Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
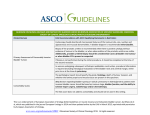
BLADDER CANCER 7 Management of muscle-invasive bladder cancer ANDREW MOON, HANS VAN DER VOET AND JO CRESSWELL Cancer that has invaded the detrusor muscle can be associated with a high degree of morbidity and mortality. Radical treatments are required, including cystectomy, radiotherapy and chemotherapy. These treatments can cause short-term and long-term consequences for patients. In this article the authors describe the current treatment approaches to muscle-invasive bladder cancer. © Steve Gschmeissner/Science Photo Library B ladder cancer can be clinically classified by stage as either non-muscle invasive (NMIBC) or muscle invasive (MIBC) based on the involvement of the detrusor muscle (Figure 1). Approximately 20% of bladder tumours are muscle invasive at presentation, requiring radical treatment. Tumour grade is also a well-established predictor of disease progression and bladder cancer specific mortality.1,2 High-grade bladder tumours present a significant risk in terms of disease recurrence, local invasion and metastasis, and are responsible for the high degree of morbidity and mortality associated with bladder cancer.3 High-risk NMIBC can progress to MIBC, and the prognosis is thought to be poorer for progressive disease compared to primary MIBC.4 In the UK, the majority of bladder cancers are transitional cell carcinomas, but there are variants, such as squamous cell carcinoma, adenocarcinoma and small cell cancer, which require different treatment strategies.5 TREATING MUSCLE INVASIVE BLADDER CANCER NICE has recently published guidelines for the management of bladder cancer.6 TRENDS IN UROLOGY & MEN’S HEALTH The patient should be reviewed in clinic following discussion and review of histology and staging radiology results at the uro-oncology MDT. A thorough assessment of the patient’s cardiac and respiratory function and exercise tolerance NOVEMBER/DECEMBER 2015 Andrew Moon, Urology Specialist Registrar; Hans Van der Voet, Consultant Oncologist; Jo Cresswell, Consultant Urologist, James Cook University Hospital, Middlesbrough www.trendsinmenshealth.com BLADDER CANCER 8 should be made, and renal function (eGFR) should also be assessed. These assessments will help inform both the patient and the clinical team about the risks posed by major surgery and the potential for chemotherapy. Patients should be counselled by the bladder cancer team (comprising the urologist performing cystectomy, a clinical oncologist and a nurse specialist) with regard to their treatment options, which include radical cystectomy (RC) with an ileal conduit or neobladder formation, or radical chemoradiotherapy (CRT). Both treatment options may be preceded by neoadjuvant chemotherapy (NAC), which has shown a 5% improvement in survival at 5 years.7 At the present time, there are no randomised controlled trials comparing the effectiveness of radical cystectomy and CRT. The patient should have the opportunity to discuss surgery and bladder sparing options in detail, including the risks of each procedure. More advanced cases may be offered palliative radiotherapy, which can ease symptoms such as bleeding and pain. Metastatic disease is managed with systemic chemotherapy. RADICAL CYSTECTOMY RC has long been considered the standard method of care for MIBC. It usually includes the complete surgical removal of the bladder and prostate in males and the bladder, uterus and part of the vagina in females. Pelvic lymphadenectomy is also performed and may provide both diagnostic and therapeutic benefit. Two randomised clinical trials – the LEA study in Germany and SWOG (South West Oncology Group) BLOG Read Rik Bryan and Nick James’ blog on ‘The appropriate management of muscle-invasive bladder cancer in the elderly’: www.trendsinmenshealth.com/blog www.trendsinmenshealth.com Ureters 0is or CIS Fat 0a Stage 1 Muscle Stage 2 Connective tissue Stage 3 Bladder lining (urothelium) Stage 4 Figure 1. Bladder cancer staging is based on the degree of invasion through the detrusor muscle wall (reproduced with permission from Macmillan Cancer Support) 1011 study in the USA – are evaluating the extent of lymph node dissection required and the impact on cancer control. RC is associated with significant morbidity and mortality. However, improvements in technique and perioperative care have reduced the 90-day mortality rate to 2.1% of patients.8,9 Overall complication rates, when collected meticulously and