Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Forensic epidemiology wikipedia , lookup
Clinical trial wikipedia , lookup
Harm reduction wikipedia , lookup
Patient safety wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Pharmacogenomics wikipedia , lookup
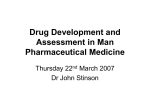
Pharmacovigilance 1 The New Drug Development Process: Steps from Test Tube to New Drug Application Review ▪ FDA estimates 8 year time-span for entire process ▪ Pharmaceutical industry claims $802 million spent for each new drug brought to market 2 Courtesy: www.fda.gov/cder/handbook/develop.htm, 2007. Learning Objectives • Pharmacovigilance and Global Pharmacovigilance System • Individual Case Safety Reports (ICSRs), AEM form, CIOMS and Medwatch • Case processing and Reporting • Medical dictionary (MedDRA) and Medical aspects in Pharmacovigilance • Special cases in Pharmacovigilance • Medical Information System • Safety monitoring in Clinical Trials • Signal detection • Periodic Safety Update Reports (PSURs) and suspected unexpected serious adverse reactions (SUSARs) • Medication errors, Risk –benefit assessment and management in Pharmacovigilance • Standard Operating Procedures in Pharmacovigilance • Compliance monitoring and Pharmacovigilance inspections • Global regulatory affairs and their requirements and related guidelines in Pharmacovigilance • Pharmacovigilance communications 3 • Pharmacoepidemiology Pharmacovigilance The science and activities relating to the Detection, Assessment, Understanding and Prevention of adverse effects or any other medicine-related problem - WHO 4 Vigilance • Vigilare = to watch –alert watchfulness – forbearance of sleep; wakefulness –watchfulness in respect of danger; care; caution; circumspection –the process of paying close and continuous attention 5 Adverse Event An unwanted or harmful reaction experienced following the administration of a drug or combination of drugs under normal condition of use and suspected to be related to the drug. 6 Common ADRs • • • • Constipation after Codeine Sedation with Antihistamine Nausea with Fluaxetine GIT upset with NSAIDs 7 ▪ 1959 / 61–Thalidomide 4.000 – 10.000 cases (Phocomelia) Medicines are supposed to save lives Dying from a disease is sometimes unavoidable; dying from a medicine is unacceptable. WHO. 8 Geneva 2005 Drug Outcomes » Outcomes: • • • Effects (Pharmacological, therapeutic) Side effects (Unintended) Interactions (Expected, unexpected) » Impact: • • Beneficial Harmful 9 Harmful Effects • Mortality • Morbidity » Hospitalization » Prolonged stay » Extra treatment • Cost »Resources consumed 10 Need for PVG • Limited value of animal experiments in predicting human safety • Clinical trials are limited in time and number of individuals (a few hundred), usually under favorable conditions, i.e. in the hospital, under close surveillance, over a short period, with few concomitant medications, and with few high-risk individuals (e.g. children, older individuals, pregnant women, or patients with renal or hepatic failure) 11 Populations not studied in the pre-approval phase • • • • Children The elderly Pregnant or lactating women Patients with co-morbidity such as hepatic or renal disorders • Sup-populations carrying known and relevant genetic polymorphisms • Patients of different racial and/or ethnic origins 12 Drug Development Clinical development of medicines Phase I 20 – 50 healthy volunteers to gather preliminary data Animal experiments for acute toxicity, organ damage, dose dependence, metabolism, kinetics, carcinogenicity, mutagenicity/teratoge nicity Preclinical Animal Experiments Phase I Development Phase III 250 – 4000 more varied patient groups – to determine short-term safety and efficacy Phase II 150 – 350 subjects with disease - to determine safety and dosage recommendations Phase II Phase III Phase IV Post-approval studies to determine specific safety issues Phase IV Spontaneous Post-approval Reporting Post Registration 13 Need for PVG • Rare or delayed serious reactions are likely to remain unnoticed • Rare ADRs (occurring for instance in 1/1000 individuals) are unlikely to be identified in pre-marketing studies. Effects that are difficult, even impossible to detect clinically » Toxicity to Reproduction » Genotoxicity » Carcinogenicity • A drug that belongs to a widely used pharmacological class may be used in up to 100,000 individuals within the first month, so that a rare but serious ADR may occur only in few patients. rare diseases occurs as very rare as rare 14 Medication Errors • Medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professionals, patient, or consumer. 15 Key facts • No medicine is risk free. Vigilant assessment of the risks and benefits of medicines promotes patient safety. • People in every country of the world are affected by ADRs. In some countries ADRrelated costs, such as hospitalization, surgery and lost productivity, exceed the cost of the medications. • Unintended, harmful reactions to medicines (known as adverse drug reactions) are among the leading causes of death in many 16 countries. Medication Errors … . USA Drug related death rate: 19% due to adverse events in health care 50% preventable United Kingdom Adverse events in 10% of patients 50% preventable 1100 deaths in adverse drug events (low estimate) Australia Adverse events cause 16.6%of hospital admissions Adverse drug events in 2-4%hospital admissions Up to 75% potentially preventable 17 • 1. 2. 3. 4. 5. 6. 7. 8. Key facts… The majority of adverse drug reactions (ADR) are preventable and can be due to: Wrong diagnosis of the patient’s condition; Prescription of the wrong drug or wrong dosage of the right drug; An undetected medical, genetic or allergic condition that might cause a patient reaction; Self-medication with prescription medicines; Not following the instructions for taking the medication; Reactions with other drugs (including traditional medicines) and certain foods; Use of a sub-standard medication whose composition and ingredients do not meet the correct scientific requirements, and can be ineffective and often dangerous; Use of counterfeit medicines with no active ingredients or the wrong ingredients, which can be dangerous or fatal. Prescribing & transcription – 60%; Administration – 30%; 18 Dispensing – 10% Aims and Responsibilities • • • • • Early detection of unknown safety problems Detection of increases in frequency Identification of risk factors Quantifying risks Preventing patients/Public from being affected unnecessarily • Standard Requirements: » Reporting » Labelling » Approach (Insert, package, etc) 19 When PVG Starts • Testing of drug safety always begins in clinical trials. Before a medication reach the market, it must go through several stages of clinical trials to gauge the potential risks and benefits associated with the drug 20 Adverse Reactions: Possible Causes • Intrinsic factors of the drug – – – – Pharmacological Idiosyncratic Carcinogenicity, Mutagenicity Teratogenicity • Extrinsic factors – Adulterants – Contamination • Underlying medical conditions • Interactions • Wrong usage 21 Outcome of PVG • Contribute to the regulatory assessment of benefit, harm, effectiveness and risk of medicines, encouraging their safe, rational and more effective (including cost effective) use. • Improve patient care and safety in relation to use of medicines and all medical and paramedical interventions. • Improve public health and safety in relation to use of medicines. • Promote understanding, education and clinical training in Pharmacovigilance and its effective communication to the public. • The results of pharmacoepidemiological studies would confirm or disprove the license • Effectiveness of the drug in clinical practice (confirmation of the therapeutic effect), determine whether approved uses • Should be expanded or restricted 22 Classification Pharmacovigilance Active Passive ADR Cause Severity 23 Passive or active Pharmacovigilance? Active PVG: Active (or proactive) safety surveillance means that active measures are taken to detect adverse events. This is managed by active follow-up after treatment and the events may be detected by asking patients directly or screening patient records. The most comprehensive method is cohort event monitoring (CEM) The essential and interesting tasks of causality assessment and signal identification are applicable to both methods of surveillance 24 Passive or Active Pharmacovigilance? Passive PVG: Passive surveillance means that no active measures are taken to look for adverse effects other than the encouragement of health professionals and others to report safety concerns. Reporting is entirely dependent on the initiative and motivation of the potential reporters. This is the most common form of pharmacovigilance. It is commonly referred to as “spontaneous” or “voluntary” reporting. In some countries this form of reporting is mandatory 25 ADVERSE DRUG REACTIONS TYPES BY CAUSE • Type A: Augmented pharmacologic effects dose dependent and predictable a. Intolerance b. side effects • Type B: Bizarre effects (or idiosyncratic) dose independent and unpredictable • Type C: Chronic effects • Type D: Delayed effects • Type E: End-of-treatment effects • Type F: Failure of therapy 26 ADVERSE DRUG REACTIONS TYPES BY CAUSE 1. Type A Type A reactions are extensions of the drug's known pharmacology 1. Responsible for the majority of ADRs. • Type A reactions ate usually dose dependent and predictable but can be the result of concomitant disease states, drug-drug interactions, or drugfood interactions. • • Ways to minimize type A reactions include understanding the pharmacology of the drug being prescribed, monitoring drugs with a narrow therapeutic index, and avoiding poly-pharmacy when possible. 1. Type B Type B reactions are usually not the result of a known pharmacology of the drug but seem to be a function of patient susceptibility. 1. Uncommon but are generally serious and can be life threatening. • They are rarely predictable, are usually not dose dependent, and seem to concentrate in certain body systems such as the liver, blood, skin, kidney, and nervous system. • Type B reactions include idiosyncratic reactions, immunological or allergic reactions, and carcinogenic or teratogenic reactions • Except for immediate hypersensitivity reactions, type B reactions usually take 5 days before the patient demonstrates hypersensitivity to a drug. There is no maximum time for the occurrence of a reaction, but most occur within 12 weeks of initiation of therapy. e.g. cough with ACE Inhibitors e.g. cough with ACE Inhibitors • 27 When is an ADR serious? • Death / life-threatening (real risk of dying) • Hospitalization (initial or prolonged) • Disability (significant, persistent or permanent) • Congenital anomaly • Required intervention to prevent permanent impairment or damage • Causes malignancy and Malformations • Medical and scientific judgment determines 28 SAEs that may not need to be recorded on an SAE • Deaths due to disease in a study where death is a primary endpoint Example: Death from stroke in a stroke trial Death from Cancer in a caner trial 29 Exceptions to hospitalization as SAEs • In the absence of medical adverse event • Admission for the treatment of a pre-existing condition not associated with the development of a new AE with a worsening of a pre-existing condition • Social admission • Administrative admission • Protocol specified admission during the study • Any other optional admission not related tot the AE • Hospitalization for an event that is an endpoint – MI, AIDS event, cancer recurrence 30 Confirmation of case seriousness Seriousness should not be changed if the case • Received as serious from an HCP • Received from a license partner or regulatory authority • Clinical trial case that already reported as serious • MedDRA preferred critical term (coded as always serious) 31 Ratings by iGuard While no official scale exists yet to communicate overall drug risk, the iGuard Drug Risk Rating System is a five color rating scale similar to the Homeland Security Advisory System • High Risk (Red): Requires careful consideration of risk versus benefit with your doctor. e.g. Adriamycin, Vincristine • Elevated (Orange): Create a personal risk reduction plan with your doctor e.g. Prednisone, Warfarin, Insulin • Guarded (Yellow): Reserved for new products, be on the lookout for safety events e.g. Januvia, Yaz • General (Blue): Use under the normal care of your doctor e.g. Lipitor, Lopressor • Low (Green): Suitable for widespread use e.g. Vitamin C, Caltrate In the United States, the Homeland Security Advisory System is a color-coded terrorism threat advisory scale 32 Definitions Term Definition Adverse Event (AE) Any untoward medical occurrence in a Patient or Clinical Trial Subject administered a medicinal product and which does not necessarily have a causal link with the treatment. Adverse Reaction (AR) or Adverse Drug Reaction (ADR) Unexpected Adverse Reaction (UAR) SUSAR Suspected Unexpected Serious Adverse Reaction (SUSAR) Any untoward and unintended responses to an investigational medicinal