Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
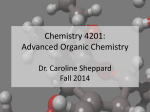
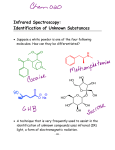
Ultraviolet/Visible Light Absorption Spectrophotometry in Clinical Chemistry Stephen L. Upstone in Encyclopedia of Analytical Chemistry R.A. Meyers (Ed.) pp. 1699–1714 John Wiley & Sons Ltd, Chichester, 2000 UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY 1 Ultraviolet/Visible Light Absorption Spectrophotometry in Clinical Chemistry Acknowledgments 13 Abbreviations and Acronyms 13 Related Articles 14 References 14 Stephen L. Upstone PerkinElmer Ltd., Beaconsfield, UK Ultraviolet/visible (UV/VIS) absorption spectroscopy has been used in the clinical laboratory for many years. The technique has appeal, as it is almost universal in its application. Although much of the routine work is performed using high-throughput dedicated clinical analysis systems, absorption spectroscopy still has a place in most clinical laboratories. This article discusses the range of application types for which absorption spectroscopy can be used and some examples of common analyses are given. The article also discusses the merits of various instrument types and discusses some more advanced spectroscopic techniques, such as derivative spectroscopy, to enhance the data measured by the spectrophotometer. Brief reference is also made to the use of reflectance in clinical analysis. 1 Introduction 2 Principles of Analysis and Instrument Parameters 2.1 Fundamentals of Ultraviolet/Visible Spectroscopy and the Beer – Lambert Law 2.2 Linearity and Deviations from the Beer – Lambert Law 2.3 Cuvettes and Solvents 2.4 Resolution (Band-pass) and Slit Width 2.5 First- and Second-derivative Spectroscopy 2.6 Verification of Spectrophotometer Performance 3 Overview of Instrument Designs and Their Advantages and Disadvantages 3.1 Dispersive and Diode-array Systems 3.2 Dispersive Ultraviolet/Visible Spectrophotometers 3.3 Single-beam Spectrophotometers 3.4 Double-beam Spectrophotometers 3.5 Dual-beam Spectrophotometers 3.6 Photodiode-array Spectrophotometers 3.7 Microplate Reader Spectrophotometers 3.8 Reflectance-based Analyzers 4 Common Clinical Applications Using Ultraviolet/Visible Absorption Spectroscopy 4.1 Enzyme Rate Assays 4.2 Colorimetric and End-point Assays 4.3 Immunoassays, Enzyme-linked Immunosorbent Assays and Microplate Assays 4.4 Porphyrin Analysis 4.5 Hemoglobin Analysis 4.6 Protein Assays 4.7 Molecular Biology 1 2 2 2 3 4 5 1 INTRODUCTION 5 Ultraviolet/visible (UV/VIS) absorption spectroscopy has been used in the clinical laboratory for many years. The technique has appeal, as it is almost universal in its application. The reliance on UV/VIS spectrophotometers (and other spectroscopic techniques) has diminished over the years, however, as dedicated multichannel clinical analyzers and readers have appeared on the market. These analyzers offer high sample throughput and clinically validated proprietary chemistries with ready-mixed reagents for greater speed and convenience. These analyzers normally utilize a range of analytical techniques such as ion-selective electrodes, turbidometry and UV/VIS absorption in one integrated instrument. Reagent manufacturers are also trying to simplify the analysis even further so that much simpler instrumentation is required. There is some work on solid-phase chemistry systems in which the completed reaction on the solid surface can be measured on a simple reader which uses a simple light-emitting diode (LED) source and measures light reflectance from the active face. Spectroscopic analysis, in general, is in a slow decline in the clinical laboratory as the increasing adoption of molecular biological techniques such as the polymerase chain reaction (PCR) and DNA sequencing are now being used to measure (for example) genetic abnormalities rather than the more indirect biochemistry-based approach. 6 6 6 6 6 8 8 8 9 9 9 10 11 11 12 12 13 Encyclopedia of Analytical Chemistry R.A. Meyers (Ed.) Copyright John Wiley & Sons Ltd 2 CLINICAL CHEMISTRY I have spent some length explaining the fundamentals of the technique and about instrument design. This is deliberate – too often people treat UV/VIS spectrophotometers as a simple ‘‘meter’’ without understanding their limitations or suitability for a particular analysis. This article should also be useful for understanding spectrophotometric assays on dedicated analyzers. 2 PRINCIPLES OF ANALYSIS AND INSTRUMENT PARAMETERS 2.1 Fundamentals of Ultraviolet/Visible Spectroscopy and the Beer – Lambert Law UV/VIS spectroscopy is the study of how a sample responds to light. When a beam of light passes through a substance or a solution, some of the light may be absorbed and the remainder transmitted through the sample. The ratio of the intensity of the light entering the sample (I0 ) to that exiting the sample (It ) at a particular wavelength is defined as the transmittance (T). This is often expressed as the percentage transmittance (%T), which is the transmittance multiplied by 100 (Equation 1): I0 %T D ð 100 .1/ It The absorbance (A) of a sample is the negative logarithm of the transmittance (Equation 2): AD log T .2/ The UV/VIS range of the electromagnetic spectrum covers the range 190 – 700 nm (most instruments are capable of measuring at longer wavelengths than this, depending on their detector type). For clinical analysis this is useful, as water (most assays are in aqueous solution) is almost completely transparent in this region. Most clinical assays are