prospectively, are approximately 60%.10 The procedure carries a significant risk of bleeding requiring blood transfusion.10 In addition, infection in the surgical wound, chest or pelvis can occur. Other complications, including small bowel anastomotic leak, uretero-ileal anastomotic leakage, rectal injury, deep vein thrombosis, pulmonary embolism, stroke, myocardial infarction, and disease recurrence, must all be discussed with the patient. Recent trials with laparoscopic and robotic RC have also been described. These techniques appear to have similar morbidities, oncological and functional outcomes as open approaches.9,10 Blood loss and transfusion rates are lower with minimally invasive surgery, but operative times may be longer than for open surgery. The experience of the operator is an important factor, as with all surgical procedures. Figueroa et al demonstrated that elderly patients (>70 years) with few comorbidities recovered following RC with clinical and functional results similar to younger patients.11 Contemporary surgical series (without NAC) have shown 5-year overall, recurrence-free and cancer-specific survival rates of 57.9%, 69.5% and 71.2%, respectively.12 URINARY DIVERSION Following removal of the bladder during RC, an ileal conduit or neobladder reconstruction is formed. Ileal conduit is the most commonly used method of urinary diversion in the UK (80%) and involves anastomosing the ureters to an isolated piece of distal ileum.13 The distal end is then mobilised and brought out as stoma on the right side of the abdomen (Figure 2). Patients who require an ileal conduit need to be aware of the associated TRENDS IN UROLOGY & MEN’S HEALTH NOVEMBER/DECEMBER 2015 BLADDER CANCER 9 Kidney Ureter Early Late Metabolic Ileus Stomal stenosis Hyperchloraemic metabolic acidosis Bowel obstruction Para-stomal hernia Macrocytic anaemia Anastomotic leakage Uretero-ileal stenosis Ischaemia of conduit Skin excoriation Table 1. Potential complications following ileal conduit formation Stoma Figure 2. Ileal conduit formation is the most commonly used method of urinary diversion in the UK, and involves anastomosing the ureters to an isolated piece of distal ileum, which is then mobilised and brought out as stoma on the abdomen (reproduced with permission from Macmillan Cancer Support) complications (Table 1), which are relatively frequent in the longer term (over 15 years’ follow-up) with ureteric obstruction reported in 14%, stoma problems in 24%, bowel problems in 24%, UTIs in 20% and metabolic derangement (severe metabolic acidosis) in 1%. Renal insufficiency developed in 27%, although in this elderly, comorbid population it is difficult to determine how much of this is attributable to the diversion.14 Metabolic complications are less common with an ileal conduit than a neobladder, as the conduit does not act as a storage reservoir for urine. The absorption of acid and chloride can result in the development of a hyperchloraemic metabolic acidosis. Although this can occur with an ileal conduit, it is more common in neobladders and can be managed with sodium bicarbonate, 1g once daily. The loss of the terminal ileum can result in the malabsorption of vitamin B12 and iron, which may cause macrocytic anaemia and neurological symptoms, although this is rare. The most common neobladder procedure performed in the UK is Studer pouch TRENDS IN UROLOGY & MEN’S HEALTH reconstruction (Figure 3). This involves using a section of small bowel between 45–60cm long, which is detubularised and reconstructed into a globular shape, forming a new reservoir that replaces the existing bladder. The ureters are implanted into this new reservoir, which is then anastomosed on to the urethra, utilising the patient’s pelvic floor sphincter mechanisms to provide a continent reservoir. For younger patients, neobladder formation is increasingly offered to patients at the time of RC. It has the advantage of not requiring a stoma and 90% of patients are continent by day and 70–80% by night. The disadvantages are that it requires a larger segment of small bowel than an ileal conduit (60cm in the Studer neobladder versus 15cm for an ileal conduit). As such, the rate of metabolic complications is proportionately higher. In more recent studies, intermittent self-catheterisation is required in a minority of patients (10%), with higher rates observed in women.15 For any radical cystectomy procedure, patients also need to be aware of the risks of impotence, incontinence or urinary retention, and