Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
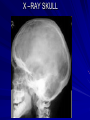
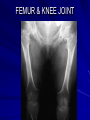
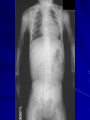
ACHONDROPLASIA DR. O.KUMARESAN SMCH, CHENNAI ANAESTHETIC MANAGEMENT OF FAMILIAL ACHONDROPLASTIC DWARF This report describes the successful management of a 20 year old female miss.Jothi, a familial achondroplastic dwarf with height of 120 cm and weight of 38kg taken up for emergency appendicectomy. Procedure was done under endotracheal tube general anaesthesia with controlled ventilation. CASE REPORT While assessing, no relevant medical or surgical history was found. Physical examination revealed her height as 120 cm and weight 38 kg with typical features of achondroplasia Relatively large head with short limbs, mild kyphoscoliosis of the thoracolumbar spine, impalpable Lumbar vertebrae, short neck with limited extention,<30* mouth opening adequate, airway III (MPC), trachea midline and normal chest movements. peripheral IV access was difficult due to excessive soft tissues. Other systems and parameters were normal CASE REPORT contd Pre operative investigations were normal with Hb of 10gm. In the operation theatre, the patient was monitored with pulse oximeter, ECG and NIBP. With difficulty , left Basilic vein was cannulated with an 18 G IV cannula. ETGA with IPPV was planned. Emergency Airway management cart kept ready. Started with premed inj. Glycopyrrolate 0.2 mg. IV ; Inj. Midazolam 1 mg. IV ; Inj. Fentanyl 80 mic.gm. IV. Pre oxygenation was done for 5 minutes. CASE REPORT contd Anaesthesia was induced with inj. Propofol 80 mg IV. Inj. Suxamethonium 80 mg. IV was used to facilitate the insertion of 6.5 mm cuffed oral ETT. Intubation was difficult because of restricted neck movements. Cormack and lehane”s grade 2 view Managed with Optimal External Laryngeal Manipulation . Anaesthesia was maintained with nitrous oxide 4 Ltrs and oxygen 2 Ltrs in Closed circuit. Atracurium was used as muscle relaxant. Intraop vitals were stable. Procedure lasted for 70 minutes. Intraoperatively 700ml of IV crystalloids was given. CASE REPORT contd Reversal of residual paralysis was done with neostigmine 2.0mg and glycopyrrolate 0.4mg IV. Spontaneos ventilation was quickly established. After extubation patient was given 100%oxygen by face mask for 10 minutes. Patient was monitored and remained clinically well. Post operatively Inj. Diclofenac 50 mg IM thrice a day was given for analgesia. Patient was given chest physiotherapy to avoid post operative respiratory complications. DWARFISM abnormal underdevelopment of the body, characterized predominantly by extreme shortness of stature, associated with numerous other defects and may involve varying degrees of mental retardation. Dwarfism has multiple causes, including genetic defects, endocrine dysfunction involving either the pituitary or the thyroid gland, chronic diseases such as rickets, renal failure, intestinal malabsorption defects, and psychosocial stress, as in the maternal deprivation syndrome. The Little People of America (LPA) define dwarfism as an adult height of 148 cm (4 feet 10 inches) or less. Also known as nanism. Dwarfism is now more correctly called short stature. ACHONDROPLASIA Non-lethal form of short limbed dwarfism presenting at birth (rhizomelic form-proximal shortening) with an incidence of 0.5 – 1.5 / 10,000 live births. Transmission is by an autosomal dominant gene. 80% spontaneous mutation 20% are familial mutation in the FGFR-3 gene. The commonest form of dwarfism and a relatively rare condition. normal periosteal bone deposition coupled with failure of endochondral bone formation. Abnormolities in chondrogenesis and osteogenesis. ACHONDROPLASIA contd Mental functions and muscular development are normal with low fertility rates. Pre maturity is frequent but those surviving first year of life generally have a normal life expectancy Due to overall appearance employed as clowns in the circus ACHONDROPLASIA contd Orthopedic problems Disparity between axial & appendicular skeleton Tubular bones – short & wide abnormal metaphysis skull base uder developed Sternal prominence with pectus carinatum Narrow pelvic outlet kyphoscoliosis and genuvarum are common. Flexion contracture of hip Trident hand ACHONDROPLASIA contd Hallmark- progressive narrowing of interpedicular distance in the lumbarspine towards caudal direction SURGERIES limb lengthening procedures Surgical Decompression- for narrow spinal canal Realignment osteotomies-genu varum SPINAL STENOSIS X –RAY SKULL X-RAY CHEST SPINE & RIBS FEMUR & KNEE JOINT HUMERUS HANDS GENERAL ANAESTHESIA Anaesthesia-both regional and general pose problems for Achondroplastic dwarf. The intubation may be difficult due to craniofacial deformity, restricted neck movements, short neck, large tongue, small larynx Hence a small ETT may be required. GENERAL ANAESTHESIA Review of data by MAYHEW et al suggest that age based formula for selecting ETT size for children is. Tube size (mm ID) = [ Age (Yr) + 16 ] / 4 predicts correct size. These patients also have narrow nasal passages and pharyngeal hypoplasia as a result of dysplasia and angulation of cranial base. Sternal prominence with pectus carinatum interfere with midline positioning of laryngoscope. Hence the use of laryngoscope with small handle is indicated. GENERAL ANAESTHESIA Hyperextension of neck should be avoided to prevent cord compression because foramen magnum stenosis is common. Requirement of drugs including inducing agents and relaxants is judged on body weight basis. Patients may have restrictive lung disease from rib hypoplasia, thoracic lordosis, leading to corpulmonale. Central and obstructive sleep apnoea is common. Because of all these factors adequate post operative physiotherapy is needed REGIONAL ANAESTHESIA Regional anaesthesia may be technically difficult because of poor landmarks. A relatively narrow spinal canal may result in cord compression. Prolapsed discs and deformed vertebral bodies are common in elderly Achondroplastics. The possibility of herniation with neurological symptoms and paraplegia may be against the use of regional techniques. REGIONAL ANAESTHESIA A narrow epidural space makes catheter insertion difficult and inadvertent subarachnoid tap is likely. SAB-results unpredictable level Recognition of subarachnoid tap may be difficult because free flow of CSF is difficult due to foramen magnum stenosis REGIONAL ANAESTHESIA Epidural Anaesthesia is preferable to SAB because it helps in titration of dose of LA according to height of block. Incremental dosage also prevents marked hypotension and its associated complications. Anxiety may be greater for these patients than normal persons. Hence the need for a good rapport between the Anesthesiologist and the patient. CONCLUSION The anaesthetic management of Achondroplastic dwarf is a challenge. All patients must be assessed preoperatively to identify possible hazards. The benefits and risks of GA and RA must be considered. TAKE CARE OF THE AGE RATHER THAN THE SIZE OF THE PATiIENT THANK YOU