product related to any dose administered. An adverse reaction, the nature or severity of which is not consistent with the product information eg. Investigator Brochure (IB) or Summary of Product Characteristics or USPI or CDS not listed in the protocol as an expected adverse reaction and it occurs it is defined as a SUSAR A Useful Hint: Minimise SUSARs by listing everything you know about the Dru33g Examples of ADRs Medicines Reactions Amidopyrine (for inflammation) White blood cell disorder Clioquinol (for skin infections) Visual impairment Erythromycin estolate (antibacterial) Hepatitis (liver disorder) Oral contraceptives Thromboembolism (blood clots) Statins (for controlling cholesterol) Muscle degeneration Thalidomide (for managing morning sickness) Phocomelia (disfigured infants) Courtesy: WHOSIS 34 TEN DRUGS WITH THE MOST REPORTED ADRs NO 2002 2003 2004 2005 2006 2007 1 CO – TRIMOXAZOLE (47) ALLOPURINOL (33) ALLOPURINOL (37) CAPTOPRIL (52) TRADITIONAL MEDICINE (68) PERINDOPRIL (97) 2 CARBAMAZEPINE (32) CLOXACILLIN (30) PARACETAMOL (29) ALLOPURINOL (51) DICLOFENAC (65) ALLOPURINOL (75) 3 CLOXACILLIN (31) MEFENAMIC ACID (25) CARBAMAZEPINE (29) CLOXACILLIN (50) CARBAMAZEPINE (62) CLOXACILLIN (71) 4 AMOXYCILLIN (28) DICLOFENAC (24) NIFEDIPINE (28) DICLOFENAC (44) NIFEDIPINE (58) DICLOFENAC (71) 5 ALLOPURINOL (22) CHLOROTHIAZIDE (22) CO – TRIMOXAZOLE (28) NIFEDIPINE (44) ALLOPURINOL (57) METFORMIN (69) 6 TRADITIONAL MEDICINE (22) CARBAMAZEPINE (19) ERYTHROMYCIN (23) METFORMIN (39) PERINDOPRIL (57) ASPIRIN (67) 7 ALENDRONATE (19) TRADITIONAL MEDICINE (18) AMOXYCILLIN (23) PARACETAMOL (38) CO – TRIMOXAZOLE (55) 8 DICLOFENAC (19) AMOXYCILLIN (18) MEFENAMIC ACID (21) CO – TRIMOXAZOLE (37) ASPIRIN (41) RIFAMPICIN (46) 9 ISOSORBIDE DINITRATE (18) PENICILLIN G SODIUM (15) ASPIRIN (19) ATENOLOL (37) ERYTHROMYCIN (40) PHENYTOIN (44) 10 LOVASTATIN (13) VANCOMYCIN (15) CLOXACILLIN (18) CEFUROXIME (36) PHENYTOIN (39) TICLOPIDINE (50) AMOXYCILLIN (43) 35 ACTIVE INGREDIENTS WITHDRAWN – – – – – – – – – – – THALIDOMIDE (1961) BENOXAPROFEN (1982) PHENFORMIN (1982) FENFLURAMINE (1997) ASTEMIZOLE PHENYLPROPANOLAMINE(2000) KAVA KAVA CERIVASTATIN CISAPRIDE ROFECOXIB (2004) VALDECOXIB (2005) – COMFREY, SENECIO – TEGASEROD (2007) – CLOBUTINOL (2007) Congenital limb defects Hepatotoxicity Lactic acidosis Heart-valve abnormalities Many drug interactions Haemorragic stroke Liver abnormalities Rhabdomyolysis Cardiac arrythmias Cardiovascular events Cardiovascular events, serious skin reactions Nephrotoxicity Cardiovascular events Cardiac arrhythmia 36 Functions of Pharmacovigilance (WHO Guidelines, 2000) • Detection and study of adverse reactions • Measurement of risk and benefits • Measurement of effectiveness and Monitoring the impact of any corrective actions taken • Benefit & harm evaluation • Dissemination of information, education ►Early warning ► Rational and safe use of medicines 37 WHO Response • WHO promotes global drug safety through its International Drug Monitoring Programme, which began in the 1960s. Through the cooperative effort, Member States and WHO work together to identify possible relationships between the use of a drug and adverse effects. Nearly 100 countries now have national systems in place to report ADRs to the database managed by the WHO Collaborating Centre, the Uppsala Monitoring Centre. When signals of drug safety problems emerge, WHO shares the results with all Member Countries. In addition, WHO: 1. Facilitates regular information exchanges among Member States on the safety and effectiveness of medicines, involving a network of national information officers; 2. Promptly informs national health authorities about new information on serious adverse effects of pharmaceutical products; 3. Provides guidelines to help countries set up national drug monitoring centers; 4. Assists countries as they work to strengthen drug regulatory authorities and reporting systems; 5. Trains health professionals on safety monitoring for new and complex medicines (e.g. antiretrovirals to treat HIV); 6. Draws together regulatory authorities, police, customs officials and38 others to combat counterfeit medicines worldwide. Pharmacovigilance Reporting 39 Pharmacovigilance reporting requirements Learning Objectives: • Identify the minimum criteria for AEM reporting • Identify HCP reports 40 Identifiable Patient Suspect Product Minimum criteria for AEM reporting Adverse Event Identifiable reporting source 41 Components of a case report • Identifiable Patient: At least one of the details should be available (Age, DOB, sex, history, case identification i.e Patient ID) • Product: Clearly refers to name of a drug or biologics or any device • Adverse event: (Sign, symptom, severity, diagnosis, outcome, Action taken, dechallenge, rechallenge, Laboratory data,, drug exposure (Dose, dosage, concoms, Indication, overdose, misuse) • Source: Identifiable reporter (Consumer/Patient, Legal source) Case follow-up for missing data 42 43 Who Can Report? - Any healthcare professional including Physicians, Dentists, Nurses, and Pharmacists, Coroners - Voluntary registers - Pharmaceutical Firms - ADR Reporting systems/Camps - Employees of physician or other HCP who contact the company n behalf of physician - HCP by local regulations (Physician assistant in US, Psychologist in Germany) - Literature reports from medical and scientific journals - Clinical study report - Regulatory agency reports (except where the reporter to the regulatory agency is identified not to b an HCP i.e. like consumer) - Dr. Specialist, (Reports from unidentifiable experts) - Other occupations/qualifications not previously mentioned44 How to Report AEM or AE Reporting Form: • Individually developed by each country that has set up a Pharmacovigilance Centre • To be effective should be available in the local language with features relating it to the responsible authority e.g. a logo, and the address and contact details of the issuing institution Other options for reporting • Telephone. Report receiver should have a reporting form • E-mail. A written case report submitted by e-mail may be acceptable. Further details can be obtained by follow-up. Reporting forms can be sent to reporters as e-mail attach-ments and faxed or mailed to the Pharmacovigilance Centre when completed. • Fax. Sending reports by fax is equivalent to mailing the report, but faster. A fax machine is a very important asset for a national Pharmacovigilance Centre and its major sentinel sites. • The Internet. An Internet site is a valuable asset for a Pharmacovigilance Centre