Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
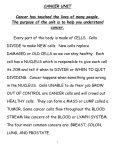
Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. REVISIONES Cytoreductive surgery and intraperitoneal chemotherapy for the treatment of peritoneal surface malignancy C. Pablo Carmignani, Jesús Esquivel and Paul H. Sugarbaker aDepartament of Surgical Oncology. Washington Cancer Institute. Despite new developments in the treatment of solid tumors, complete resection remains as an absolute requirement for cure of gastrointestinal cancer. Success in the surgical management of peritoneal surface malignancy depends on the surgeon’s ability to complete complex cytoreductive procedures so that only microscopic disease remains. This paper describes the current strategy that the surgical oncologist should pursue in the treatment of patients with peritoneal carcinomatosis, sarcomatosis and mesothelioma. Technical details required for this surgery include patient position, incision and exposure, complete lysis of adhesions, electroevaporative dissection, peritonectomy procedures, proper positioning of drains for intraperitoneal chemotherapy, and reconstructive surgery. Understanding the treatment and mastery of surgical skills to manage the peritoneal surface spread of malignancy has led to long-term survival of selected patients. The success of this treatment strategy depends on a long-term dedication to achieve the full potential of a curative outcome. Key words: peritoneal carcinomatosis, cytoreductive surgery, intraperitoneal chemotherapy. Carmignani CP, Esquivel J, Sugarbaker PH. Cytoreductive surgery and intraperitoneal chemotherapy for the treatment of peritoneal surface malignancy. Rev Oncol 2003;5(4):192-8.c INTRODUCTION Peritoneal seeding is one of the most frequent manifestations of treatment failure in patients with abdo- Correspondence: Dr. P.H. Sugarbaker Departament of Surgical Oncology Washinton Cancer Institute 110 Irving Street Suite CG-185 NW Washington, D.C. 20010 United States. E-mail: [email protected] Received 9 December 2002; Revised 12 March 2003; Accepted 21 March 2003. 192 Cirugía citorreductora y quimioterapia intraperitoneal para el tratamiento de la neoplasia en la superficie peritoneal A pesar de los nuevos descubrimientos en el tratamiento de los tumores sólidos, la resección completa continúa siendo un requisito absoluto para lograr la curación del cáncer gastrointestinal. El éxito del manejo quirúrgico de la neoplasia en la superficie peritoneal depende de la habilidad del cirujano para realizar complejas resecciones eliminando todo vestigio neoplásico visible. Este artículo describe la estrategia actual que el cirujano oncológico debería usar en el tratamiento de pacientes con carcinomatosis, sarcomatosis y mesotelioma peritoneales. Los aspectos técnicos del procedimiento quirúrgico consisten en posición del paciente, incisión y exposición, completa lisis de adherencias, disección electroevaporativa, peritonectomías, adecuado posicionamiento de drenajes para la quimioterapia intraperitoneal y cirugía reconstructiva. Como consecuencia de la comprensión del tratamiento y del perfeccionamiento de las habilidades quirúrgicas para manejar la siembra peritoneal del cáncer, la sobrevida ha aumentado en pacientes seleccionados. Es indispensable una prolongada dedicación tendiente a aprovechar todo el potencial de esta estrategia terapéutica. Palabras clave: carcinomatosis peritoneal, cirugía citorreductora, quimioterapia intraperitoneal. minopelvic malignancies. Despite curative surgery, between 20% and 30% of the patients will develop local tumor recurrence1,2. Regional dissemination with peritoneal implants has always been a therapeutic challenge with most patients undergoing palliative surgery or no surgery at all. Peritoneal carcinomatosis and sarcomatosis may occur either concomitantly with the primary tumor or as a recurrence after surgical resection. In the former, malignant cell dissemination is spontaneous, following serosal invasion or perforation of the involved organ. In the latter, it