Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
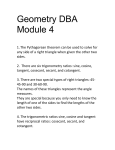
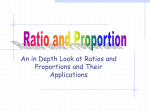
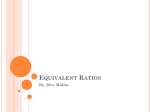
Volume 9 Number 6 Symposium 425 nographies, carried out at the time of maximal drug effect, showed no reduction in resistance. Fifty per cent of the patients studied showed a tachycardia with associated palpitations or weakness following prolonged use of the drug. It was concluded that isoproterenol produces a re- duction in intraocular pressure in man, unaccompanied by an improvement in facility of outflow. Direct measurements of aqueous production seem to be necessary to establish the pharmacologic effects of the beta stimulator isoproterenol on aqueous dynamics in man. Optic cup in normal and glaucomatous eyes M. F. Armaly Enlargement of the optic cup occurs early in the clinical course of open-angle glaucoma and results in inequality of this ratio in the 2 eyes. The enlargement, in general, parallels the magnitude of field defect. It is suggested that involvement of the visual field in eyes with ocular hypertension is related to the cup disc ratio (C/D), being more frequent in eyes with genetically large cups T, he ratio of the horizontal diameter of the optic cup to that of the optic disc (C/D), estimated to the nearest tenth by ophthalmoscopic examination, was shown to exhibit marked individual variation which was independent of age and sex. It was found to be genetically determined and separately related to two genetically determined measures, applanation pressure (PA) and tonographic estimate of aqueous outflow facility (C). This relationship exhibited significant interaction, such that the highest frequency of large ratios, i.e., C/D > 0.3, occurred in eyes with high PA readings and low C values, whereas in eyes with large C values this frequency did not vary with PA-1"3 In eyes with established glaucomatous From the Department of Ophthalmology, University Hospitals, Iowa City, Iowa. This investigation was supported in part by research grant CD-00017 from the National Center for Health Services Research and Development Health Services and Mental Health, and NB-07328 from the National Institute of Neurological Diseases and Blindness, United States Public Health Service, Bethesda, Md. field defect, marked variation in this ratio was encountered, such that it could not be used to predict the presence of field defect.4 These studies emphasized the difference between an acquired enlargement of the optic cup in glaucoma and the genetically large cup in the normal eye and indicated that a significant clue in this regard is that in the normal, the ratio is equal in the 2 eyes, and a difference > 0.2 occurs in less than 1 per cent of the normal samples. This report will be concerned with the C/D ratio in individuals, free of ocular complaints, who were discovered to have glaucomatous field defect as they participated in studies involving the normal population. Such individuals constitute the earliest clinical stage of glaucoma. Findings in these subject indicate that enlargement of the optic cup is already evident at this stage of involvement and can be suspected by comparison of the 2 eyes. Ophthalmoscopic examination is important in this regard. Involvement of the visual field in eyes with high applanation pressure may be significantly related to the genetically determined size of the optic Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933613/ on 05/12/2017 426 Armaly Investigative Ophthalmology June 1970 cup and occurs more frequently in eyes with large C/D ratios. The sample The sample consisted of 83 subjects who had been discovered, through their participation in population studies, to have a PA level of 20 mm. Hg or higher, a 50 Affected eye 40 § glaucomatous defect of the visual field, and open angles on gonioscopy. They had experienced no significant ocular symptoms and had, to the best of their knowledge, normal eyes. Field defects that were considered glaucomatous were demonstrated with the stimulus of 1-2-e or larger on the Goldmann perimeter and consisted •Normal control 30 20 10 0.0-0.1 0.2-0.3 0.4-0.5 0.6-0.7 CUP/DISC, Ratio 0.8-0.9 Fig. 1. The C/D ratio in the affected eye of patients with unilateral field defect. C/D ratio of the affected eye is represented in stippled bars and that of the normal control in light gray bars. 50 Unaffected eye 40 rNormal control 30 20 10 0 0.0-0.1 -mm 0.2-0.3 0.4-0.5 0.6-0.7 CUP/DISC Ratio 0.8-0.9 Fig. 2. C/D ratios in the unaffected eye of patients with unilateral field defect. C/D ratio of the unaffected eye is represented by stippled bars and that of the normal control in light gray bars. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933613/ on 05/12/2017 Volume 9 Number 6 Symposium 427 of the following: (1) arcuate scotoma continuous with the blind spot and greater than 45 degrees, (2) paracentral scotoma larger than 5 degrees in diameter, and (3) nasal step greater than 10 degrees. In 52 subjects the defects existed in one eye only, the other having normal visual field. Both eyes were affected in 31 subjects. Results In order to compare the C/D ratio in this sample with an appropriate control, the frequency distribution of C/D ratio in individuals with normal visual fields in both eyes and a pressure of 20 mm. Hg or higher was used as a reference or control. In this group, the frequency of C/D > 0.3 was greater (27 per cent) than that in normal eyes with PA less than 20 mm. Hg (15.5 per cent). The results of the first group of unilateral involvement appear in Figs. 1 and 2. The distribution of C/D ratios in the affected eye differs markedly from that of the control. In the affected eye, the frequency increases with larger cup/disc ratios, being greatest for C/D of 0.8 to 0.9, whereas in the control, the frequency is highest for C/D values between 0.0 and 0.3 and decreases markedly and progressively for larger C/D values so that the least frequent is 0.8 