and a reporting form could be made available for downloading or for completion online (en-tering d4a5ta through web-based data entry) if the site is secure. Of which to report? Medicinal Products covered by Pharmacovigilance activities includes, • Centrally authorised • Authorised through mutual recognition procedure • Purely nationally authorised • New medicinal products (NCE), old medicinal products • Biologicals: vaccines, blood products, others • Herbal medicinal products • Alternative and complementary medicinal “..vegetable pills have taken root in my nose. It was reddish before but now it is carotty” products Morrison’s universal vegetable pills, 1834/148634 What to Report? • » » » » » » » All suspected reactions including Unknown, Unexpected Lack of effect Counterfeiting Resistance Interaction Dependence and abuse Unexpected beneficial effects • Excludes: (At risk and other special scenarios) » Therapeutic failures » Intentional/accidental poisoning, abuse » Errors in administration » Noncompliance For New drugs, Report all suspected reactions including minor ones Quality defects can also lead to ADRs 47 When to report • A report should be completed as soon as possible after the reaction. • It is better to advise reporters not to wait until final results and information such as hospital letters are received. These additional details can be sent to the Pharmacovigilance Centre later as a Follow up item 48 Follow-up when Necessary • All reports of serious events should be followed up if details are incomplete. This may require the involvement of health professionals trained and appointed for this type of work. • Occasionally follow-up information is required to fully assess reports of non-serious events. Follow-up requests should be kept to a minimum because they can act as a deterrent to further reporting. Examples A request for essential missing details; Information on the final outcome; The result of rechallenge; The results of laboratory tests; Postmortem results, from health facilities where autopsy is undertaken. 49 Where To Report • Reports should be sent to the Pharmacovigilance Centre. • If it is not practical to send the forms directly to the centre, it may be necessary to arrange points of collection at other sites as e.g. specific hospitals or clinics. • They should be stored securely to maintain confidentiality. 50 Who are the partners? • • • • • • • • • • Government Industry Hospitals and academia Medical and pharmaceutical associations Poisons information centers Health professionals Patients Consumers Media WHO 51 PVG Reporting 52 PVG Reports Learning Objectives: • Classification of AE reports • Product labeling • Difference between expected and unexpected AES • Causality Assessment • Determine medically confirmed reports • Special case scenarios (EIU, medical devices) • Narrative writing • Regulatory reports 53 Methods in Pharmacovigilance • Spontaneous Reporting: AE report from any unsolicited source (Legal) • Clinical studies • Prescription Event Monitoring (Solicited reports) • Literature reports • Registry reports • Case Control Surveillance • Record Linkage (automated population databases; ‘data mining’) • Medical device complains 54 Advantages of Spontaneous Reporting • Effective! • Wide coverage (‘all patients, all drugs, all adverse reactions’) • Continuous • Rapid • Cheap Limitations of Spontaneous Reporting • Suspicions • Underreporting and bias • Insensitive to type C adverse effects (Chronic) • Drug consumption data available? (denominator) • No quantitative assessment • Comparison of drugs difficult • No proof of causality • Often further study needed (hypothesis testing, evaluation) 55 Product Labeling/Listedness assessment • United States Package Insert (USPI), Core Data Sheet (CD), Summary of Product Characteristics (SPC) IB_2 IB sample 56 Expected Vs. unexpected Expected AEs • Consistent/synonymous with AEs contained in the labeling document • Labeled, listed depending on labeling document used Unexpected AEs • Not consistent/synonymous with AEs contained in the labeling document • Not labeled, unlisted depending on labeling document used 57 Listedness assessment • The safety sections (Undesirable Effects / Adverse Reactions, Warnings and Precautions, Contraindications, Interactions, Overdose, Effects on Pregnancy and Lactation, Effects on Driving and Operating Machinery, Drug Abuse, and Dependence) of the product labeling document are reviewed 58 Listedness assessment • Listedness assessments are based upon the event term as coded. • If the term(s) is not identical to that explicitly stated in the product labeling document, but is medically equivalent, the AE is considered listed. Eg. Ischemic attack Vs Stroke Infarction Vs Myocardial Infarction Chest Pain Vs Angina Breathing difficulties Vs Dyspnoea • If the term(s) is a less severe presentation of a listed term, the AE is considered listed. Eg. Transient Ischemic attack Severe Depression Acute or Chronic Infarction 59 Events Considered To Be Listed • AEs included in the selected product labeling document • AEs identified by the reporter as symptoms or consequences of a listed event (e.g., the listed event of stroke resulting in hemiplegia); • Based on medical judgment, exacerbations of certain AEs (i.e., AEs in which the natural course of the disease include exacerbation/quiescent periods, e.g., asthma, depression); • All AEs in the selected document in cases of drug overdose; • Reactions listed for a product continue to be considered listed even when reported as the consequence of an interaction; and • Fatal SAEs are considered listed when the selected product labeling document specifically indicates that the SAEs could result in death. • “Drug Withdrawal Syndrome” (e.g., applicable to CNS products) if “withdrawal symptoms” are mentioned in the selected document or the AEs occurring upon drug withdrawal are part of the normal signs and symptoms of the disease for which the drug was indicated. 60 Events Considered To Be Unlisted • Events not included in the selected product labeling document; • All clinical study SAEs which are specifically associated with an excipient of a placebo; and • AEs that while included in a more general, listed event add more specificity or are more severe (e.g., ‘infections' in the labeling document would be less specific than ‘E. coli infection’, bacterial septicemia); • Fatal SAEs are considered unlisted when the selected product labeling document does not specifically indicate that the SAEs could result in death. • “Drug Withdrawal Syndrome” if “withdrawal symptoms” are not mentioned in the selected data sheet or the AEs are not part of the normal signs and symptoms of the disease for which the drug was indicated. 