may be the consequence of in- Rev Oncol 2003;5(4):192-8 00 Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. CARMIGNANI CP, ESQUIVEL J, SUGARBAKER PH. CYTOREDUCTIVE SURGERY AND INTRAPERITONEAL CHEMOTHERAPY FOR THE TREATMENT OF PERITONEAL SURFACE MALIGNANCY vasive diagnostic or therapeutic procedures (i.e. fine needle aspiration, tumor rupture during an operation)3. Peritoneal seeding may occur even in the absence of hematogenous or lymphatic metastasis. A positive peritoneal fluid cytology has been detected in 25% to 30% of resectable gastric and colonic tumors4-7. Surgical resection results in the release of viable cancer cells in 50% to 60% of the patients8-10. The disruption of the peritoneal membrane provides a fertile area for peritoneal implants during inflammatory response period along with the healing process11. Combined use of peritonectomy and perioperative intraperitoneal chemotherapy is aimed to complete eradication of the disease. This new approach requires the acquisition of new technical skills to ensure safety and efficacy. STRATEGY FOR COMBINED TREATMENT Peritoneal surface malignancy requires a new therapeutic strategy that can be divided in four steps: electrosurgery for tumor resection and peritonectomy, hyperthermic intraperitoneal chemotherapy, reconstruction and early postoperative intraperitoneal chemotherapy. The use of adequate instruments and specific surgical techniques are essential to achieve optimum results. Electrosurgical dissection Surgical dissection is performed using 3 mm ball-tipped monopolar electrosurgery. The electrosurgical generator is set to pure cut, 200-250 MW.12 Tissues are evaporated at the contact of the ball tip, minimizing blood loss from vessels up to 1.5 mm in diameter. Larger vessels are electrocoagulated or ligated in continuity and divided. Intermittent saline irrigation is utilized to decrease the risk of heat damage to adjacent tissues. Heat necrosis at the tumor’s margin of resection could reduce the possibility of dissemination and cancer recurrence. Chemotherapy Agent’s selection for intraperitoneal chemotherapy is based on the ability of the drug to produce a cytotoxic effect over a short period of time and to show heat synergy. Mitomycin C, doxorubicin and cisplatin have a low clearance from the abdominal cavity13-15. Pharmacokinetic studies on intraoperative intraperitoneal chemotherapy showed 75% to 90% absorption of mitomycin C and cisplatin within the first hour16,17. Despite the enhanced cytotoxicity due to high concentrations and heat, this technique is effective only when treating small volume peritoneal carcinomatosis. Any anastomosis is constructed once intraoperative intraperitoneal chemotherapy is finished. In this way, 00 intestinal stumps are exposed to heat and to cytotoxic agent, preventing possible anastomotic recurrences. The first 5 days of the postoperative period, patients undergo a treatment with intraperitoneal chemotherapy through a Tenckhoff catheter using a different agent. Currently, the drugs on use are 5-fluorouracil or paclitaxel, depending on the primary tumor, its histologic characteristics, previous systemic or intraperitoneal chemotherapy and the response to these treatments. This stage of the treatment may be restricted in some patients, due to concomitant conditions or when the postoperative chemotherapy may increase importantly the morbidity of the procedure. Safety The occupational risk of the personnel exposed to long-term, low-dose cytotoxic agents used in the operating room remains unknown. Nevertheless, to date, research suggests no significant risk18. Guidelines for administration and manipulation of such agents are available19. The safety of all personnel in the operating room is paramount. The use of eye protection, double gloving with outer elbow-length gloves secured with sterile tape and impervious gowns are essential to protect the operator. Incorporation of a plastic cover within the sutures to the skin edge prevents droplet contamination. A smoke evacuation system removes steam from the