology Screen Lumbar puncture Electroencephalogram Brain imaging with computed tomography or magnetic resonance imaging Protocol for Management of SE Assess A,B,C,GCS Give O2 and consider need for intubation/ventilation Monitor blood pressure, ECG, Pulse Oximetry Obtain I.V. access and draw blood for investigations If patient is hypoglycemic or if blood glucose estimation is not available give glucose: adults: give thiamine100mg I.V. and 50ml of 50% glucose I.V. Seizure control: A. Give benzodiazepine, for example: Diazepam: 0.2 mg/kg , I.V. at 5 mg/min up to total dose of 20 mg. Lorazepam: 0.1 mg/kg, I.V. at 2 mg/min up to total dose of 10 mg. Clonazepam: 0.01–0.02 mg/kg, I.V. at 0.5 mg/min up to total dose of 4mg. If diazepam stops the seizures, phenytoin should be given next to prevent recurrence. Repeat dose every 2–5 min if required. B. If seizures persist, give Phenytoin: Phenytoin: 15–20mg/kg (adults ≤50mg/min) (children ≤1mg/kg/min) or Fosphenytoin: 15–20 pheny- toin equivalents (PE) mg/kg, I.V. (adults ≤150mg/ min) (children ≤3mg/kg per min). Additional doses of 5 mg/kg I.V. to a maximum dose of 30mg/kg can be given for persistent seizures. Monitor blood pressure and the ECG during infusion. If hypotension or arrhythmias develop, stop or slow the rate of the infusion. C. If seizures persist (refractory SE), intubate and ventilate patient. Give either: Thiopental: Slow bolus 3–5 mg/kg, I.V. followed by infusion 1– 5mg/kg per hour Propofol : slow bolus 1–2mg/kg , I.V. followed by infusion 2– 5mg/kg per hour Midazolam: slow bolus 0.1 – 0.2 mg/kg followed by infusion 0.1 – 1.0mg/kg/h Titrate doses based on clinical and electrographic evidence of seizures, targeting electrographic suppression of seizures or EEG background suppression (isoelectric). Monitor BP and maintain normotension by reducing infusion rate and/or giving fluids/ pressor agents. D. Insert nasogastric tube and administer usual anti-convulsant medications if patient is receiving treatment for pre-existing epilepsy. E. Beware of ongoing unrecognized seizures. Use EEG monitoring until seizures are controlled and then for 1–2 hours after seizures stop. Continue to monitor the EEG continuously, or for periods of more than 30 minutes every 2 hours, during the maintenance phase. Avoid muscle relaxants (use continuous EEG if giving repeated doses of muscle relaxants). F. Discontinue Midazolam or Thiopental, or start reducing Propofol, approximately 12 hours after resolution of seizures. Use continuous EEG monitoring and observe for further clinical and/or electrographic seizure activity. If seizures recur, reinstate the infusion and repeat this step at 12–24-hour intervals or longer if the patient’s seizures remain refractory. OTHER AGENTS OF POTENTIAL USE IN REFRACTORY SE Ketamine acts as an antagonist at the NMDA receptor and may have a role in the treatment of prolonged refractory SE. Intravenous lacosamide is a new anticonvulsant drug available in intravenous and oral formulations that may be an option for treatment of established SE after failure of standard therapy, or when standard agents are considered unsuitable. Pregabalin appears to be an interesting option as add-on treatment in refractory NCSE and may lessen the requirement for ICU treatment. Magnesium is the drug of choice in eclamptic seizures and also is effective in seizures due to hypomagnesaemia, but there is little evidence to support its use in other forms of SE SURGERY Surgery has occasionally been used in refractory SE with procedures based on standard epilepsy surgery techniques. Some success has been reported with focal resections, subpial transection, corpus callosotomy, hemispherectomy and vagus nerve stimulation. INTENSIVE CARE MONITORING Monitoring using ECG, intra-arterial and central venous catheters, capnography and pulse oximetry should be considered in patients with, or at risk of, cardio respiratory compromise. Indications for EEG monitoring: Refractory SE, to aid the titration of anticonvulsant anesthetic drugs (minimizing dose and toxicity) and ensure suppression of seizure activity. Patients receiving neuromuscular blockade. Patients who continue to have a poor conscious state after apparent cessation of seizures. Suspected non-convulsive status epilepticus in a patient with an altered conscious state. Suspected Pseudoseizures OUTCOME The prognosis of patients with SE is related to age, aetiology, degree of impairment of consciousness at presentation, and duration of SE. Refractory SE is associated with a worse prognosis and very prolonged ‘super-refractory’ SE an even higher mortality. However, where no underlying irreversible brain damage is present, good recovery is possible even after weeks of SE. Children have a much lower mortality of 3% whereas those aged over 65 years have a mortality rate of 30%. THANK YOU !!