61 Class Labeling • If the AE as listed in the product labeling document refers to drug class only, with no specification that the event has been observed with the case suspect product, and is not listed in any other section of the product labeling document, the AE is considered unlisted • Eg. Antihypertensives Diuretics 62 Special Patient Population • If an adult, who does not meet the criteria of a special patient population as identified in the product labeling document, experiences an AE that is listed only in the section of the product labeling document referring to AEs experienced by special patient populations (e.g., pediatric, patients with renal impairment, etc.), then the AE is considered unlisted. 63 Reassessment of Listedness • Reassessment of listedness of event(s) is performed upon receipt of significant follow-up that changes the medical assessment (e.g., an event that becomes fatal or life-threatening). • Reassessment of listedness of event(s) is not performed upon receipt of a follow-up report [where no change in the event(s) is reported], for the sole reason of the product labeling document being updated.64 Causality Assessment A medical judgement made by a qualified medical Practitioner • Is there a reasonable possibility that the serious adverse event Is related to the study or suspect product or clinical trial procedure? 1. How close is the relationship between drug and event? 2. Did the drug cause the event? • • YES -Related NO - Unrelated Final judgment will depends on Company and the reporter 65 Uses and limitation of Causality Assessment • What it can do? - - Decrease disagreement between accessor. Classify uncertainty Mark individual case reports Improve the scientific basis of assessment 66 What it cannot do? • Give and accurate quantitative measurement of the likelihood of a relationship. • Distinguish valid form invalid cases • Quantify the contribution of a drug to the development of an adverse event • Change uncertainty to certainty 67 Methods of Causality Assessment There were several method that can be use to make a causality assessment of ADRs reports. • The literature (9 points of consideration – Morges, Switzerland , 1981) • Probability calculation (Bayes’ Theorem) • Aetiological – Diagnostic Systems (Bénchiou’s group method) • French imputation systems • The European ABO Systems • The US Reasonable Possibility Systems • The Naranjo ADR Probability Scale • WHO Causality Categories 68 The literature (9 points of consideration – Morges, Switzerland , 1981) 1. 2. 3. 4. 5. 6. 7. 8. 9. Drug given prior to event? Reaction at site of application? Drug/ADR interval compatible with the event? ADR immediately follows drug administration and is of acute onset? Rechallenge positive? Dechallenge positive? Were concomitant drugs stopped at the same time? Same adverse reaction to this drug before? Adverse reaction known with the suspected drug? 69 Causality Assessment Not Related [The Adverse Event is clearly not related to the investigational agent(s)] Unlikely Related [The Adverse Event is doubtfully related to the investigational agent(s)] Possibly Related [The Adverse Event may be related to the investigational agent(s)] Probably Related [The Temporal relationship of the onset of the event, relative to the administration of the product, is not reasonable or another cause can by itself explain the occurrence of the event. A clinical event, including laboratory test abnormality, with a temporal relationship to drug administration which makes a causal relationship improbable, and in which other drugs, chemicals or underlying disease provide plausible explanations. Again temporal relationship, relative, however is reasonable but the event could be due to another, equally likely cause. Temporal relationship, relative, reasonable and more likely explained by the product than any other cause Adverse Event is likely related to the investigational agent(s)] Definitely Related [The Adverse Event is clearly related to the investigational agent(s)] Temporal relationship, relative, reasonable and there is no other cause to explain the event. 70 Medically Confirmed • Report received from HCP, confirms the occurrence of AE’s and does not deny the relationship of the confirmed AE’s to the company product Case with at least one serious event will be considered as serious case 71 Special case scenarios • At risk Situation - Not associated with adverse event but involve a circumstance that may increase the patients/subjects risk or developing adverse events (Associated events) Eg. Drug misuse, EIU, Extravasations, Medication error and Overdose • Suspected transmission of infections agent (Any Infections agent or pathogen transmitted via product) • Drug interaction • Lack of Efficacy 72 Narrative Writing • A concise, comprehensive written summary or all clinical and relevant information relating the suspect with the adverse events Key elements: • Source type and follow-up details (initial or FU #) • Patients details • Relevant patient social, medical and drug history • Suspect/Co-suspect product (s) details • Concomitants products • Adverse events in details including outcome, Action taken any treatment received • Diagnosis and relevant laboratory details Narratives should be framed in Chronological order and should comply with the SOPs 73 Narrative Writing • This is a “report type” from a consumer by way of “source type”. This 00 year old male consumer experienced Event or signs or symptoms on “date”. His concomitants includes …..The Relevant history includes……Along with XXX he was also treated with YYY from 00 to 00. As a result of the event, he was hospitalized from 00 to 00. His discharge medications includes.. and the diagnostic report includes…. --------. He was re hospitalized on 00 and he died on the same day. The primary cause of death was noted as …….The secondary cause associated for the death reason were ……..Autopsy results shows …. 