chemotherapy in the abdominal cavity. INDICATIONS AND CONTRAINDICATIONS This therapeutic approach has been successfully employed in patients with peritoneal dissemination of primary peritoneal tumors, like peritoneal mesothelioma; in patients with tumors of the gastrointestinal tract like appendiceal, colonic and gastric cancer, and in selected cases of peritoneal sarcomatosis. This treatment is contraindicated in four well defined situations: when there is evidence indicating that the patient may not survive the procedure, when there are liver or extra-abdominal metastasis or when the computed tomography (CT) scan shows signs of segmental small bowel obstruction. If none of these stop signs is present and the surgeon finds during the operation that it would be impossible to re-establish intestinal function, he or she should perform the best possible surgical palliation. OPERATIVE PROCEDURE Patient position Careful positioning of the patient on the operating table is crucial to avoid complications related to areas of pressure, since this is a procedure that can last 10 to 12 hours. We advocate the lithotomy position, with Rev Oncol 2003;5(4):192-8 193 Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. CARMIGNANI CP, ESQUIVEL J, SUGARBAKER PH. CYTOREDUCTIVE SURGERY AND INTRAPERITONEAL CHEMOTHERAPY FOR THE TREATMENT OF PERITONEAL SURFACE MALIGNANCY open legs, thighs flexed 15° on the abdomen and legs flexed 30° on the thighs. The legs are supported by St. Mark’s leg holders (AMSCO, Erie, PA, USA) surrounded with alternating pressure devices (SBC Compression boots, Kendall Co., Boston, MA, USA) and protected from decubitus lesions by egg crate foam padding. The weight of the lower extremity is on the heel and not on the calf or popliteal crease. Exposure A vertical xiphopubic incision is made to allow maximum exposure; the xiphoid process is usually excised. During re-operation, old surgical scar is resected from the skin through the peritoneum, including umbilicus, to excise any implant in scar tissue20,21. A selfretaining retractor (Thompson Surgical Instruments, Inc., Traverse City, MI, USA) allows multiple angles of retraction to gain maximum exposure for peritonectomy (fig. 1). Peritonectomy All visible tumor should be excised in order to obtain maximum benefit from intraperitoneal chemotherapy. Peritonectomy techniques make possible to resect any disease involving parietal peritoneum. Small nodules can be electroevaporated but bigger nodules must be resected (fig. 2). Electroevaporative surgery Small implant adenocarcinoma Result Intraperitoneal chemotherapy Large implant adenoarcinoma Fig. 2. The small nodules (≤ 7 mm) usually do not invade beyond the muscular layer and allowing their electro-evaporation from the surface of the small bowel. Nodules bigger than the mentioned size invade the full thickness of the bowel wall. In such cases, electro-evaporation is too risky. Self-retaining retractor Lessea omentum Greater omentum Right and left upper quadrant peritonectomy Falciform and triangular ligaments are resected at the start of the operation. In right upper quadrant peritonectomy, peritoneum is stripped from the posterior rectus sheath in continuum. Dissection extends to the bear area of the liver. In case the tumor is advanced and has an invasive component, peritoneal stripping of the tendinous portion of the diaphragm may result in penetration into the pleural cavity. Tumor nodules sitting on the surface of the liver should be electroe- Fig. 1. Abdominal incision and self-retaining retractor position. Right hemidiafragm Centripetal surgery Peritoneal stripping begins in the medial line and proceeds in a circumferential fashion towards the deepest areas of the tumor and the major vessels. A coordinate effort includes up to 6 peritonectomy procedures. It is necessary to allow optimum clearance and containment of the tumor with minimal bleeding and no damage to vital structures. Rectal muscle should be preserved, but occasionally the posterior rectus sheath may be sacrificed. 