Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
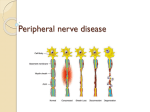
PERIPHERAL NEUROPATHY PHYSIOLOGY • Pain and temperature sensation : unmyelinated and small myelinated Ad fibers, • Vibratory sense, proprioception, and the afferent limb of the tendon reflex : large myelinated Aa and Ab fibers. • Light touch : both large and small myelinated fibers. FIVE QUESTION APPROACH 1. Fiber type 2. Pattern of distribution 5. Pathology 3. Temporal course 4. Key features • 1.What is the fiber type involved? (motor, large sensory, small sensory, autonomic, combination) • 2. What is the pattern of distribution? (distal or proximal, symmetric or asymmetric) • 3. What is the temporal course? (acute, chronic, progressive, stepwise, relapsing remitting) • 4. Are there any key features pointing to a specific etiology? (toxic/nutritional/malignancy) • 5. What is the pathology? (axonal, demyelinating) Pathological Process • (1) Wallerian degeneration, which is the response to axonal interruption; • (2) Axonal degeneration or axonopathy; • (3) Primary neuronal degeneration or neuronopathy; • (4) Segmental demyelination Wallerian degeneration • Any type of mechanical injury that causes interruption of axons leads to wallerian degeneration (degeneration of axons and their myelin sheaths) distal to the site of transection. Axonal degeneration • Most common pathological reaction of peripheral nerve • Caused by :Systemic metabolic disorders, toxin exposure, and some inherited neuropathies • Also called dying-back or length-dependent neuropathy: • The myelin sheath breaks down along with the axon in a process that starts at the most distal part of the nerve fiber and progresses toward the nerve cell body. Dying-back neuropathy • Clinically, presents with symmetrical, distal loss of sensory and motor function in the lower extremities that extends proximally in a graded manner. • The result is sensory loss in a stocking-like pattern, distal muscle weakness and atrophy, and loss of ankle reflexes Neuronopathy • Primary loss or destruction of nerve cell bodies with resultant degeneration of their entire peripheral and central axons. • Either lower motor neurons or dorsal root ganglion cells may be affected. • When anterior horn cells - poliomyelitis or motor neuron disease: focal weakness without sensory loss • Sensory neuronopathy, or polyganglionopathy :damage to dorsal root ganglion neurons - inability to localize the limb in space, diffuse areflexia, and sensory ataxia. Segmental demyelination • The term implies injury of either myelin sheaths or Schwann cells, resulting in breakdown of myelin with sparing of axons • This occurs in immune-mediated demyelinating neuropathies and in hereditary disorders of Schwann cell/myelin metabolism. Demyelinating neuropathies • Relative sparing of temperature and pinprick sensation + • 1.Early generalized loss of reflexes, 2.disproportionately mild muscle atrophy 3.presence of proximal and distal weakness, 4.neuropathic tremor 5. palpably enlarged nerves Diagnostic Clues from the History • 1.motor 2.sensory 3.autonomic disturbances. Seek both positive and negative symptoms. • A. Motor: • Positive : Muscle cramps, fasciculations, myokymia, or tremor • Negative : early distal toe and ankle extensor weakness, resulting in tripping on rugs or uneven ground Sensory symptoms Positive : • prickling, searing, burning, and tight bandlike sensations. • Paresthesia: Unpleasant sensations arising spontaneously without apparent stimulus • Allodynia: perception of nonpainful stimuli as painful. • Hyperalgesia: Painful hypersensitivity to noxious stimuli • Neuropathic pain: cardinal feature of many neuropathies. Autonomic dysfunction • • • • • • Orthostatic lightheadedness, Fainting spells, Sweating reduced or excessive, Heat intolerance, Bladder, Bowel, and Sexual dysfunction. Anorexia, early satiety, nausea, and vomiting TEMPORAL CLUES • • • • Onset, duration, and evolution of symptoms Tempo of disease : acute, subacute, or chronic Course: monophasic, progressive, or relapsing Acute presentations: Guillain-Barré syndrome (GBS), acute porphyria, vasculitis, toxic neuropathies. • Relapsing course : (CIDP), acute porphyria, Refsum's disease, hereditary neuropathy with liability to pressure palsies (HNPP), familial brachial