Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
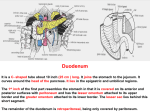
Activity Think back to your Dietetic Internship. What was one of the most humbling and potentially embarrassing moments? In a few words, write this moment on a piece of paper, do not put your name on the paper (this will remain anonymous) Fold the paper and place it in front of you when you are finished Nutritional Implications of Superior Mesenteric Artery Syndrome Meghan Zook Sodexo Dietetic Intern Definition of SMAS Uncommon and potentially fatal cause of small bowel obstruction Occurs when the 3rd portion of the duodenum becomes closed off due to external pressure from the Superior Mesenteric Artery and the Aortic Artery Occurs in 0.013%-0.3% of the general population Occurs in mainly youth and young and slender females Pathophysiology In a normal adult, the SMA leaves the Aortic artery at the location of the first lumbar vertebra This creates an angle in which the duodenum passes through Duodenum is fixed at this point by the ligament of Treitz Angle normally is 25-60 degrees* *no exact definition of what angle is considered “normal” SMA Mesenteric fat pad 3rd portion of the duodenum Aorta Pathophysiology cont. Pathophysiology cont. Symptoms of SMAS begin to occur when the angle is reduced to approx. <25 degrees Symptoms are due to mechanical compression of the duodenum, not from ischemic insult Pathophysiology cont. Anatomic reasons Abnormally short ligament of Trietz Superior mesenteric artery with unusually low origin Loss of mesenteric fat pad Eating disorders Tube-feeding-dependent patients who are underfed Excessive exercise Gastric bypass surgery Wasting/malabsorption diseases Post-surgical External compression Spinal correction surgery Abdominal surgery Trauma Abdominal trauma Spinal cord injury Local pathology Malignancy Aortic aneurysm Chronic inflammation and adhesions Other names Wilkie’s Syndrome Nutcracker Syndrome Cast syndrome Chronic Duodenal Ileus History of SMAS Carl von Rokitansky in 1861 Series of autopsies on thin young women All had post-prandial pain and vomiting Under-studied until 1927 D. P. Wilkie performed first original research 75 patients Similar symptoms Early Research Further research has remained slim Limited number of diagnosed cases Between 1800s and 1985 – 400 cases Most were children and females Pre-existing conditions: disordered eating patterns, cancer, other wasting diseases Controversy existed due to questions about pathology and methods used to diagnose Current Research Body of literature has begun to grow 13 articles 9 case reports (bulk of the literature) 4 observational research studies (multiple patients) 2 studies of pediatric patients Patient Population 67 patients total 47 of these were female (70%) Mean age of 26.77 years Past Medical History Included: Intentional dieting (2) Tuberculosis interstitial nephritis (1) Traumatic paraplegia (1) Appendicular perforation (1) Mild COPD, repair of perforated duodenal ulcer (1) Several years of disordered eating (3) Other psychosocial issues Drug/alcohol abuse (2) Domestic abuse (1) *several articles only listed symptoms and not past medical history Disordered Eating Patients 21-year old Japanese female 2 years bulimia nervosa, 6 years anorexia nervosa – vomiting 1-2x per day 47-year old female “many-year” history of anorexia nervosa Laxative use and excessive exercise 15-year old girl History of anorexia nervosa Presenting Symptoms Post-prandial pain and discomfort Bilious emesis Anorexia Weight loss Diagnostic Tests Barium upper GI studies – “Gold Standard” Small bowel follow through and Doppler blood flow assessment Abdominal ultrasounds CT scans Discern the degree between the SMA and Aortic Artery, fat, and dilation of stomach and 1st and 2nd part of the duodenum Abdominal Ultrasound CT Scan Barium Upper GI Series Misdiagnosed Persons Several individuals were first misdiagnosed Reflux disease Treated with Proton-Pump Inhibitors Other possible misdiagnoses: Peptic ulcer disease Gall bladder disease IBS Duodenitis Cholelithiasis Visceral neuropathy Pancreatitis Gastroparesis Treatment Options Conservative – goal is to increase mesenteric fat pad, all patients except 4 were first conservatively treated Aggressive – surgical relief Depends on medical staff and surgeon Depends on acute vs. chronic SMAS Conservatively Treated Length of treatment 4 days to several weeks 1 study by-passed conservative treatment completely (4) Nasogastric decompression Parenteral & Enteral Nutrition Positioning patient during meals Parenteral & Enteral Nutrition Goal: Avoid re-feeding syndrome Provide enough nutrition for weight gain and to build up the mesenteric fat pad Total Parenteral Nutrition Advised May run with Enteral Nutrition NJ tube treaded past the point of decompression PN and EN Recommendations No recommendations through ASPEN 1 study, 1 patient (70 Y.O. man) – Chan et al. Bolus feeds through NJ tube – Ensure by Nestle 50 mL Q4 hours, increased gradually to 250 mL Study took place in Singapore *ASPEN recommends continuous feeds if feeding into the duodenum Use clinical judgment and nutritional status of the patient to determine appropriate calorie and protein needs Fluids and Soft Foods 1 study, 1 patient (47 Y.O female with anorexia nervosa) – Mascolo et