194 Peritoneum involved Fig. 3. Peritonectomy of the right upper quadrant. Rev Oncol 2003;5(4):192-8 00 Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. CARMIGNANI CP, ESQUIVEL J, SUGARBAKER PH. CYTOREDUCTIVE SURGERY AND INTRAPERITONEAL CHEMOTHERAPY FOR THE TREATMENT OF PERITONEAL SURFACE MALIGNANCY vaporated, sometimes going beyond the Glisson’s capsule. In the left upper peritonectomy, the stripping away of the peritoneum will expose the left hemidiaphragm muscle and tendon, left adrenal gland, distal portion of the pancreas and the cephalic portion of the perirenal fat. Care is taken with the left gastric artery and coronary vein to protect the vascular supply of the stomach (fig. 3). Greater omentectomy and splenectomy The greater omentum is involved early in tumor dissemination within the abdominopelvic cavity and its removal is important to reduce risk of recurrence even if this structure appears normal. The greater omentum is resected to include the branches of the gastro-epiploic vessels on the greater curvature of the stomach and the short gastric vessels. All vessels are ligated and divided on the surface of the stomach. Early mobilization of the omentum improves exposure and enables an adequate visual assessment of the abdominal cavity, especially of the lesser sac. A splenectomy is performed to include the complete removal of tumor deposits on the anterior fascia of the pancreas and on the splenic hilus. Pelvic peritonectomy and rectosigmoidectomy It includes peritoneal stripping from the right and left caudal portions of the abdominal wall, the bladder and resection of rectosigmoid portion of large bowel along with their mesenteries from the origin of the inferior mesenteric artery. Stripping the peritoneum up to the duodenum and ligament of Treitz completes the peritonectomy and facilitates ligation of the inferior mesenteric artery and vein. In women a hysterectomy and bilateral salpingoophorectomy is performed. The subperitoneal rectum and apex of vagina in women are removed en-bloc including all the neoplastic tissues in the peritoneal cul-de-sac. Closure of the vagina is necessary before the intraoperative chemotherapy is initiated. Special care should be taken in order to avoid injuries to the ureters, bladder and pre-sacral and iliac vessels (fig. 4). Cholecystectomy, lesser omentectomy, and stripping the floor of the omental bursa Cholecystectomy is performed from the fundus; the structures of the porta hepatis are dissected free of tumor by a spreading clamp. Tumor from the anterior surface of the left caudate lobe process is electroevaporated and the gastrohepatic ligament is excised in resection of the lesser omentum. Care is taken with the left gastric artery and vein to protect the vascular supply of the stomach. After tumor resection, the abdominopelvic cavity is vigorously lavaged by many liters of warm saline solution aimed at mechanically eliminating viable cancer cells from fibrin and blood clots. The removal of fibrin and blood clots also helps reduce the risk of postoperative adhesions. OPEN HYPERTHERMIC INTRAPERITONEAL CHEMOTHERAPY Wide ligament (ligated) Douglas Pouch Ovaric vessels (sectioned) Ureter Inferior mesenteric artery (ligated) Fig. 4. The line shows the location of the incision for a comprehensive pelvic peritonectomy. 00 Hyperthermia optimizes the dose intensity of chemotherapy to the abdominal and pelvic surfaces. The combined use of hyperthermia and intraperitoneal chemotherapy has enhanced the cytotoxicity of the chemotherapeutic agents and increased tissue penetration by chemotherapy in cancerous as compared to normal tissue. Chemotherapy solution is administered with the abdomen open. To keep temperature to constant 42°C, the solution is pumped by two rolling pumps through a heat exchanger; then, through a Tenckhoff catheter reaches the peritoneal cavity. The hyperthermic perfusate comes-off the abdomen through four JacksonPratt drains going back to the heat exchanger, closing the circuit. The Tenckhoff catheter and the JacksonPratt drains are secured watertight with