plexus neuropathy, and repeated episodes of toxin exposure. Constitutional symptoms •Weight loss, malaise, and anorexia. • • • • • • • DM hypothyroidism chronic renal failure liver disease intestinal malabsorption malignancy connective tissue diseases • • • • • [HIV] drug use Vitamin B6 toxicity alcohol and dietary habits exposure to solvents, pesticides, or heavy metals. Mononeuropathy • Focal involvement of a single nerve and implies a local process: • Direct trauma • compression or entrapment • vascular lesions • neoplastic compression or infiltration Mononeuropathy multiplex • simultaneous /sequential damage to multiple noncontiguous nerves. • Ischemia caused by vasculitis • Microangiopathy in diabetes mellitus • Less common causes : Infectious, granulomatous, leukemic, or neoplastic infiltration, Hansen's disease (leprosy) and sarcoidosis. Polyneuropathy • Characterized by symmetrical, distal motor and sensory deficits that have a graded increase in severity distally and by distal attenuation of reflexes, • Rarely predominantly proximal:(E.g: acute intermittent porphyria). • The sensory deficits generally follow a lengthdependent stocking-glove pattern Motor deficits Dominate the clinical picture in • 1. AIDP/CIDP • 2. Hereditary motor and sensory neuropathies, • 3. Neuropathies associated with osteosclerotic myeloma, porphyria, lead and organophosphate intoxications, and hypoglycemia. Pattern of weakness • Asymmetrical motor weakness without sensory loss suggests motor neuron disease or multifocal motor neuropathy with conduction block Neuropathies with Facial Nerve Involvement • Guillain-Barré syndrome • Chronic inflammatory polyradiculoneuropathy • Lyme disease • Sarcoidosis • HIV Predominant Sensory • • • • • • • Diabetes • Carcinoma; Sjögren's syndrome; Dysproteinemia; • AIDS vitamin B12 deficiency Celiac disease Toxicity with cisplatin, thalidomide, or pyridoxine Inherited and idiopathic sensory neuropathies Autonomic dysfunction • GBS • Diabetes • Amyloid sensorimotor polyneuropathy Small-Fiber Neuropathies • • • • • Idiopathic small fiber neuropathy Diabetes mellitus Amyloid neuropathy HIV-associated distal sensory neuropathy Hereditary sensory and autonomic neuropathies Large-fiber • Areflexia • Pseudoathetosis • Loss of joint position and vibration sense • Positive Romberg's sign Electrodiagnostic studies • (1) Confirming the presence of neuropathy, • (2) Locating focal nerve lesions, • (3) Nature of the underlying nerve pathology Distal motor latency prolonged Nerve conduction velocity slow Reduced action potential Nerve biopsy • In vasculitis, amyloid neuropathy, leprosy, CIDP, Inherited disorders of myelin, and rare axonopathies • The Sural nerve is selected most commonly • The superficial peroneal nerve – alternative; :advantage of allowing simultaneous biopsy of the peroneus brevis muscle through the same incision. • This combined nerve and muscle biopsy procedure increases the yield of identifying suspected vasculitis Neuropathies + Serum Autoantibodies Antibodies against Gangliosides • GM1 : Multifocal motor neuropathy • GM1, GD1a : Guillain-Barré syndrome • GQ1b : Miller Fisher variant Antibodies against Glycoproteins • Myelin-associated glycoprotein : MGUS Antibodies against RNA-binding proteins • Anti-Hu, antineuronal nuclear antibody 1: Malignant inflammatory polyganglionopathy SUMMARY • A. Clinical pattern of neurologic findings Polyneuropathy, Neuronopathy, Mononeuropathy, Multiple mononeuropathy, Plexopathies • B. Functional disturbance: Motor, Sensory, Autonomic, Mixed • C. Mode of onset : • 1.Acute 2.Subacute 3.Chronic 4.Relapsing • • D. Pathological and electrophysiological criteria: • 1.Demyelinating disease vs Axonopathy • 2.Wallerian degeneration - trauma • 3.Dying back neuropathy - toxic, metabolic • E. Etiology: • Metabolic, immune mediated, toxic, vasculitis, dysproteinemic, inherited, Nutritional deficiency • • F. Diagnosis • 1.Clinical data • 2.Electrophysiologic test : NCS, EMG • 3.Biochemical test : metabolic, nutritional, toxic • 4.CSF study • 5. Nerve & muscle biopsy • 6. Measurement of Ig & anti-neural antibody • 7. Genetic study

















































![[SENSORY LANGUAGE WRITING TOOL]](http://s1.studyres.com/store/data/014348242_1-6458abd974b03da267bcaa1c7b2177cc-150x150.png)