to 0.9. In the unaffected eye, the frequency distribution of C/D ratio is also different from the control group. Frequency of C/D of 0.0 to 0.1 is very small compared to the control, whereas that of values greater than 0.3 is comparatively greater. These differences in frequency are statistically significant at the 1 per cent level of confidence. If we now compare in each individual the C/D ratio in the affected eye with that of the uninvolved eye, we see evidence that the C/D ratio in the affected eye has already become enlarged. Instead of values falling on the line indicating equality of the 2 ratios or being distributed randomly above and below it, a systematic effect is evident (Fig. 3): The C/D ratio of the affected eye is larger than that of the unaffected eye. The results of the second group with bilateral involvement appear in Figs. 4 and 5. They demonstrate the greater frequency of large C/D ratios in these eyes and the greater enlargement of the cup in eyes with a greater field defect. Comments 0.9 • * / 0.7 i 6 «i w • 0.5 0.3 0.1 0 0.1 0.3 0.5 0.7 0.9 Fig. 3. C/D ratios in subjects with unilateral glaucomatous field defect. C/D ratio in the eye with normal field appears on the abscissa and that in the eye with field defect on the ordinate. The line representing equality of the 2 ratios is drawn. Each subject is represented by one point at the intersection of the 2 coordinates of the C/D ratios in his 2 eyes. These findings clearly point out that enlargement of the optic cup in open-angle glaucoma is not limited to the later stages of the clinical disease but can be detected in the earlier stages, long before the individual becomes aware of this condition. As such, it becomes an important useful tool in the suspicion and detection of this otherwise symptomless disease. In individuals with monocular involvement of the visual field, the C/D ratio was larger in the affected eye in 36 subjects. Thus, with careful ophthalmoscopic examination, one could have suspected glaucoma on the basis of this inequality in 69 per cent and successfully identified the involved eye in 63 per cent of this group. Considering the simplicity of this procedure and the high frequency of false posi- Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933613/ on 05/12/2017 Investigative Ophthalmology June 1970 428 Armaly 50 r 40 -Normal control ^ I 30 mm mm 20 10 0L 0.0-0.1 0.2-0.3 0.4-0.5 0.6-0/? CUP/DISC Ratio 0.8-0.9 Fig. 4. C/D ratio in patients with bilateral field defects. C/D ratio of affected eyes is represented in stippled bars and that of the normal control in light gray bars. 0.9 r 0 0.1 Fig. 5. C/D ratios in subjects with bilateral glaucomatous field defects. C/D ratio in the eye with the lesser defect appears on the abscissa and that in the eye with the greater defect on the ordinate. The line indicating equality of the 2 ratios is drawn. Each subject is represented by one point at the intersection of the 2 coordinates of C/D ratios of his 2 eyes. tive suspicion by tonometry alone, the clinical usefulness of ophthalmoscopy in early detection of glaucoma becomes obvious. This is further emphasized by the innocuous nature of this examination and the feasibility of including ophthalmoscopy as a part of the general medical examination of the practicing physician. This inequality was present also in bilaterally involved eyes. Here, however, the process of enlargement of the cup has affected both eyes and the difference between them has been masked by this process so that inequality occurred in 52 per cent. In the two groups combined, inequality was present in 63 per cent of subjects. If we consider the C/D ratio in the uninvolved eye in individuals with unilateral field defects to represent the genetically determined ratio for that individual, and compare its distribution with that in ocular hypertensive subjects with normal visual fields in both eyes, we are led to conclude that affected individuals were not randomly selected from among the ocular hypertensive group to represent all C/D ratios. Instead, those with large C/D ratios were selected with a significantly greater frequency. Thus, from among ocular hypertensive subjects, those with large C/D ratios developed a glaucomatous field defect with a significantly greater frequency than those with small C/D ratios. Long-term follow-up of individuals with ocular hypertension and varying values of C/D ratio, who have normal visual fields, is currently in progress in order to evaluate this conclusion. Those who have a large C/D ratio are expected to develop field defects in the future more Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933613/ on 05/12/2017 Symposium 429 Volume 9 Number 6 frequently than those with small C/D ratios. The results in bilaterally affected individuals suggest that they fall into two clusters: one with small C/D ratios and another with large C/D ratios. This could reflect a distortion in the distribution of C/D ratio due to the acquired enlargement; on the other hand, it could indicate that different sets of factors are involved in the production of the field defect in these two groups. Systemic factors, vascular, metabolic, or endocrine, have been shown to influence the vulnerability of the visual field to the ocular pressure level. These may play different roles in the two clusters. REFERENCES 1. Armaly, M. F.: Genetic determination of cup/disc ratio of the optic nerve, Arch. Ophthal. 78: 35, 1967. 2. Armaly, M. F., and Sayegh, R. E.: The cup/disc ratio—the findings of tonometry and tonography in the normal eye, Arch. Ophthal. 82: 191, 1969. 3. Armaly, M. F.: The optic cup in the normal eye. I. Cup width, depth, vessel displacement, ocular tension and outflow facility, Amer. J. Ophthal. 68: 401, 1969. 4. Armaly, M. F.: The correlation between appearance of the optic cup and visual function, Trans. Amer. Acad. Ophthal. Otolaryng. 78: 898, 1969. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933613/ on 05/12/2017