Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Electronic Health Record (EHR)/EMR
In 1816, a Frenchman, Laennec wanted to examine an obese lady with heart trouble. The
very need to hear her heartbeats clearly made him think creatively and led him to invent
the stethoscope. Most of the physicians ridiculed it for they feared they would appear
funny with it. Nevertheless the stethoscope transcended all their misgivings to prove its
worth. Since more than two centuries now, it is the most extensively used medical
equipment today! Likewise, we can transform the healthcare operations by marrying
business and technology innovation.
Background: Medical records:
A medical record, health record, or medical chart is a systematic documentation of a patient's
medical history and care. The term 'Medical record' is used both for the physical folder for each
individual patient and for the body of information which comprises the total of each patient's
health history. Medical records are intensely personal documents and there are many ethical and
legal issues surrounding them such as the degree of third-party access and appropriate storage and
disposal. Although medical records are traditionally compiled and stored by health care providers,
personal health records maintained by individual patients have become more popular in recent
years.
Purpose
The information contained in the medical record allows health care providers to provide
continuity of care to individual patients. The medical record also serves as a basis for planning
patient care, documenting communication between the health care provider and any other health
professional contributing to the patient's care, assisting in protecting the legal interest of the
patient and the health care providers responsible for the patient's care, and documenting the care
and services provided to the patient. In addition, the medical record may serve as a document to
educate medical students/resident physicians, to provide data for internal hospital auditing and
quality assurance, and to provide data for medical research. Personal health records combine many
of the above features with portability, thus allowing a patient to share medical records across
providers and health care systems.
Format
Traditionally, medical records have been written on paper and kept in folders. These folders are
typically divided into useful sections, with new information added to each section chronologically
as the patient experiences new medical issues. Active records are usually housed at the clinical site,
but older records (e.g., those of the deceased) are often kept in separate facilities.
The advent of electronic medical records has not only changed the format of medical records but
has increased accessibility of files.
Electronic Health Record:
Definitions:
1. An EHR, also called an electronic medical record, acts as a" personal health library"
providing access to all resources on a patient's health history and insurance information.
An EHR is a linking system rather than an independent database, and is more a process than
a product. An integrated EHR will link to separate sources detailing medical history and
images, laboratory results and drug allergies. Several organizations are focused on creating
standards for EHRs, including common coding terminology, clinical decision support,
patient confidentiality and secure data transfers.
2. An electronic health record (EHR) refers to an individual patient's medical record in digital
format. Electronic health record systems co-ordinate the storage and retrieval of individual
records with the aid of computers. EHRs are usually accessed on a computer, often over a
network. It may be made up of electronic medical records (EMRs) from many locations
and/or sources. A variety of types of healthcare-related information may be stored and
accessed in this way.
Even though EMR systems with computerized provider order entry (CPOE) have existed for more
than 30 years, less than 10 percent of hospitals as of 2006 have a fully integrated system.
EMR vs. EHR
Overlap in Terminology
Multiple terms have been used to define electronic patient care records, with overlapping
definitions. Both electronic health record (EHR) and electronic medical record (EMR) have gained
widespread use, with some health informatics users assigning the term EHR to a global concept and
EMR to a discrete localised record. For most users, however, the terms EHR and EMR are used
interchangeably. An EHR system is also often abbreviated as EHR or EMR.
The electronic medical record (EMR) is simply one of several kinds of electronic health records
(EHR), which include general health-related information not directly related to the patient’s
record.
Evolution of Medical Records:
1. In the beginning there was the hand written chart. It was simple and the tools were
inexpensive (pen & paper). However, the hand written chart has many disadvantages.
Limitations:
It is both time consuming & tedious. Furthermore, hand written charts are often illegible.
The common belief about doctor?s handwriting is not only a cliché but is all too often a
fact. Illegible handwritten charts not only waste time producing and interpreting, they can
lead to more serious problems such as errors in diagnoses, treatment and billing.