concerned with quantitation rather than identification (there are more powerful techniques available to perform the latter) as absorption spectra tend to be featureless – they lack the fine structure which is found, for example, in an infrared (IR) spectrum. Some techniques to enhance resolution and qualitative information will be discussed later. The most important principle in absorption analysis is the Beer – Lambert law. This law states that, for a given ideal solution, there is a linear relationship between concentration and absorbance provided that the path length is kept constant; the absorptivity (e) is a constant for each molecule for each wavelength (Equation 3): A D ecl .3/ where e D the absorptivity of the substance, c D concentration and l D path length. Provided that e and l are kept constant for a given set of experiments, a plot of the sample absorbance against the concentration of the absorbing substance should give a straight line. In practice, a calibration curve is prepared by plotting the absorbance of a series of standard samples as a function of their concentration. If the absorbance of an unknown sample is then measured, the concentration of the absorbing component can be assessed from this graph. Another consequence of the Beer – Lambert law is that it is possible to change the path length to affect the absorbance. This can be useful where lower detection limits are required as the path length can be increased (longer path length cuvettes are available) or, where the absorbance is too high to be measured on the instrument, the path length can be reduced. Alternatively, it is possible to reduce the absorbance by diluting the sample, but one has to take care when dealing with biologically active samples, particularly enzyme-based solutions, as this may have a profound effect on the activity. 2.2 Linearity and Deviations from the Beer – Lambert Law Above, the Beer – Lambert Law has been shown to be a linear relationship between sample concentration and absorbance. If this relationship is tested experimentally by measuring samples of increasing concentration and the results are plotted, the relationship will be seen to break down with increasing absorbance. With general laboratory UV/VIS spectrophotometers of recent design, this will probably be around 3 absorbance units (AU). What is observed here is not a breakdown in the Beer – Lambert law (although some assumptions about the sample being infinitely dilute are made in the law) but a limitation in the instrument’s performance. The greatest contributor to this nonlinearity is the instrument’s stray light. Stray light can be loosely defined as the amount of light present in the instrument at nonanalytical wavelengths or, put another way, the amount of unwanted light present in the system. This unwanted light can come from several sources. First, there may be light from outside entering the optical system. Manufacturers usually go to some lengths to exclude this light and so it ought to be negligible in a well-designed instrument. The main source of stray light comes from the monochromator itself. Monochromators (in dispersive instruments) are usually diffraction gratings. These gratings, although highly efficient producers of monochromatic radiation, are not entirely efficient. They will also allow small amounts of light to pass through at other discrete wavelengths, in addition to small amounts of white light. We have seen UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY Table 1 Observed absorbance readings for three different instrument stray light specifications True absorbance 1.0 2.0 3.0 4.0 5.0 a b c 1% T stray lighta 0.01% T stray lightb 0.0001% T stray lightc 0.9788 1.8239 2.2218 2.2924 2.3009 0.9996 1.9957 2.9586 3.6999 3.9586 1.0000 2.0000 3.0000 3.9957 4.9586 Low-cost or old instrument. High-performance double-beam instrument. ‘‘Top of the range’’ double-monochromator, double-beam instrument. earlier that absorbance is a logarithmic scale and so 1 AU corresponds to 10% T, 2 AU corresponds to 1% T, 3 AU to 0.1% T and so on. If the light throughput is expressed in percentage terms (%T) and a stray light value (from the instrument manufacturer’s data) of 0.05% transmittance is quoted, this will represent a third of the total light seen by the detector at 3 AU (i.e. 0.1% T). This will cause an underreporting of the true absorbance. By 4 AU (0.01% T), there will be more stray light than sample signal, rendering the instrument unusable at this value. Table 1 shows the anticipated effect on the observed absorbance for a range of stray light values which may be encountered on various instruments found within the clinical laboratory. 2.2.1 Other Causes of Non-linearity Occasionally, there are other reasons why there may be unexpected deviations from linearity. One major cause is sample fluorescence. If a fluorophore is excited at the same wavelength at which one is trying to measure absorption (the chromaphore), the detector will see a combination of absorbed light and the fluorescence emission. This emission will occur at a longer wavelength than the absorption. It should be borne in mind that there is no monochromator (on a dispersive instrument) between the sample and detector, so the emission will be detected. The observed result will be a lower absorbance reading than expected (as the detector is receiving light from two phenomena instead of one). If sample fluorescence is severe, it can be removed by inserting a cutoff filter between the sample and the