Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
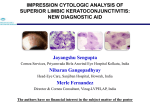
The AOA’s CLCS Newsletter, May 2013 Superior Limbic Keratoconjunctivitis Melissa Barnett, O.D. Characteristics There are three distinctive features of Superior Limbic Keratoconjunctivitis (SLK), also known as SLK of Theodore. The first is superior bulbar conjunctival inflammation. This area may have sectoral injection with thickening of tissue. The second sign is an adjacent corneal epithelial keratitis. The third characteristic is papillary hypertrophy of the superior palpebral conjunctiva. Symptoms of SLK include ocular discomfort, burning, foreign-body sensation, non-specific pain, a red eye, photophobia and excessive tearing. Visual acuity is typically not affected. The course of SLK may be chronic with exacerbations and remissions.4 Work up A systemic thyroid workup should be performed in all patients with SLK. Thyroid disease has been reported in 50-65% of patients with SLK. Rheumatoid arthritis and Sjögren’s syndrome may also have similar associations with SLK therefore additional testing may be indicated. In 2011, a study by Sun et al. determined that there is an over expression of MMP-1 and -3 in surgical specimens and cultured conjunctival fibroblasts from SLK patients.8 Treatment SLK is a chronic, recurrent and sometimes unruly condition. There are many different treatment modalities that may be utilized with success. For mild cases, treatment includes aggressive lubrication with non-preserved artificial tears and lubricant ointment. Punctal occlusion may also be used as well as treating any coexistent blepharitis. Eye drops such a cyclosporine A, autologous serum, vitamin A and 4% cromolyn sodium solution have been somewhat effective in managing SLK.1,5,7 If symptoms are more severe, 0.5 to 1.0% silver nitrate solution may be applied topically for 1020 seconds to the superior bulbar and tarsal conjunctivae after a local anesthetic is applied. The eye is then irrigated with saline and antibiotic ointment is used nightly for 1 week. The goal of this treatment is to chemically cauterize the irregular tissue in order to promote regrowth of new healthier epithelium. Other treatment options include pressure patching, bandage contact lenses or thermal cauterization. Surgical recession or resection of the superior bulbar conjunctiva with or without amniotic membrane has also been employed as treatment modalities for SLK.3,6 A report in 2009 by Chun demonstrated that a large diameter contact lens and Botulium toxin A may also be considered for treatment of SLK for a short duration.2 References 1. Confino J, Brown SI. Treatment of superior limbic keratoconjunctivitis with topical cromolyn sodium. Ann Ophthalmol. Apr 1987;19(4):129-31. 2. Chun YS, Kim JC. Treatment of superior limbic keratoconjunctivitis with a large-diameter contact lens and Botulium Toxin. Cornea. 2009 Aug;28(7):752-8. 3. Donshik PC, Collin HB, Foster CS, et al. Conjunctival resection treatment and ultrastructural histopathology of superior limbic keratoconjunctivitis. Am J Ophthalmol. Jan 1978;85(1):101-10. 4. Gerstenblith A, Rabinowitz M. Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. March 2012. 5. Goto E, Shimmura S, Shimazaki J, et al. Treatment of superior limbic keratoconjunctivitis by application of autologous serum. Cornea. Nov 2001;20(8):807-10. The AOA’s CLCS Newsletter, May 2013 6. 7. 8. Kheirkhah A, Casas V, Esquenazi S, et al. New surgical approach for superior conjunctivochalasis. Cornea. Jul 2007;26(6):685-91. Sahin A, Bozkurt B, Irkec M. Topical cyclosporine a in the treatment of superior limbic keratoconjunctivitis: a long-term follow-up. Cornea. Feb 2008;27(2):193-5. Sun YC, Hsiao CH, Chen WL, et al. Overexpression of matrix metalloproteinase-1 (MMP-1) and MMP-3 in superior limbic keratoconjunctivitis. Invest Ophthalmol Vis Sci. 2011 Jun 1;52(6):3701-5. Dr. Melissa Barnett is a principal optometrist at the UC Davis Medical Center in Sacramento, where she performs primary and medical eye examinations and fits contact lenses including specialty contact lenses in addition to teaching optics and contact lenses to ophthalmology residents. She lectures and has been published on topics including dry eye, anterior segment disease, contact lenses, corneal collagen cross-linking and creating a healthy balance between work and home life for women in optometry. She is also a spokesperson for the California Optometric Association and has appeared on several television shows. Please close this browser window to return to the CLCS Newsletter