Another major problem with handwritten charts is their inaccessibility. They must be
stored and retrieved manually. The data in these charts is difficult to access. . As a result,
these charts are inefficient and thus not very useful to those delivering care. Furthermore,
the same data has to be entered repeatedly, which wastes even more time and increases the
chance of errors.
Clearly there had to be a better way...
2. Next came Transcription. This did improve legibility, and saving the chart as a computer file
did make it somewhat easier to store & retrieve. However, transcription also has some
serious drawbacks.
Drawbacks:
Transcription is not "real time" ? Documents are transcribed and returned hours, or more
often, days after the health care was delivered. Important data is often lost/changed before,
during and after transcription. The inherent time delays in this method of charting
increases the likelihood of missing any errors created during the transcription process.
Transcription can be very costly, with transcription services charging by the page or line.
Although the transcribed files can be saved and retrieved on the computer, they are just
plain text files and do not have the power of a true database.
3. PC-based word processors (MS Word, etc.) brought about the next step in medical record
creation. Now the chart could be created right in the doctors office and were legible and
easy to store & retrieve. However, this system is still less than ideal.
Limitations:
Keying in data can be time consuming, depending on the typing skills and fatigue level of
the writer.
Specific medical data is not easily retrievable or searchable. With a word processor you
cannot generate Q A reports or provide much useful data beyond a paper document. In this
regard they are similar to charts generated by a transcription service. Word processor
produced charts just don't have the power and convenience of a true database.
History of EHRs:
1. The impetus for computer-based patient records, now Electronic Health Records or EHR,
arose from a 1999 report completed by the Institute of Medicine (IOM), an organization
that serves as an independent, scientific adviser to the nation on the issue of health. This
report entitled “To Err is Human: Building a Safer Health System,” found that up to 98,000
hospital patients die unnecessarily each year in the United States. The Institute then
challenged the healthcare industry to reduce preventable errors by 50% by 2004. Care
delivery organizations (CDOs) can expect to spend a lot of time and money addressing this
issue and will be faced with many difficult decisions along the way. One such decision
involves how to use technology to reduce medical error rates. The Gartner Group contends
that CDOs can invest in narrowly focused approaches, such as automated prescription
writing, and achieve a series of limited, tactical gains on a restricted budget, or they can
tackle the large task of implementing an EHR system. The EHR approach will cost more in
terms of money and time but will ultimately position a CDO to achieve a more significant
improvement in error rates as well as realize the many other benefits associated with
implementing a EHR.
While many of the industry’s players have taken to heart the Institute’s challenge to reduce
medical errors by 50%, much progress remains to be made. For example, when Mark Neaman,
president and CEO of Evanston Northwestern Healthcare, first saw the 1999 report he was
horrified and vowed to rectify the situation. The three-hospital system in the Chicago suburbs has
fully implemented an electronic medical record system, educated staff and launched an online
portal where patients can have 24-hour access to their medical information and correspond with
physicians. The result, which was reported in 2004, has been a 20% drop in medication errors and
total elimination of transcription errors, Neaman contends. In another example, at St. Luke's
Episcopal Hospital, a 664-bed facility in Houston, administrators reacted to the report by creating a
new position-director of patient safety and quality enhancement. Then they bar-coded medication
and tried to improve doctors' handwriting to cut down on prescription errors. Eventually the
hospital moved to a system where doctors entered drug prescriptions by computer and
computerized standard order sets so doctors could see what kinds of drugs were recommended for a
specific ailment. St. Luke's has implemented all national patient-safety goals including those
established by the NQF (National Quality Forum). However, not all CDOs have made similar
progress as five years after the groundbreaking IOM report, follow-up reports and assessments have
painted a bleak picture of healthcare quality and safety. Also, despite all the talk of information
technology in healthcare, only 4.4% of the 1,019 hospitals surveyed had fully implemented
computerized physician order-entry systems.
2) In the 1960s, a physician named Lawrence L. Weed first described the concept of
computerized or electronic medical records. Weed described a system to automate and
reorganize patient medical records to enhance their utilization and thereby lead to
improved patient care.