female patients aware of the risk of vaginal shortening. Zippe et al found that fewer than 50% of female patients were able to have successful vaginal intercourse postoperatively and most female patients described reduced satisfaction with their sexual lives following surgery.16 In males, RC can be performed with nerve sparing techniques during the prostatic dissection to preserve sexual function. In females NOVEMBER/DECEMBER 2015 the procedure can be performed with preservation of the vagina. CHEMOTHERAPY RC achieves excellent local control; however, many patients will present with clinically advanced and likely micro-metastatic disease. As a result, there is a role for NAC prior to patients undergoing RC. There is an associated morbidity with NAC which can result in a delay before definitive surgical treatment can be performed, although accelerated chemotherapy regimes have been developed to shorten the time to definitive treatment. Kidney Ureter New bladder Urethra Figure 3. Neobladder formation involves using a section of small bowel reconstructed into a globular shape, forming a new reservoir that replaces the existing bladder. The ureters are implanted into this new reservoir, which is then anastomosed on to the urethra, utilising the patient’s pelvic floor sphincter mechanisms to provide a continent reservoir (reproduced with permission from Macmillan Cancer Support) www.trendsinmenshealth.com BLADDER CANCER 10 NAC (prior to RC) is predominantly used in patients with operable muscle-invasive tumours, with the purpose of treating micro-metastatic disease already present at the time of diagnosis. The administration of NAC may be preferable to postoperative treatment as tumour downstaging through chemotherapy may enhance resectability, metastatic disease may be treated as early as possible, and chemotherapy may be better tolerated than in the adjuvant setting. Adjuvant chemotherapy is used mostly to prevent recurrence in patients with either advanced disease or where there is regional lymph node involvement. Currently, the body of evidence supporting preoperative chemotherapy is much stronger than the evidence supporting postoperative chemotherapy.7 As such, preoperative cisplatin-based combination chemotherapy followed by RC represents a standard therapeutic option for patients with MIBC who are fit for chemotherapy. EXTERNAL-BEAM RADIATION THERAPY (EBRT) Radiotherapy involves the use of ionising radiation to cause fatal damage to neoplastic cells. A typical course of radical radiotherapy takes either 4 or 6.5 weeks. Radiation therapy as a single curative modality for MIBC has inferior local control rates compared to radical cystectomy, with 5-year survival between 30-60% depending on the stage.17,18 Radiotherapy outcomes can be improved with concurrent chemotherapy or with combined carbogen and nicotinamide administration.6 When combined with chemotherapy, although local relapse rates can be reduced, there is no benefit in terms of survival, mortality or quality of life. Smith et al identified no survival advantage following the addition of preoperative radiation therapy to RC when compared to RC alone in a prospective randomised trial.19 www.trendsinmenshealth.com Early Late Bladder Dysuria, frequency, urgency, radiation induced cystitis, incontinence Haematuria, reduced bladder volume Bowel Diarrhoea, cramps, radiation enteritis/ proctitis, incontinence Chronic enteritis General Fatigue, skin inflammation Subcutaneous fibrosis, sexual dysfunction Vaginal Irritation, bleeding, discharge, pain Shrinkage, adhesions Table 2. Early and late side-effects with external beam radiotherapy The best results with EBRT are seen in patients with solitary bladder lesions and without carcinoma in situ or evidence of upper tract obstruction. EBRT is associated with side-effects. Up to half of patients will complain of lower urinary tract symptoms, including dysuria and urinary frequency, during EBRT treatment. This tends to be resolved several weeks after treatment. In addition, 15% of patients report bowel side-effects secondary to EBRT. Radiotherapy can cause early side-effects that come on during the course, but can settle after 4 to 6 weeks, or late and often lasting adverse effects (Table 2). Although the 5-year survival rates are better with RC, this may be because patients with significant comorbidities are more likely to be given radical radiotherapy, whereas patients who are stronger and have better general health are put forward for surgery. A staging