74 75 76 77 EDI: Electronic Data Interchange 78 79 COSTART - Coding Symbols for Thesaurus of Adverse Reaction Terms. WHOART - WHO Adverse Reactions Terminology 80 81 82 83 84 85 Safety monitoring in Clinical Trials 86 Decision Tree for Data and Safety Monitoring for Clinical Trials Human Subjects involved? (even if exempted under 45 CFR 46)? YES NO Data and Safety Monitoring Policy and Guidance do not apply Is a Clinical Trial proposed (any Phase) ? YES NO Plan not required Is the Data and Safety Monitoring Plan Acceptable? • Entity responsible for monitoring is identified? and • Policies and procedures for adverse event reporting are described? and • Plan is appropriate with respect to risks to participants, complexity of study design, and methods for data analysis? Regulatory bodies requires a Data and Safety Monitoring Board for multi-site clinical trials of interventions with potential risk to participants. YES ABSENT NO No Information ACCEPTABLE Explain why the data and safety monitoring plan is scientifically acceptable. UNACCEPTABLE Contact Scientific Review Administrator UNACCEPTABLE Negative impact on score. Explain why the data and safety monitoring plan is scientifically unacceptable. 87 Safety Monitoring in Clinical Trials 88 Definitions • Data Safety Monitoring Plan (DSMP) – Describes how the study investigators plan to oversee research subject safety and how adverse events will be characterized and reported – The intensity and frequency of monitoring should be tailored to fit the expected risk level, complexity, and size of the particular study • Data and Safety Monitoring Board (DSMB/DMC) – A group of individuals with pertinent expertise that review on a regular basis accumulating data from ongoing an clinical trial – Advises sponsor regarding safety of current and future participants and validity and scientific merit of the trial 89 Study Risk Definitions Minimal-risk: Non-therapeutic trials such as survey research, questionnaires, blood samples, or observations. One standard definition is: A study where the magnitude of harm or discomfort is not greater than that encountered in daily life or the performance of routine physical or psychological examinations or tests. Moderate-risk: Phase II or phase III multi-intuitional industry sponsored trials with independent data monitoring High-risk: Clinical trials with investigational agents, phase I clinical protocols, investigator initiated INDs, manufacturing of product on campus, some phase II clinical trials, and investigator initiated phase III clinical trials. 90 Which Studies Require DSMB? Clinical Research? Yes No Phase III or Multicenter Yes No Blinded, high-risk intervention, or vulnerable population? Yes IRB + DSMP + DSMB No IRB + DSMP 91 DSMB Checklist Preliminary DSMP Checklist 1) 2) 3) 4) 5) 6) 7) 8) Is some form of study risk assessment? Is there a description of the anticipated adverse events? Is there a description of how adverse events will be detected and monitored at a research subject level? Is there an adverse event grading and attribution scale described? Is there a plan for the reporting of adverse events? Is there a plan for annual reporting of adverse events? Is there a description of who will be performing safety reviews for the study and how often these will be reviewed? Has preliminary criteria for decision making regarding continuation, modification or termination of the clinical study been documented 92 Regulatory reports • • • • • 15-Day NDA Report CIOMS 1 Report NDA Periodic Report IND Annual report Periodic Safety Update Report (PSUR) • Med watch report 93 15-Day NDA Report • Non-clinical study cases for a marketed product and clinical study cases for an investigation product with an active NDA • AE- serious, unexpected and related • Reference Labeling document • Due date: 15 calendar day from the company receipt date • Submitted to US FDA 94 CIOMS-1 Report • Council for International Organizations of Medical Sciences • AE = Serious and Related • Reference labeling document: Not applicable • Due date: 12 calendar days from company receipt date • For licensed product report has to be generated to the respected company in the stipulated time 95 NDA Periodic report • Required for all FDA-approved marketed drugs • Includes a compilation of all non-15 day AE reports that have occurred in the US and a listing of 15-day submitted reports • Due date: Quarterly for the 1st 3 yrs following date of FDA approval of an NDA and annually thereafter • Submitted to USFDA 96 IND Annual Report • Required for all drugs for which an IND has been opened • Due date : 60 days following the effective anniversary date • Submitted to the US FDA 97 Periodic safety update report (PSUR) • • 1. 2. 3. 4. 5. The PSUR is a practical mechanism for summarizing interval safety data covering short periods of time and for conducting and overall safety evaluation Includes All serious, non clinical trial cases from a HCP All Nonserious, non clinical trial cases with unlisted AEs from a HCP Clinical trial cases with a casual relationship with the study drug All solicited cases from a HCP with a casual relationship with the subject drug HCP EIU cases 98 LEGISLATIVE REPORTING REQUIREMENTS To the Sponsor, MHRA (Medicines and Healthcare products Regulatory Agency), Ethics Committee, all other investigators, (must include a causality assessment): • Fatal life/threatening SUSARs = within 7 days. • All other SUSARs = No later than 15 calendar days. 99 SIGNAL DETECTION 100 Data assessment in Pharmacovigilance • • • • • • Individual case report assessment Aggregated assessment and interpretation Signal detection Interactions and risk factors Serial (clinicopathological) study Frequency estimation 101 Signal Detection • “An alert from any available source that a drug may be associated with a previously unrecognized hazard or that a known hazard may be quantitatively (more frequent) or qualitatively (e.g., more serious) different from existing expectations” • Minimum requirement: Single, well documented report with a positive rechallenge or replication of findings in a series of reports SNIP Rule for signals: » » » » Wish to examine signals that are: Strong New Important Preventable 102 WHO-UMC definition of a signal • Reported information on a possible causal relationship between an adverse event and a drug, the relationship being unknown or incompletely documented previously. Usually more than a single report is required to generate a signal, depending upon the seriousness of the event and the quality of the information. • Edwards IR, BiriellC. Drug Safety 1994;10:93102 103 A signal consists of • Hypothesis • Data • Arguments, in favor or against 104 Data of a signal • Qualitative (clinical) • Quantitative (epidemiological) • Experimental’ • Develops over time 105 1. Signal detection • Selection of a possibly relevant association (hypothesis generation) • Preliminary assessment of the available evidence (signal strengthening) 2. Signal follow-up 106 Criteria for selecting a