purse-string sutures on the skin of the abdomen to avoid leaks and spillage. Before starting the chemotherapy perfusion the system is tested and primed for leaks using one liter of 1.5% of dextrose peritoneal dialysis solution. Finally, three liters of chemotherapy solution are used Rev Oncol 2003;5(4):192-8 195 Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. CARMIGNANI CP, ESQUIVEL J, SUGARBAKER PH. CYTOREDUCTIVE SURGERY AND INTRAPERITONEAL CHEMOTHERAPY FOR THE TREATMENT OF PERITONEAL SURFACE MALIGNANCY to lavage the peritoneal cavity during 90 minutes at 42°C. RECONSTRUCTION OF THE ALIMENTARY TRACT AND CONSTRUCTION OF OSTOMIES Any anastomosis or ostomy is performed once the heated intraoperative intraperitoneal chemotherapy is finished. Patients that undergo a gastrectomy as part of the cytoreductive surgery, receive a duodenal exclusion operation to protect the esophagojejunostomy. The jejunum is transected 20 cm distal to the ligament of Treitz and its proximal portion is exteriorized to divert biliopancreatic fluid. The distal portion of the jejunum is anastomosed with the esophagus using a circular stapler (Ethicon ILS 29, Cincinatti, OH, USA). Before closure the Tenckhoff catheter is placed in the left upper quadrant close to the ligament of Treitz or in the right subdiaphragmatic space. Drains are placed in the pelvis cavity and subdiaphragmatic spaces. Chest tubes are inserted in pleural spaces when stripping of undersurface of diaphragm was performed. The abdomen is then closed in the usual fashion. Skin is sutured with a nylon running suture to decrease the likelihood of chemotherapy spillage during postoperative intraperitoneal chemotherapy. One last drain is positioned in the subcutaneous tissue. EARLY POSTOPERATIVE INTRAPERITONEAL CHEMOTHERAPY It is indicated following the complete resection of appendiceal, colorectal, gastric or other gastrointestinal carcinomas. Approximately 24 hours after cytoreductive surgery early postoperative intraperitoneal chemotherapy is initiated and the drains are closed for 23 hours. The abdomen is then drained for one hour until next chemotherapy infusion. This is repeated for 5 consecutive days. Table 1 summarizes the indications for perioperative intraperitoneal chemotherapy in the colorectal cancer setting. TABLE 1. Indications for perioperative intraperitoneal chemotherapy in colorectal cancer Positive peritoneal cytology Invasion or metastasis to the ovaries Seeding to the colonic serosa Rupture of a necrotic tumoral mass Invasion to adjacent organs Intraoperative peritoneal dissemination Primary tumor perforation Lymph node metastasis in the resection margin Limited peritoneal seeding with a peritoneal cancer index <20 Completeness of cytoreduction score 0-1 Advanced primary mucinous tumor Modified from Cancer Chemother Pharmacol23. 196 1 2 3 8 0 4 7 6 5 Regions 0 Central 1 Right superior 2 Epigastrium 3 Left superior 4 Left flank 5 Left inferior 6 Pelvis 7 Right superior 8 Right flank 9 Proximal yeyunum 10 Distal yeyunum 11 Proximal ileum 12 Distal ileum 11 9 10 12 Score of size of lesion LS0 No visible tumor LS1 Tumor until 0.5 cm LS2 Tumor until 5 cm LS3 Tumor bigger than 5 cm or tumoral confluency Fig. 5.Tumor volume as assessed by the lesion size score is determined for the 13 abdomino-pelvic regions. The sum of these scores (0-39) is the peritoneal cancer index. PERITONEAL CANCER INDEX The peritoneal cancer index is a quantitative prognostic score calculated after abdominal exploration and complete adhesiolysis. The success of complete cytoreduction and long-term survival can be predicted by grading the distribution and the mass of peritoneal surface cancer22. It is not useful, however, in grading minimally invasive tumors such as pseudomyxoma peritonei or cystic mesothelioma. In patients with peritoneal seeding from colon cancer, a score of 20 or less had a year survival of 50%, from 11-20 a survival of 20% and a score greater than 20, survival of 0% (fig. 5). CYTOREDUCTION SCORE Another quantitative prognostic score is the completeness of