detector. This filter should allow light of the absorbance wavelength to pass through but block higher wavelengths. Sometimes the linearity can be affected by changes in pH. Some chromophores (the functional group in the molecule responsible for the light absorption) will shift wavelength with a change in pH. If the absorption peak is particularly sharp, it may mean that measurement 3 is no longer at the actual peak but at its side. More sophisticated instruments can detect the actual peak for every measurement or measure areas under the absorption curve between two user-defined points. Another possible reason for nonlinearity is sample scatter. The instrument expects light to travel through the sample in a straight line (unless there is special provision in the instrument design). If the sample is turbid, this light will be scattered and the light will be splayed out in a cone-like fashion. As a result, less light will fall on the detector and a falsely high absorbance reading will be observed. Turbidity is relatively easy to observe as it is not wavelength specific. A scattering sample, therefore, will have a raised baseline. In bad cases, the baseline may be elevated over 1 AU. 2.3 Cuvettes and Solvents Apart from ensuring that the instrument design is sufficient for the required analysis, the user must also check that the other components of the analytical system – the cuvettes and the solvents – are applicable for the required task. Cuvettes are offered in either optical glass or quartz. Optical glass will transmit light above 320 nm whereas quartz will transmit light well below 190 nm (the usual low-wavelength limit for UV/VIS spectrophotometers). As an alternative to glass and quartz cuvettes, several manufacturers offer disposable cuvettes. These are made from various plastics including polystyrene and acrylic. These cuvettes offer the main advantage that they do not need cleaning between samples, which is very useful when handling biohazardous samples. The disadvantages are that they have a restricted wavelength range (one should carefully check the manufacturer’s stated wavelength specification before using disposable cuvettes) and they have a lower optical performance. In some cases striations across the face of the cuvette might be observed. These are due to the molding process in the cell manufacture. There will also be a molding mark at the bottom of the cuvette (from the extrusion process) and this can make stirring with a small magnetic flea difficult (with instruments which provide a stirring facility). Another disadvantage with disposable cuvettes is that the cell path length (an important consideration for the Beer – Lambert law) will not be as accurate as with glass or quartz cells and this may have quantitative accuracy implications. Figure 1 shows the light transmission charateristics of some common cuvette materials. As regards solvents, water has the widest range and the lowest cutoff wavelength. Cutoff wavelengths are somewhat arbitrary and there will be variations in the stated values from different literature sources. I have used the definition as being the wavelength 4 CLINICAL CHEMISTRY 100 60 40 Quartz Plastic (acrylic) Glass 20 0 190 300 400 500 600 700 Wavelength (nm) Figure 1 Light transmission characteristics of various cuvette materials. Table 2 Cutoffs for common solvents Solvent Cutoff (transmittance of 10% in a 1-cm cell) (nm) Water 2-Propanol (isopropyl alcohol) Ethanol Methanol Acetonitrile Dichloromethane Toluene Acetone Chloroform 190 210 210 210 210 235 270 330 250 Absorbance %T 80 possess a broad spectrum, so a small band-pass will not change the appearance of the spectrum (apart from increased noise). Some molecules commonly encountered in clinical analysis, such as porphyrins and the various types of hemoglobin (oxy-, met- and carboxy-) give sharp structures and the position of the peak has to be accurately measured or a misdiagnosis may otherwise result. Figure 2 shows the effect on a sample with fine structure, i.e. benzene vapor in a sealed cuvette. This is a highly artificial situation, as typical samples in the clinical laboratory do not exhibit such sharp features. Figure 3 shows the effect of variable resolution on a more typical sample with a single broad peak. In this instance there is little or no difference between a highand low-resolution (band-pass) scan. (a) (b) 230 at which a 1-cm cuvette filled with pure solvent has a transmittance of 10% (equivalent to 1 AU). The cutoffs for common solvents are given in Table 2. Some buffers [e.g. tris(hydroxymethyl)aminomethane (TRIS)] have organic components and so it should not be assumed that the cutoff is identical with that for water. 235 240 245 250 255 260 265 270 Wavelength (nm) Figure 2 Effect of changing the instrument resolution on a sample with sharp peaks (benzene vapor) showing the effect on band shapes and illustrating sharper discrimination using a 0.5-nm slit (b) compared with a 2-nm slit (a). 