Weed's work formed the basis of the PROMIS project at the University of Vermont, a collaborative
effort between physicians and information technology experts started in 1967 to develop an
automated electronic medical record system. The project?s objectives were to develop a system that
would provide timely and sequential patient data to the physician, and enable the rapid collection
of data for epidemiological studies, medical audits and business audits. The group?s efforts led to
the development of the problem-oriented medical record, or POMR. Also, in the 1960s, the Mayo
Clinic began developing electronic medical record systems.
In 1970, the POMR was used in a medical ward of the Medical Center Hospital of Vermont for the
first time. At this time, touchscreen technology had been incorporated into data entry procedures.
Over the next few years, drug information elements were added to the core program, allowing
physicians to check for drug actions, dosages, side effects, allergies and interactions. At the same
time, diagnostic and treatment plans for over 600 common medical problems were devised.
During the 1970s and 1980s, several electronic medical record systems were developed and further
refined by various academic and research institutions. The Technicon system was hospital-based,
and Harvard?s COSTAR system had records for ambulatory care. The HELP system and Duke?s
?The Medical Record? are examples of early in-patient care systems. Indiana's Regenstrief record
was one of the earliest combined in-patient and outpatient systems.
With advancements in computer and diagnostic applications during the 1990s, electronic medical
record systems became increasingly complex and more widely used by practices. In the 21st
century, more and more practices are implementing electronic medical records.
Potential Benefits of the EHRs:
Advantages of electronic medical records over paper records
A medical record includes any of an individual's health documents of the types listed above.
Medical records may be on "physical" media such as film (X-rays), paper (notes), or
photographs, often of different sizes and shapes. Physical storage of documents is
problematic, as not all document types fit in the same size folders or storage spaces. In the
current global medical environment, patients are shopping for their procedures. Coordinating
these appointments via paper records is a time-consuming procedure and may violate the
patient's HIPAA privacy.
Physical records usually require significant amounts of space to store them. When physical
records are no longer maintained, the large amounts of storage space are no longer required.
Paper, film, and other expensive physical media usage (and therefore cost) is also reduced
with electronic record storage.
When paper records are stored in different locations, furthermore, collecting and transporting
them to a single location for review by a healthcare provider is time-consuming. When paper
(or other types of) records are required in multiple locations, copying, faxing, and
transporting costs are significant, as are the concerns of HIPAA compliance.
Electronic medical records are estimated to improve efficiency by 6% per year, and the
monthly cost of an EMR is offset by the cost of only a few unnecessary tests or admissions.
Handwritten paper medical records can be associated with poor legibility, which can
contribute to medical errors. Pre-printed forms, the standardization of abbreviations, and
standards for penmanship were encouraged to improve reliability of paper medical records.
Electronic records help with the standardization of forms, terminology and abbreviations,
and data input. Digitization of forms facilitates the collection of data for epidemiology and
clinical studies.
Electronic records keeping and order entry were found to reduce errors associated with
handwritten documents and were recommended for widespread adoption.
1. EHR systems can reduce medical errors.
2. EHR systems are believed to increase physician efficiency and reduce costs, as well as
promote standardization of care.
3. help improve quality of care and control costs by leveraging an interoperability
infrastructure to enable collaborative healthcare processes.
4. Help improve quality of care and control costs by leveraging an interoperability
infrastructure to enable collaborative healthcare processes.
5. builds a Collaborative Health Information Network across a range of clinical services
including electronic/personal health records, health management tools, ePrescribing,
referral management, clinical messaging, and scheduling.
6. It offers a comprehensive 360 degree view of the patient in a provider, payer
7. The solution aims to provide the right information to the right person at the right time.
8. It helps organizations improve patient care, safety and quality, while simultaneously
reducing preventable medical errors and costs.
9. It delivers a mechanism to aggregate, transmit and exchange clinical information
across enterprises.