cytoreduction. For gastrointestinal cancer, the completeness of cytoreduction score has been defined as follows: CC-0, no visible peritoneal carcinomatosis remained after cytoreduction; CC-1, tumor nodules persist after cytoreduction but less than 0.25 cm; CC-2 tumor of 25 to 2.5 cm; CC-3 tumor greater than 2.5 cm or confluence of tumor unresectable at any site (fig. 6). Patients with complete cytoreduction have a higher chance of long-term survival, but incomplete cytore- Rev Oncol 2003;5(4):192-8 00 Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. CARMIGNANI CP, ESQUIVEL J, SUGARBAKER PH. CYTOREDUCTIVE SURGERY AND INTRAPERITONEAL CHEMOTHERAPY FOR THE TREATMENT OF PERITONEAL SURFACE MALIGNANCY DISCUSSION Citoreduction index (after resection) CC-0 CC-1 No evidence Evidence of disease of disease CC-2 0.25 cm 0.25 cm CC-3 2.5 cm >2.5 cm Fig. 6. Completeness of cytoreduction after surgery duction have a higher chance of long-term survival, but incomplete cytoreduction rarely offers cure. In patients with peritoneal seeding from colon cancer a complete cytoreduction had a 40% 5-year survival; patients with an incomplete cytoreduction had a 0% 5-year survival23. No patient with long-term survival has been reported undergoing surgery alone or surgery plus systemic chemotherapy. POSTOPERATIVE COMPLICATIONS Careful patient selection is crucial for the success of this treatment. The most common postoperative complications are prolonged intestinal ileus and gastric paresis. Nasogastric suction is maintained until there is evidence of bowel function. Total parenteral nutrition is needed until full caloric and proteic intake is achieved. About one fifth of the patients require parenteral feeding at home. In the most recent study of 200 patients who had undergone cytoreductive surgery and heated intraperitoneal chemotherapy for peritoneal carcinomatosis, 25% of the patients had complications grade III and IV. Mortality rate was less than 2% (3/200). Most frequent complications were peripancreatitis (7.1%) and bowel fistula (4.7%)24. Acute postoperative peripancreatitis, a potentially life-threatening condition, occurs more frequently if the peritoneum and fat are stripped from the surface of the pancreas. If the patient presents with fever, peripancreatitis should be ruled out. Along with the routine blood sample, a sample from the material in the left upper quadrant drain should be sent for lipase and amylase levels. SECOND-LOOK OPERATION A second-look with closure of a diverting jejunostomy or ileostomy is routinely performed at 6-9 months in one third of the patients. Eighty percent of the patients are found to have recurrences but have a complete redo-cytoreduction in 80% of the cases because of the low peritoneal cancer index. 00 The successful management of peritoneal surface malignancy depends on several factors: the presence of co-morbid conditions, the disease stage, tumor biology, the completeness of cancer excision and the elimination of minimal residual cancer by chemotherapy. The higher success rates associated with the treatment of cystadenocarcinoma, cystic mesothelioma and low-grade sarcomas are attributable to their expansive growth, with minimal invasion of the underlying structures. Poorer results were obtained with the treatment of adenocarcinoma, probably related to the invasive nature of these tumors. Incomplete peritonectomies result in early recurrence and treatment failure. The surgical procedure for the management of peritoneal malignancies poses a steep learning curve. It is technically and physically demanding with long operative time and a risk of excessive blood loss. Furthermore, the administration of early postoperative intraperitoneal chemotherapy may be compromised by the patient’s postoperative status. These factors may contribute to poor treatment outcome during the early stages of a program in treating peritoneal surface malignancy and may deter many surgeons25. However, the use of electroevaporative surgery has revolutionized the radical excision of peritoneal malignancies by