Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
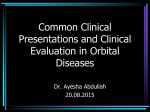
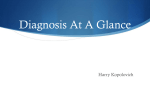
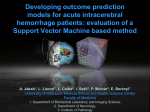
Case Report Orbital Hematoma with Extradural Hematoma Presentating as Acute Proptosis following Head Injury - A Rare Case Report Dr. Pradeep Reddy, Dr Vipul Arora, Dr. Usha Kim, Dr. P.Subburam, Aravind Eye Hospital, Madurai Introduction Post traumatic proptosis due to orbital subperiosteal hematoma is an uncommon entity. We report a very rare case of post traumatic simultaneous occurrence of subfrontal extradural hematoma and orbital subperiosteal hematoma with orbital roof fracture following head injury in a 15 year old boy. This association has been reported previously in only 10 cases and only one report has appeared in the ophthalmic literature.(1-2) This case report highlights the rarity of the combination of the pathological lesions, and the need for having a high index of suspicion of such, in a patient presenting with post traumatic Proptosis and orbital roof fracture. Case Report A 15-year-old village boy presented to our hospital complaining of left-sided Proptosis, pain and diplopia for the past 6 days. He sustained head injury after a 3 meter fall from tree 13 days prior. He had a lacerated wound at left temporal region and left supraorbital region for which suturing was done by local surgeon. He was observed for 24 hours for any neurological deficit and then discharged. After 6 days he developed gradually progressive left eye proptosis, pain and diplopia. On examination the patient was fully conscious with a normal affect and a Glasgow coma scale of 15/15. He had no neck stiffness, cranial nerve palsy, or any other localising signs. The visual acuity in the right eye was 6/9 and in the left 6/60. On the left, non-axial proptosis measuring 6 mm forwards, 5 mm downwards and Fig : 1 (showing left eye gross eccentric proptosis) 5 mm laterally was present (fig1). Proptosis had no bruit, non posture dependent, and no change with the valsalva maneuver. Eyelids were unable to close because of gross proptosis and chemosis leading to corneal epithelial defect and crusting. Pupils were normal and reacting. There was marked limitation of elevation and depression, slight limitation of abduction, and adduction. As the cornea was hazy, fundus details were not made. Axial section Coronal section Extradural hematoma (5.75 x 4.53 x 3.30cm) Superior subperiosteal hematoma of orbital roof (3.44 x 2.73 x 2.24cm) Fig: 2 (CT showing left frontal extradural haemorrhage & left superior orbital subperiosteal haemorrhage) 24 Computed tomography demonstrated a superio-medially located orbital subperiosteal hematoma (measuring 3.44 x 2.73 x 2.24cm), in continuity with sub frontal extradural haematoma (measuring 5.75 x 4.53 x 3.30 cm) through the undisplaced orbital roof fracture in the left side (fig 2). Patient underwent left frontal craniotomy, and a thick solid clot overlying floor of anterior cranial fossa was evacuated (fig 3). However we could not find the orbital roof fracture on table. Superior orbitotomy was done and orbital subperiosteal hematoma evacuated. Proptosis disappeared immediately and periorbital swelling subsided over a period of one week. Postoperatively the patient Fig : 3 (Intraoperative) Fig:4 (Post-operative) made an uneventful recovery with no neurological deficit, normal vision and fundus (fig 4). Discussion The differential diagnosis of acute proptosis after head injury includes fracture of orbit with retrobulbar haemorrhage, laceration and rupture of the tissues of the orbit and extra ocular muscle, AECS Illumination carotid cavernous aneurysm in orbit. Post traumatic progressive proptosis developing due to subperiosteal haematoma is uncommon and even rare is its association with sub frontal extradural haemorrhage (3-4). Extradural hematoma comprises about 1-2% of head trauma admission.