Benefits of EHR standardization / National Healthcare Information Network
Improved billing accuracy
Billing is a tedious task when records are in an electronic format not compatible with the billing
program, or when the records are in paper format. An integrated electronic medical record / billing
system, therefore, both expedites and makes billing more accurate.
Reduction in duplication of services
Duplication of lab tests, diagnostic imaging, work-ups, and other services can be prevented by good
record-keeping of any type. However, because electronic records can be available at many
locations at once, integration of services and awareness of duplication is facilitated.
Facilitation of clinical trials
Clinicians and researchers suggest benefits to integrating electronic health records with data
collection and analysis in clinical trials.
Potential clinical trial participants may be more easily identified, administrative overhead costs
may be lessened, data errors may be reduced, and adverse outcomes may more rapidly identified.
Some institutions have already been partially successful in implementing and integrating coordinated data collection and analysis systems. For example, the Shared Pathology Network (SPIN)
of the National Cancer Institute has effectively established a web-based network for locating
pathological tissue samples at various institutions across the nation. The electronic nature of
reports within the system allows the use of search engines to find specific text with the reports,
facilitating analysis.
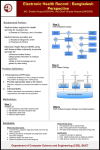
EHR Components:
There are six primary components of an EHR system.
1. Clinical Data Repository (CDR)
Provides a comprehensive source for clinical information to avoid errors
2. Clinical Decision Support System (CDSS)
Provides rule-based alerts that help avoid errors such as a patient inadvertently placed on
two medications that have a dangerous interaction
3. Clinical Documentation Module
Can inform each clinician of the activities of the other clinicians helping to manage this
patient.
4. Computerized Point of Entry (CPOE) module
Helps to eliminate errors resulting from illegible, handwritten orders.
5. Controlled Medical Vocabulary (CMV)
Ensures that information from various clinical sources can be compared and makes it easier
to write proper clinical rules to ensure the quality of medical care
6. Workflow Controller
Manages clinical care processes so that they are carried out properly, in the correct
sequence and without omissions.
Ideal characteristics of an electronic health record (EHR)
Information should be able to be continuously updated.
The data from an electronic health records system should be able to be used anonymously
for statistical reporting for purposes of quality improvement, outcome reporting, resource
management, and public health communicable disease surveillance.
The ability to exchange records between different electronic health records systems
("interoperability") would facilitate the co-ordination of healthcare delivery in nonaffiliated healthcare facilities.
Continuity of Care Record
Continuity of Care Record (CCR) is a health record standard specification developed jointly by
ASTM International, the Massachusetts Medical Society (MMS), the HIMSS (HIMSS), the
American Academy of Family Physicians (AAFP), the American Academy of Pediatrics (AAP), and
other health informatics vendors.
The CCR standard
The CCR standard is a patient health summary standard. It is a way to create flexible documents
that contain the most relevant and timely core health information about a patient, and to send
these electronically from one care giver to another. It contains various sections such as patient
demographics, insurance information, diagnosis and problem list, medications, allergies and care
plan. These represent a "snapshot" of a patient's health data that can be useful or possibly lifesaving,
if available at the time of clinical encounter. The ASTM CCR standard is designed to permit easy
creation by a physician using an electronic health record (EHR) system at the end of an encounter.
Because it is expressed in the standard data interchange language known as XML, a CCR can
potentially be created, read and interpreted by any EHR or EMR software application. A CCR can
also be exported in other formats, such as PDF and Office Open XML (Microsoft Word 2007
format).
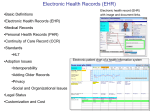
Types of data stored in an electronic medical record
An electronic medical record might include:
* Patient demographics.
* Medical history, examination and progress reports of health and illnesses.
* Medicine and allergy lists, and immunization status.
* Laboratory test results.
* Radiology images (X-rays, CTs, MRIs, etc.)
* Photographs, from endoscopy or laparoscopy or clinical photographs.
* Medication information, including side-effects and interactions.
* Evidence-based recommendations for specific medical conditions
* A record of appointments and other reminders.
* Billing records.