minimizing blood loss. The pharmacokinetics advantages to intraperitoneal chemotherapy have been well described. The success of intraperitoneal chemotherapy is dependent on the elimination of residual cancer cells following complete resection. However, the benefit of intraperitoneal chemotherapy is localized to the surface area of infusion. Drug diffusion occurs but the tissue penetration is limited to 1-2 mm from the surface26-28. We believe that the open technique is superior to the closed technique in allowing adequate and uniform exposure of all abdominal and pelvic surfaces to intraperitoneal chemotherapy, as demonstrated by dye studies. In contrast, many areas are unstained with dye when the closed technique is employed, especially the lesser omentum, the base of the mesentery, the pelvis and the suture lines. As a result, recurrence of tumor often occurs on these sites of poor chemoperfusion20. SUMMARY Traditionally, peritoneal surface malignancy was regarded as a terminal condition for which surgery was indicated only as a palliative effort. Advances in cytoreductive surgery and perioperative intraperitoneal chemotherapy have improved the surgical approach for this condition23,25,29-32. Also, new evidence from tumor biology research suggests that peritoneal carcinomatosis, sarcomatosis and mesothelioma may oc- Rev Oncol 2003;5(4):192-8 197 Document downloaded from http://www.elsevier.es, day 12/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. CARMIGNANI CP, ESQUIVEL J, SUGARBAKER PH. CYTOREDUCTIVE SURGERY AND INTRAPERITONEAL CHEMOTHERAPY FOR THE TREATMENT OF PERITONEAL SURFACE MALIGNANCY cur without systemic dissemination, which has sparked new interest in these conditions. Curative treatment for peritoneal surface malignancies requires a complete cytoreduction followed by intraperitoneal chemotherapy. The careful selection of patients for a complete cytoreduction with curative intent vs. appropriate surgical palliation remains a crucial component of management to ensure that patients with unresectable disease receive an adequate palliation. This paper describes the current strategy for the management of patients with peritoneal carcinomatosis, sarcomatosis and mesothelioma. The relevant technical details specific to this form of treatment include patient position, incision and exposure, electroevaporative dissection, complete lysis of adhesions, peritonectomy procedures, reconstructive surgery and intraperitoneal chemotherapy. References 1. Abulafi AM, Williams NS. Local recurrence of colorectal cancer: the problem, mechanisms, management and adjuvant therapy. Br J Surg 1994;81:7-19. 2. Dahlberg M, Pahlman L, Bergstrom R, et al. Improved survival in patients with rectal cancer: a population-based register study. Br J Surg 1998;85:515-20. 3. Fortner JG. Inadvertent spread of cancer at surgery. J Surg Oncol 1993;53:191-6. 4. Koga S, Kaibara N, Iitsuka Y, et al. Prognostic significance of intraperitoneal free cancer cells in gastric cancer patients. J Cancer Res Clin Oncol 1984;108:236-8. 5. Baba H, Korenaga D, Haraguchi M, et al. Width of serosal invasion and prognosis in advanced human gastric cancer with special reference to the mode of tumor invasion. Cancer 1989;64:2482-6. 6. Haraguchi M, Watanabe A, Kakeji Y, et al. Prognostic significance of serosal invasion in carcinoma of the stomach. Surg Gynecol Obstet 1991;172:29-32. 7. Zeng Z, Cohen AM, Hajdu S, et al. Serosal cytologic study to determine free mesothelial penetration of intraperitoneal colon cancer. Cancer 1992;70:737-40. 8. Hansen E, Wolff N, Knuechel R, et al. Tumor cells in blood shed from the surgical field. Arch Surg 1995;130:38793. 9. Iitsuka Y, Kaneshima S, Tanida O, et al. Intraperitoneal free cancer cells and their viability in gastric cancer. Cancer 1979;44:1476-80. 10. Tanida O, Kaneshima S, Iitsuka Y, et al. Viability of intraperitoneal free cancer cells in patients with gastric cancer. Acta Cytol 1982;26:681-7. 11. Savalgi RS. Mechanism of Abdominal Wall Recurrence After Laparoscopic Resection of Colonic Cancers. Semin Laparosc Surg 1995;2:158-62. 