effect may be another possible factor, as staging is more accurate following surgery. Management following either RC or EBRT according to NICE guidance is given in Table 3. CONCLUSION Treatment for MIBC is associated with significant morbidity. Patients need to be counselled extensively prior to commencing treatment, and healthcare professionals need to be aware of the long-term sequelae. Following radical cystectomy Following radical radiotherapy Monitor upper tracts annually for hydronephrosis, stones, cancer Rigid cystoscopy 3 months after completion of radiotherapy Monitor eGFR annually Then cystoscopy every 3 months for first 2 years CT chest/abdomen/pelvis to assess for local and distant recurrence at 6, 12 and 24 months post-cystectomy Then cystoscopy every 6 months for the next 2 years Then annual cystoscopy thereafter Monitor annually for metabolic acidosis, vitamin B12 and folate deficiency Upper tract imaging annually for 5 years Male patients: urethral washings and annual urethroscopy for 5 years CT chest/abdomen/pelvis to assess for local and distant recurrence at 6, 12 and 24 months post radiotherapy Table 3. Follow-up after treatment for muscle-invasive bladder cancer according to NICE guidance6 TRENDS IN UROLOGY & MEN’S HEALTH NOVEMBER/DECEMBER 2015 BLADDER CANCER 11 Declaration of interests Jo Cresswell has received an honorarium from Prostrakan as an invited speaker and from Abbott as a member of an advisory panel. REFERENCES 1.Sobin D, Wittekind C, eds. TNM classification of malignant tumors. 6th edn. New York: Wiley-Liss, 2002;199–202. 2.Wu XR. Urothelial tumorigenesis: a tale of divergent pathways. Nat Rev Cancer 2005;5:713–25. 3.Dall’Era MA, Cheng L, Pan C-X. Contemporary management of muscle invasive bladder cancer. Expert Rev Anticancer Ther 2012;12:941–50. 4.Sylvester RJ, van der Meijden AP, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol 2006;49:466–77. 5.Fleshner NE, Herr HW, Stewart AK, et al. The National Cancer Data Base report on bladder carcinoma. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer 1996;78:1505. 6.NICE. Bladder cancer: diagnosis and management (NG2). February 2015 TRENDS IN UROLOGY & MEN’S HEALTH (www.nice.org.uk/guidance/ng2; accessed 30 September 2015). 7.Neoadjuvant chemotherapy for invasive bladder cancer. Cochrane Database Syst Rev 2005;2:CD005246. 8.Hounsome LS, Verne J, McGrath JS, Gillatt DA. Trends in operative caseload and mortality rates after radical cystectomy for bladder cancer in England for 1998–2010. Eur Urol 2015;67:1056–62. 9.Styn NR, Montgomery JS, Wood DP, et al. Matched comparison of robotic assisted and open radical cystectomy. Urology 2012;79:1303–8. 10.Bochner B, Sjoberg D, Laudone V. A randomized trial of robot-assisted laparoscopic radical cystectomy. N Eng J Med 2014;371:389–90. 11.Figueroa AJ, Stein JP, Dickinson M, et al. Radical cystectomy for elderly patients with bladder carcinoma: an updated experience with 404 patients. Cancer 1998;83:141–7. 12.Hautmann RE, de Petriconi RC, Pfeiffer C, Volkmer BG. Radical cystectomy for urothelial carcinoma of the bladder without neoadjuvant or adjuvant therapy: long-term results in 1100 patients. Eur Urol 2012;61;1039–47. 13.Cresswell J, Mariappan P, Thomas SA, et al. Radical cystectomy: analysis of trends in UK practice 2004–2012, in the British Association of Urological Surgeons’ (BAUS) NOVEMBER/DECEMBER 2015 Section of Oncology Dataset. J Clin Urology 2015. doi: 10.1177/2051415815595325 [Epub ahead of print]. 14.Lee RK, Abol-Enein H, Artibani W, et al. Urinary diversion after radical cystectomy for bladder cancer: options, patient selection, and outcomes. BJU Int 2014;113:11–23. 15.Meyer JP, Blick C, Arumainayagam N, et al. A three-centre experience of orthotopic neobladder reconstruction after radical cystectomy: revisiting the initial experience, and results in 104 patients. BJU Int 2009;103:680–3. 16.Zippe CD, Raina R, Shah AD, et al. Female sexual dysfunction after radical cystectomy: a new outcome measure. Urology 2004; 63:1153–7. 17.James ND, Hussain SA, Hall E, et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med 2012;366:1477–88. 18.Efstathiou JA, Zietman AL, Kaufman DS, et al. Bladder-sparing approaches to invasive disease. World J Urol 2006; 24:517–29. 19.Smith JA Jr, Crawford ED, Paradelo JC, et al. Treatment of advanced bladder cancer with combined preoperative irradiation and radical cystectomy versus radical cystectomy alone: a phase III intergroup study. J Urol 1997;157:805–8. www.trendsinmenshealth.com