* Eligibility
* Advanced directives, living wills, and health powers of attorney
Barriers to implementing an EHR system
Difficulty in adding older records to an EHR system
Older paper medical records ought to be incorporated into a patient's electronic health
record.
One method is to merely scan the documents and retain them as images. However, surveys
suggest that 22-25% of physicians are less satisfied with records systems that use scanned
documents alone rather than fully electronic data-based systems. EHR systems with image
archival capability (such as VistA Imaging) are able to integrate these scanned records
(along with other types of image-based records) into fully electronic health records systems.
Another method to convert written records (such as notes) into electronic format is to scan
the documents then perform optical character recognition. For typed documents, accurate
recognition may only achieve 90-95%, though, requiring extensive corrections.
Furthermore, illegible handwriting is poorly recognized by optical character readers.
Some states have proposed making existing statewide database data (such as immunization
records) available for download into individual electronic medical records.
Long-term preservation and storage of records
An important consideration in the process of developing electronic health records is to plan for the
long-term preservation and storage of these records. The field will need to come to consensus on
the length of time to store EHRs, methods to ensure the future accessibility and compatibility of
archived data with yet-to-be developed retrieval systems, and how to ensure the physical and
virtual security of the archives.
Additionally, considerations about long-term storage of electronic health records are complicated
by the possibility that the records might one day be used longitudinally and integrated across sites
of care. Records have the potential to be created, used, edited, and viewed by multiple independent
entities. These entities include, but are not limited to, primary care physicians, hospitals, insurance
companies, and patients. Mandl et al have noted that “choices about the structure and ownership of
these records will have profound impact on the accessibility and privacy of patient information.”
The required length of storage of an individual electronic health record will depend on national
and state regulations, which are subject to change over time. Ruotsalainen and Manning have
found that the typical preservation time of patient data varies between 20 and 100 years. In one
example of how an EHR archive might function, their research "describes a co-operative trusted
notary archive (TNA) which receives health data from different EHR-systems, stores data together
with associated meta-information for long periods and distributes EHR-data objects. TNA can store
objects in XML-format and prove the integrity of stored data with the help of event records,
timestamps and archive e-signatures."
In addition to the TNA archive described by Ruotsalainen and Manning, other combinations of
EHR systems and archive systems are possible. Again, overall requirements for the design and
security of the system and its archive will vary and must function under ethical and legal principles
specific to the time and place.
While it is currently unknown precisely how long EHRs will be preserved, it is certain that length
of time will exceed the average shelf-life of paper records. The evolution of technology is such that
the programs and systems used to input information will likely not be available to a user who
desires to examine archived data. One proposed solution to the challenge of long-term accessibility
and usability of data by future systems is to standardize information fields in a time-invariant way,
such as with XML language.
Healthcare Information Exchange and Interoperability:
In healthcare, interoperability is the ability of different information technology systems and
software applications to communicate, to exchange data accurately, effectively, and consistently,
and to use the information that has been exchanged.
In the United States, the development of standards for EMR interoperability is at the forefront of
the national health care agenda. EMRs, while an important factor in interoperability, are not a
critical first step to sharing data between practicing physicians, pharmacies and hospitals. Many
physicians currently have computerized practice management systems that can be used in
conjunction with health information exchange (HIE), allowing for first steps in sharing share
patient information(lab results, public health reporting) which are necessary for timely, patientcentered and portable care. There are currently multiple competing vendors of EHR systems, each
selling a software suite that in many cases is not compatible with those of their competitors. Only
counting the outpatient vendors, there are more than 25 major brands currently on the market.
The Center for Information Technology Leadership described four different categories (“levels”) of
data structuring at which health care data exchange can take place. While it can be achieved at any
level, each has different technical requirements and offers different potential for benefits
realization.
The four levels are:
Level
Data Type
Example
1
2
Non-electronic data
Machine transportable data
Paper, mail, and phone call.
Fax, email, and unindexed documents.