al. Small and frequent liquids Sitting in knee-chest positioning On CT scan, this patient was found to have only partial compression of the duodenum Patient improved and was able to slowly advance her diet Positioning After meals Knee-chest position Left side lying Medications Controversy over whether or not certain medications should be given during conservative treatment Medications to increase gastric emptying (Metoclopramide) Dangerous? Several reviewed articles used metoclopramide and anti-emetic Successful conservative treatment outcomes No recommended regimen for medication Aggressively Treated Normally follows period of conservative treatment 67 patients Conservative Treatment successful for 56% If patient does not gain weight and continues to be unable to eat or drink foods, surgery is recommended Surgical Procedures Strong’s Procedure (3) Gastrojejunostomy (1) Open or Laparoscopic Duodenojejunostomy (13) Gold Standard Strong’s Procedure Mobilization by division of the ligament of Treitz Preoperative gastric decompression with NG tube Dissection allows the 3rd portion of the duodenum to drop lower, relieving pressure 25% rate of failure Gastrojejunostomy Open or Laparoscopic Duodenojejunostomy Recovery Many patients will require help for existing or developed disordered eating patterns Chan et al (27 pediatric patients, 8 male) 21 conservatively treated 14 good recovery within 10-13 weeks 6 underwent surgery (type not listed) 5 had successful surgeries 1 female developed adhesion ileus and needed TPN for 3 weeks until the ileus had resolved Recovery cont. Shin et al (18 pediatric patients, 11 male) 13 responded to conservative treatment (4 recurrences, 3 recovered again, 1 did not - anorexia nervosa - and was lost to follow-up) 1 female with anorexia nervosa responded to laparoscopic gastrojejunostomy and symptoms were relieved within 2 weeks Others were lost to follow-up Role of the Clinical Dietitian Perform assessment to obtain patient nutritional status upon patient admission – document degree of malnutrition Work with medical team to give opinion as to whether or not patient is able to be conservatively treated or if patient requires immediate surgical attention If conservative treatment is an option, prescribe calories and protein and take care to avoid re-feeding syndrome Try to increase patient nutritional status as soon as possible Use clinical judgment to decide upon enteral formula and feeding rate Conclusions Body of literature leaves much to be desired Specifically in regards to feeding recommendations More original research on large groups of subjects Less focus on case reports Hopefully in the future we will see recommendations for formula type and how long to conservatively treat Quiz Time! 1. What are the two arteries that are responsible for compression of the duodenum during SMAS? 2. What is the name of the surgical procedure that is considered the “Gold Standard” used to treat SMAS? 3. List something that you did not know before this presentation. Questions? References Baltazar, U., Dunn, J., Floresguerra, C., Schmidt, L., & Browder, W. (2000). Superior mesenteric artery syndrome: an uncommon cause of intestinal obstruction. Southern medical journal, 93(6), 606-608. Gebhart, T. (2015). Superior mesenteric artery syndrome. Gastroenterology Nursing, 38(3), 189-193. McCallum R W. Superior mesenteric artery syndrome. Practical Gastroenterology, 3. 12-19. Naseem, Z., Premaratne, G., & Hendahewa, R. (2015). “Less is more”: Non operative management of short term superior mesenteric artery syndrome. Annals of Medicine and Surgery, 4(4), 428-430. Nutrition care manual website. https://www.nutritioncaremanual.org/. Accessed on April 29, 2016. Rabie, M. E., Ogunbiyi, O., Al Qahtani, A. S., Taha, S., El Hadad, A., & El Hakeem, I. (2015). Superior Mesenteric Artery Syndrome: Clinical and Radiological References cont. Merrett, N. D., Wilson, R. B., Cosman, P., & Biankin, A. V. (2009). Superior mesenteric artery syndrome: diagnosis and treatment strategies. Journal of Gastrointestinal Surgery, 13(2), 287-292. Chan, D. K., Mak, K. S., & Cheah, Y. L. (2012). Successful nutritional therapy for superior mesenteric artery syndrome. Singapore medical journal, 53(11), e233-6. Shin, M. S., & Kim, J. Y. (2013). Optimal duration of medical treatment in superior mesenteric artery syndrome in children. Journal of Korean medical science, 28(8), 1220-1225. Shiu, J. R., Chao, H. C., Luo, C. C., Lai, M. W., Kong, M. S., Chen, S. Y., ... & Wang, C. J. (2010). Clinical and nutritional outcomes in children with idiopathic superior mesenteric artery syndrome. Journal of pediatric gastroenterology and nutrition, 51(2), 177-182. Berchi, F. J., Benavent, M. I., Cano, I., Portela, E., & Urruzuno, P. (2001). Laparoscopic treatment of superior mesenteric artery syndrome. Pediatric Endosurgery and Innovative Techniques, 5(3), 309-314. References cont. Mascolo, M., Dee, E., Townsend, R., Brinton, J. T., & Mehler, P. S. (2015). Severe gastric dilatation due to superior mesenteric artery syndrome in anorexia nervosa. International Journal of Eating Disorders, 48(5), 532-534. Gthrie Jr, R. H. (1971). Wilkie's syndrome. Annals of surgery, 173(2), 290. Patel, A.H., Joshi, A.H., Shah, N. (2015). A case of superior mesenteric artery syndrome. IJSR. 4(6), 92-93.