12. Sugarbaker P. Laser-node electrosurgery. In: PH S, editor. Peritoneal carcinomatosis. Principles of management. Boston: Kluwer Academic Publishers, 1996; p. 375-85. 13. Howell SB, Pfeifle CL, Wung WE, et al. Intraperitoneal cisplatin with systemic thiosulfate protection. Ann Intern Med 1982; 97:845-51. 14. Hayashi T, Nasu Y, Aramaki K, et al. A case of peritoneal malignant mesothelioma with disappearance of ascites result of intraperitoneal instillation of mitomycin C and oral administration of UFT. Gan To Kagaku Ryoho 1989;16:2449-52. 198 15. Sugarbaker PH, Cunliffe WJ, Graves T, et al. Phase I and pharmacologic studies with early postoperative postoperative intraperitoneal epiadriamycin, Fourth International Conference on Advances in Regional Cancer Therapy. Berchtesgaden, Germany 1989. 16. Fernández-Trigo VS, Stephen OA, Hoover AD, et al. Surgically directed chemotherapy: Heated intraperitoneal lavage with mitomycin C. In: Sugarbaker P, editor. Peritoneal carcinomatosis. Drugs and disease. Boston: Kluwer, 1996; p. 55-61. 17. Stephens AD, Belliveau J, Sugarbaker PH. Intraoperative hyperthermic lavage with cisplatin for peritoneal carcinomatosis and sarcomatosis. In: Sugarbaker PH, editor. Peritoneal Carcinomatosis. Drugs and disease. Boston: Kluwer Academic Publishers, 1996; p. 15-30. 18. Stuart OA, Stephens AD, Welch L, et al. Safety monitoring of the coliseum technique for heated intraoperative intraperitoneal chemotherapy with mitomycin C. Ann Surg Oncol 2002;9:186-91. 19. White SK, Stephens AD, Sugarbaker PH. Hyperthermic intraoperative intraperitoneal chemotherapy safety considerations. Aorn J 1996;63:716-24. 20. Zoetmulder FA, Sugarbaker PH. Patterns of failure following treatment of pseudomyxoma peritonei of appendiceal origin. Eur J Cancer 1996;32A:1727-33. 21. Hughes ES, McDermott FT, Polglase AL, et al. Tumor recurrence in the abdominal wall scar tissue after largebowel cancer surgery. Dis Colon Rectum 1983;26:571-2. 22. Esquivel J, Farinetti A, Sugarbaker PH. Elective surgery in recurrent colon cancer with peritoneal seeding: when to and when not to proceed. G Chir 1999;20:81-6. 23. Sugarbaker PH. Successful management of microscopic residual disease in large bowel cancer. Cancer Chemother Pharmacol 1999;43(Suppl):15-25. 24. Stephens AD, Alderman R, Chang D, et al. Morbidity and mortality analysis of 200 treatments with cytoreductive surgery and hyperthermic intraoperative intraperitoneal chemotherapy using the coliseum technique. Ann Surg Oncol 1999;6:790-6. 25. Cavaliere F, Di Filippo F, Botti C, et al. Peritonectomy and hyperthermic antiblastic perfusion in the treatment of peritoneal carcinomatosis. Eur J Surg Oncol 2000; 26:486-91. 26. Markman M. Intraperitoneal chemotherapy for malignant diseases of the gastrointestinal tract. Surg Gynecol Obstet 1987;164:89-93. 27. Los G, Sminia P, Wondergem J, et al. Optimisation of intraperitoneal cisplatin therapy with regional hyperthermia in rats. Eur J Cancer 1991;27:472-7. 28. Los G, Verdegaal EM, Mutsaers PH, et al. Penetration of carboplatin and cisplatin into rat peritoneal tumor nodules after intraperitoneal chemotherapy. Cancer Chemother Pharmacol 1991;28:159-65. 29. Panteix G, Guillaumont M, Cherpin L, et al. Study of the pharmacokinetics of mitomycin C in humans during intraperitoneal chemohyperthermia with special mention of the concentration in local tissues. Oncology 1993; 50:366-70. 30. Yonemura Y, Fujimura T, Nishimura G, et al. Effects of intraoperative chemohyperthermia in patients with gastric cancer with peritoneal dissemination. Surgery 1996; 119:437-44. 31. Fujimoto S, Takahashi M, Mutou T, et al. Improved mortality rate of gastric carcinoma patients with peritoneal carcinomatosis treated with intraperitoneal hyperthermic chemoperfusion combined with surgery. Cancer 1997;79:884-91. 32. Sayag-Beaujard AC, Francois Y, Glehen O, et al. Intraperitoneal chemo-hyperthermia with mitomycin C for gastric cancer patients with peritoneal carcinomatosis. Anticancer Res 1999;19:1375-82. Rev Oncol 2003;5(4):192-8 00