3
Machine organizable data
(structured messages,
unstructured content)
HL7 messages and indexed (labeled)
documents, images, and objects.
4
Machine interpretable data
(structured messages,
standardized content)
Automated transfer from an external lab of
coded results into a provider’s EHR. Data can
be transmitted (or accessed without
transmission) by HIT systems without
need
for further semantic interpretation or
translation.
Medical Industry
New technologies are being introduced in hospitals and labs at an ever-increasing rate, and many
of these innovations have the potential to interact synergistically if they can be integrated
effectively. The need for “plug-and-play” interoperability – the ability to take a medical device out
of its box and easily make it work with one’s other devices – has attracted great attention from
both healthcare providers and industry.
Interoperability helps patients get the most out of technology, and it also encourages innovation in
the industrial sphere. When different products can be combined without complicated and
expensive interfaces, small companies can enter a field and make specialized products. Without
interoperability, hospitals are forced to turn to large vendors that provide suites of compatible
devices but that do not specialize in any one area. Interoperability promotes competition, and
competition encourages innovation and quality.
From the perspective of Intel, a major producer of consumer healthcare devices, there are six major
factors that affect an industry’s ability to achieve interoperability. First there needs to be a demand
for interoperable products. Second, there must be standards, or rules, defining what
interoperability means in the field. Third, business conditions must encourage manufacturers to
make their products interoperable. Fourth, guidelines must exist that make the often-complicated
standards easier for companies to interpret. Fifth, compliance must be verified by independent
testing; and finally, interoperability must be actively promoted. The rapid rise of wireless
technology illustrates that interoperability is attainable.
Conditions in the biomedical industry are still in the process of becoming conducive to the
development of interoperable systems. A potential market of interested hospitals exists, and
standards for interoperability are being developed. Nevertheless, it seems that current business
conditions do not encourage manufacturers to pursue interoperability. Only sixteen to twenty
percent of hospitals, for example, use electronic medical records (EMR). With such a low rate of
EMR adoption, most manufacturers can get away with not investing in interoperability. In fact, not
pursuing interoperability allows some of them to tout the inter-compatibility of their own products
while excluding competitors. By promoting EMR adoption, companies such as Intel hope to create
an environment in which hospitals will have the collective leverage to demand interoperable
products.
Health information exchange (HIE)
Health information exchange is defined as the mobilization of healthcare information
electronically across organizations within a region or community.
HIE provides the capability to electronically move clinical information between disparate health
care information systems while maintaining the meaning of the information being exchanged. The
goal of HIE is to facilitate access to and retrieval of clinical data to provide safer, more timely,
efficient, effective, equitable, patient-centered care.
Formal organizations are now emerging to provide both form and function for health information
exchange efforts. These organizations (often called Regional Health Information Organizations, or
RHIOs) are ordinarily geographically-defined entities which develop and manage a set of
contractual conventions and terms, arrange for the means of electronic exchange of information,
and develop and maintain HIE standards.
Health Level 7
Health Level Seven (HL7), is an all-volunteer, not-for-profit organization involved in development
of international healthcare standards. “HL7” is also used to refer to some of the specific standards
created by the organization (i.e. HL7 v2.x, v3.0, HL7 etc.) HL7 and its members provide a
framework (and related standards) for the exchange, integration, sharing and retrieval of electronic
health information. The standards, which support clinical practice and the management, delivery,
and evaluation of health services, are the most commonly used in the world. HL7 is an
international community of healthcare subject matter experts and information scientists
collaborating to create standards for the exchange, management and integration of electronic
healthcare information.
HL7 promotes the use of such standards within and among healthcare organizations to increase the
effectiveness and efficiency of healthcare delivery for the benefit of all.
Some Examples:
* LifeSaver
* CHITS Community Health Information Tracking System
* GNUmed
* FFEHR
* Hospital OS
* OpenEMR
* openEHR
* OpenMRS
* OSCAR
* Open Healthcare
* PatientOS
* HOSxP
* VistA
* ClearHealth ClearHealth
* SmartCare