signal • • • • • • • • • • • • • • • • • • Unknown adverse reaction Unexpected Expected but ‘unlabelled’ Strong statistical connection Low background frequency Specific, characteristic Objective (definitive) event Typically drug-related event or Critical Term Serious High potential relevance Known (and labelled) Weak statistical connection High background frequency Unspecific, trivial event Subjective event Common disorder, e.g. infectious or ‘endogenous’ Not serious Low relevance 107 When is a signal likely to be relevant? • • • • • • • • • Early Warning New adverse reaction; new drug Public health perspective Important drug (serious indication; widely used) Serious reaction Large number of cases; rapid increase in reporting Regulatory intervention (prevention) Change in benefit/risk Scientific or educational value 108 Signal follow-up (same database) • Drug exposure • Development over time of the quantitative data and the consistency of the pattern • Signal strengthening –individual case report assessment –reporting distribution –‘best case-worst case’scenario –targeted comparisons –nested case control studies 109 Signal follow-up (other sources) • Similar connection in other countries • WHO-UMC international database, • Additional observations (e.g. literature, registration file, other databases) • Experimental data (e.g. pharmacological, immunological) 110 The balance of evidence in a signal Quantitative strength of the association –number of case reports –statistical disproportionality –drug exposure • Consistency of the data (pattern) • Exposure-response relationship –site, timing, dose, reversibility • Biological plausibility of hypothesis –pharmacological, pathological • Experimental findings –e.g. dechallenge, rechallenge, blood levels, metabolites, drugdependentantibodies • Analogies • Nature and quality of the data –objectivity, documentation, causality assessment 111 From signal to action • Internal communication (national centers, UMC, company, academia) • Initiation of further study (signal testing) • Regulatory action (e.g. data sheet change) • External communication (drug information centers, national drug bulletin, publications) 112 Signal detection using a neural network approach • If the Posterior probability > Prior probability – The drug ADR combination is present more often than expected – This is represented by a high value of Information Component (IC) – IC=log2 (Posterior Probability/ Prior Probability) 113 Automated quantitative signal detection • Extremely large numbers ofdrug adverse reaction combinations • Selects automatically high-interest combinations, using quantitative disproportionality • Manageable subsets of data • No human time needed • No investigators bias • Objective, transparent, reproducible • Flexible / adjustable • Explorative 114 Signal Detection at the Uppsala Monitoring Centre Eur J Clin Pharmacol 1998;54:315-321 • • • A combination of automated quantitative data mining, using Bayesian statistics and a neural network architecture (Information Component – ‘IC value’) ‘Triage’ Human assessment – National Centres – Review Panel – UMC staff 115 The SIGNAL document • Sent to all National Centres (national distribution) • Individualized section available to industry • All recipients encouraged to comment on topics presented 116 Statistical analysis • Allows pattern recognition in large amounts of data • Also incomplete case data of value • Allows identificaion of interactions and syndromes 117 Risk Benefit Analysis • Risk-benefit analysis is the comparison of the risk of a situation to its related benefits • For research that involves more than minimal risk of harm to the subjects, the investigator must assure that the amount of benefit clearly outweighs the amount of risk • Only if there is favorable risk benefit ratio, a study may be considered ethical • The Helsinki Declaration [1] and the CONSORT statement [2] stress a favorable risk benefit ratio • Risk must include: Physical – death, disability; Psychological – depression and anxiety; Social – discrimination; Economical – job less 118 Benefit/risk evaluation Edit product information: • • • • • • • • Indications/use Dosing instructions Contra-indications Interactions Pregnancy/lactation Warnings/precautions Undesirable effects Over dosage Withdraw marketing authorisation 119 120 121 122 123 124 Regulatory Bodies 125 WHO Collaborating Centre for International Drug Monitoring The Uppsala Monitoring Centre Stora Torget 3, 75320 Uppsala, Sweden www.who-umc.org 126 The Uppsala Monitoring Centre • 1968 - WHO Collaborating Centre for International Drug Monitoring, Geneva • 1978 - Moved to Uppsala after agreement between Sweden and WHO • Non-profit foundation with international administrative board • WHO Headquarters responsible for policy • Self-financing • Global pharmacovigilance • Around 100 national Pharmaco-vigilance Centers around the world 127 128 Pharmacovigilance regulations • Medicines for Human Use Clinical Trials Regulations 2004 - legal requirements • EU directive and detailed guidance required harmonisation of laws- some flexibility • Internationally accepted principles of good clinical/trial practice, data management, reporting E3, E6, E8, E2A 129 Pharmacovigilance in practice • All protocols must have a PV section • Risk to patients varies in the range of clinical trials. Extent of recording and notification of adverse events may vary depending on knowledge of the risks and benefits of drugs under study and aims of the trial. • Responsibilities and systems to deal with recording, assessment and reporting must be clearly stated. • Time frames for notification, assessment and reporting are critical • As are SOPs 130 ICH Topics relevant to Pharmacovigilance E2, Clinical Safety • E2A, Definitions and Standards for Expedited Reporting E2B, Data Elements for • Transmission of ADR reports E2C, Periodic Safety Update • Reports E2E, Pharmacovigilance planning • 131 ICH Topics relevant to Pharmacovigilance • M1, Medical Terminology (MedDRA) • M2, Electronic Standards for the Transfer and Data of Regulatory Information (ESTRI) • M5, Data Elements and Standards for Drug Dictionaries 132 E2E-Pharmacovigilance planning • Pharmacovigilance Specification is a summary of the: –Important identified risks, –Important potential risks, and –Important missing information about a product. 