(5).Extradural hematomas mainly results due to bleeding from the epidural vessels or the draining emissary vein. (6) An extradural haematoma is a life-threatening condition with a mortality rate in children is upto 50% (7). The clinical features of an extradural haematoma include headache, vomiting, drowsiness, loss of consciousness. Normal mental status and normal neurological examination in the presence of an extradural hematoma is extremely rare (8). Of the previous reported case except one all had loss of consciousness. C R Stewart, J F Salmon, Z Domingo, A D Murray reported a similar case with proptosis and headache in BJO (2). But in our case patient presented with only proptosis and diplopia. Orbital subperiosteal hematoma presenting as proptosis may be spontaneous or traumatic in origin. The spontaneous hematoma is very rare (9). Subperiosteal hematomas of the orbit typically are a result of trauma to the head region. Roof of the orbit is the most commonly involved site and is more often seen in young males (10). Subperiosteal hematomas on the roof of the orbit can be explained as the frontal bone forms the largest continuous concave bone surface of the orbit and also orbital periosteum is not firmly attached to the bony surfaces except at its suture lines. It may or may not be associated with orbital roof fracture. A somewhat delayed occurrence seems to be another typical feature of subperiosteal hematoma of the roof of the orbit (11). In our case also the child presented late that was after one week. Simultaneous occurrence of the subfrontal extradural hematoma and subperiosteal hematoma is very rare. Out of 8, one case was having bilateral subperiosteal hematoma with subfrontal extradural hematoma (12). As seen in our case Vol. XIV, No.4, October - December 2014 many times size of the extradural hematoma is bigger than the orbital subperiosteal hematoma (10/13). Thus, the primary site of bleeding is at subfrontal region either due to rupture of a dural artery or an emissary vein and associated subperiosteal hematoma is due to stripping of the periorbita because of the orbital roof fracture or seepage of blood through the fracture site from subfrontal extradural hematoma. In our patient, proptosis was caused by a subperiosteal hematoma extending from a subfrontal extradural hematoma through an orbital roof fracture. This case illustrates that an extradural hematoma along with orbital subperiosteal hematoma can also be one possibility for post traumatic proptosis even in the absence of neurological signs. C.T scanning of the orbit 25 and cranium is mandatory before embarking on emergency orbital surgery. Thus the scan not only reveals the orbital anatomy in detail but also gives the opportunity to rule out any associated intracranial hematoma which may alter the surgical plan. It is important to diagnose early extadural hematoma as it has high mortality. Delayed diagnosis of orbital subperiosteal hematoma may compromise visual function (13) either due to exposure keratopathy (as in our case) or compression of optic nerve. So it requires an emergency surgical intervention for evacuation of extradural hematoma through frontal craniotomy and also subperiosteal hematoma via front-superior orbitotomy simultaneously, thus preventing further complications. References 1. Sinkiewicz A, Kasprzak H,Kachki. Epidural hematoma with unilateral exophthalmos Neurol Neurochir Pol. 1992;Suppl 1:349-52. 2. C R Stewart, J F Salmon, Z Domingo, A D Murray. Proptosis as a presenting sign of extradural hematoma..British Journal of Ophthalmology 1993;77:179-180. 3. Batuk Diyora DNB (Neuro), Alok Sharma M Ch, Kaushik Patel MS.Simultaneous occurrence of traumatic subfrontal extradural hematoma with orbital subperiosteal hematoma Indian Journal of Neurotrauma 2006, Vol. 3, No. 2, pp. 139-141. 4. Umansky F, Pomenanz S. Epidural haematoma and unilateral exophthalmos. A review, Acta Neurochir(Wein)1989;99:145-7. 5. Sharma AK, Diyora BD, Shah SG, Pandey AK, Sayal PP,Ingale HA, et al Orbital subperiosteal hematoma associated with sub frontal extradural hematoma J Trauma 2007;62:523-5. 6. Stephanov S, de Preux J. Acute subfrontal epidural hematoma: Report of two cases. Surg Neurol 1992; 37:329-31. 7. Pasaoglu A, Orhon C, Koc K, Selcuklu A, Akdemir H, Uzunoglu H Traumatic extradural haematomas in pediatric age group. Acta Neurochir(Wien) 1990; 106: 136-9. 8. Snyder HS, Salo D. Epidural hematoma: an unusual presentation. AmJ EmergMed 1990; 8: 538-41 9. Gruszkiewicz J. Ipsilateral exophthalmos in subfrontal epidural hematomas. Report of four cases. J Neurosurg 37; 613-5. 10.. J. Reimer Wolter, MD Subperiosteal hematomas of the orbit in young males. Trans Am Ophthalmol Soc. 1979; 77: 104–120. 11.Costa JR, Leodante Batista da, Andrade et al. Traumatic bilateral intraorbital hematoma associated with epidural hematoma: Case report. Arg Neuro-P siquiatr 2003;61:1039-41. 12.Nakai K, Doi E, Kuriyama T, Tanaka Y. Spontaneous subperiosteal hematoma of the orbit. Surg Neurol 1983; 20:100-2