133 Concept of E2E Guideline Clinical Trials Available Data/information NDA Approval Review Product Launch On the Market Pharmacovigilance Specification Pharmacovigilance Activities Pharmacovigilance Plan 134 Pharmacovigilance and India • India has become a major hub for clinical trials. However, whether patients in India receive safe drugs or not is still very much in question • India's Drugs Control Department within the Ministry of Health & Family Welfare initiated the establishment of a nationwide network to build a comprehensive Pharmacovigilance data system in 2004; Different PV regional centers have been listed in the below site. http://www.pharmacovigilance.co.in/home.html 135 National PVG Programme National Parmacovigilance Center: Office of the Drugs Controller General of India Central Drugs Standard Control Organization, (Directorate General of Health Services), Ministry of Health & Family Welfare Government of India National PVig Center Zonal Center 1: for North and Zonal Center 2: for West and South Regions East Regions NE Zonal N Regional E Regional SW Zonal W Regional S Regional 136 Where to report Local ADR Reporting Centre Peripheral Pharmacovigilance Centre Zonal Pharmacovigilance Centre – Statistical Regional Pharmacovigilance Centre – Causality Central Drug Standardization Control Organization The International Pharmacovigilance Database managed by WHOUPPSALA monitoring Centre in Sweden 137 Pharmacoepidemiology • • Study of the use and effects of drugs in large groups of people Pharmacoepidemiology benefits from the methodology developed in general epidemiology and may further develop them for applications of such methodology unique to Pharmacoepidemiology. Epidemiology can be defined as the study of the distribution and determinants of diseases in populations. Epidemiological studies can be divided into two main types: • – Descriptive epidemiology describes disease and/or exposure and may consist of calculating rates, e.g., incidence and prevalence. Such descriptive studies do not use control groups and can only generate hypotheses, not test them. Studies of drug use would generally fall under descriptive studies. Analytic epidemiology includes two types of studies: – observational studies, such as case-control and cohort studies, and – experimental studies which would include clinical trials such as randomised clinical trials. The analytic studies compare an exposed group with a control group and are usually designed as hypothesis testing studies 138 Infrastructure requirements in practicing Pharmacovigilance and Pharmacoepidemiology •Good pharmacovigilance practice is based on acquiring complete data from spontaneous adverse event reports, also known as case reports. The reports are used to develop case series for interpretation. •Effective pharmacovigilance is dependent on the availability of information on the clinical effects of medicines in representative populations, as used in normal practice. For this to happen, it requires a robust pharmacovigilance system, which includes a system of collecting and monitoring suspected ADRs and processes for reviewing the data to decide whether further investigations are necessary. 139 AE Case Processing AE Reporting Forms • AEM Form: ADVERSE EVENT MONITORING (REPORT) AEM Form Adobe Acrobat 7.0 Document • CIOMS Form Adobe Acrobat 7.0 Document • Medwatch Form Microsoft Word Document Adobe Acrobat 7.0 Document Action Taken with Drug • Action Taken with Drug: – Withdrawn (Temporarily/Permanent) – Dose reduced – Dose increased – Dose not changed – Post therapy – Unknown – Not applicable • ICH E2B (R3) Dechallenge - Rechallenge Definitions • Dechallenge – withdrawing the drug(s) and recording the outcome – improved or not improved • Rechallenge – giving one drug again under the same conditions as before and recording the outcome – recurrence or no recurrence. Dechallenge Dechallenge = withdrawal of drug “Positive” dechallenge = improvement of reaction when dechallenge occurs. Resolution of suspected ADR when the drug is withdrawn is a strong, although not conclusive indication of drug-induced reaction. Rechallenge Rechallenge: Reintroducing the drug after a dechallenge •Positive rechallenge (symptoms re-occurring on readministration) •negative rechallenge (failure of a symptom to re-occur after re-administration) •Rechallenge is only justifiable when the benefit of reintroducing the drug to the patient outweighs the risk of recurrence of the reaction. This is rare. In some cases the reaction may be more severe on repeated exposure. Rechallenge therefore requires serious ethical considerations. Outcome • Outcome of reaction/event at the time of last observation – – – – – – Recovered/resolved Recovering/resolving Not recovered/not resolved Recovered/resolved with sequelae Fatal Unknown – – – – Remains in Study Withdrawn Lost to follow-up Death • Outcome of subject in study 147 Case 1 A 42-year-old female experienced vomiting during treatment with 200mcg Pulmicort at night by inhalation for her asthma. The onset of the reaction was on 3rd August 2006 until 5th August 2006. She been prescribed this drug since end of July. The drug was stopped on the 5th of August and patient recovered. No rechallenge performed and her doctor change the drug. Case 2 • A 68-year-old male patient was started with Crestor on the 29th Jan. 2007 for his hyperlipidaemia. On the 2nd of Feb. 07, patient felt very ill. Upon admission, the diagnosis was myositis and abnormal hepatic function (ALT: 100 units/ml). Patient also took Sandimmun Neoral for his bone – marrow transplant rejection since October 2006. Crestor was discontinued and patient recovered a few days later. No rechallenge been performed. Case 3 • A 67-year-old woman reported , whose medical history included diabetes mellitus, hypertension and also been diagnose with Alzheimer’s Disease. This woman been on long term treatment of Amlodipine 5mg/daily, Metformin 1gm/bd and Glibenclamide 5mg/bd. She started receiving daily oral Exelon® (Rivastigmine) 6mg daily. After 5 months she was hospitalised for dizziness and syncope. On admission her BP was 90/60mm Hg, her pulse rate was 34 beats/min, and complete heart block was evident on 12 lead ECG. • The woman received a temporary transvenous pacemaker, and Exelon® and amlodipine was discontinued. Angiography showed normal coronary anatomy. After 3 days admission her heart block spontaneously resolved and sinus rhythm was restored. • Oral Exelon® was restarted that day, and complete heart block recurred on day 4. the woman received a VVI permanent pacemaker the following day. Amlodipine was restarted and Exelon® was continued at the same dosage. She had not experienced further syncopic episodes or dizziness at follow up 3 months later.