1.8 1.6 UV/VIS instruments have a specified band-pass. This term relates to the instrument’s ability to resolve peaks which are very close together or ‘‘shoulders’’ (small features on the side of a larger peak). The band-pass will either be fixed, usually between 1 and 2 nm, or, in the case of more expensive instruments, variable (either continuously or in finite steps). Photodiode-array instruments have a fixed optical band-pass as there is no physical slit aperture on these instruments (although the software may be able to simulate other slit conditions); the resolution is defined by the light dispersion, the polychromator and the number of elements in the array. The band-pass will affect the instrument’s ability to discriminate between sharp features. Most molecules 1.4 Absorbance 2.4 Resolution (Band-pass) and Slit Width 4 nm 1.2 1.0 0.5 nm 0.8 0.6 0.4 0.2 500 550 600 650 700 750 Wavelength (nm) Figure 3 Effect of using various slit settings on a typical spectrum with broad bands (spectra offset for clarity) showing that the slit setting is largely irrelevant for broad peaks. 5 UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY 2.5 First- and Second-derivative Spectroscopy UV/VIS spectra are rather featureless at room temperature, which is why the technique is primarily used for quantitative analysis rather than for sample identification purposes. A broad ultraviolet (UV) spectrum is composed of many separate electronic transitions which, at room temperature, become ‘‘blurred’’ to give the appearance of a single entity. Spectra only become more defined at very low temperatures and in the gas phase. Neither of these two conditions is applicable in routine clinical analysis. One major advantage that UV/VIS analysis possesses for biological measurements is that water (which is the main component of all living systems) is virtually transparent across the entire range (there is some very weak activity around 860 nm) and so any technique to improve the qualitative data is welcome. Derivative spectroscopy is a useful tool to give some improvement. As the name suggests, the technique consists of plotting the rate of change of the absorbance spectrum versus wavelength. This will give a plot (shown in Figure 4 with the original spectrum). At peak maxima and minima (and also points of inflection), the graph is seen to pass through zero on the ordinate. As a result, the technique can be used to identify peak maxima and minima. This is termed a first-derivative spectrum. First-derivative spectra have their uses but they are difficult to interpret (as the brain often sees the ‘peaks’ rather than the true information). If we take the secondderivative spectrum (by derivatizing the absorbance spectrum twice), we obtain a plot such as that in Figure 5. The second-derivative spectrum can be thought of as an inverted spectrum. Sharp peaks will be made even sharper. Broad peaks (and also broad background Peak Point of inflection Abs Trough D1 0 200 210 220 230 240 250 260 270 280 290 300 310 Wavelength (nm) Figure 4 Explanation of the first-derivative (D1) spectrum, and its relationship to the absorption spectrum (Abs). D2 Broad peak almost lacking in D2 spectrum Some peak shoulders Note sharper peak Sharp peak Broad peak Abs 200 250 300 350 400 450 500 550 600 650 Wavelength (nm) Figure 5 Second-derivative (D2) spectrum showing sharp band discrimination. features) will become flattened and so the technique can be used both as a peak-enhancement and background-rejection tool. The second-derivative spectrum, like its absorbance counterpart, still contains quantitative information. If two points are consistently used on the spectrum and the difference in their values on the ordinate is taken, this can be plotted against concentration and a linear relationship established. Derivative spectra represent an alternative presentation of the original data. Information cannot be created and so there is a cost involved. This cost is at the expense of a much poorer signal-to-noise ratio (as the noise is also being derivatized) and so if a requirement for derivative spectroscopy is anticipated, an instrument with a good noise specification is highly desirable. Single-beam instruments should not be considered for serious derivative spectroscopy. Higher order derivatives also are possible, and usually up to the fourth derivative is offered on current instrumentation, but the increased noise makes their general analytical use questionable. 2.6 Verification of Spectrophotometer Performance Clinical analysis is concerned with producing an accurate result to enable the clinician to make an accurate diagnosis and to provide the correct treatment. It is important, therefore, that all equipment used to make the diagnosis is well maintained and that the operators have a sufficient skill level to understand the limitations of the instrument and to use the correct operating and sampling procedures. Instruments should be checked regularly, using a certified reference material (CRM). As a minimum, the user should possess a sample for checking wavelength 6 CLINICAL CHEMISTRY accuracy and a set of absorbance filters. Wavelength standards should never be used to check absorbance accuracy and vice versa. Wavelength standards (such as holmium oxide glass filters) have very sharp peaks whereas absorbance standards such as the National Institute of Standards and Technology (NIST) 930D filters are of neutral density. Additional checks such as for stray light and noise may also be advantageous. Most instrument companies will be able to give advice on instrument performance checks and routine maintenance. Microplate reader users are more limited in the choice of calibration aids. For filter-based instruments (the majority at the time of writing), there is no way to check wavelength accuracy (other than to scan the filter on a spectrophotometer) and there are few CRMs available for all formats of microplates. If one is using a microplate reader, the manufacturer should be contacted for advice. 3 OVERVIEW OF INSTRUMENT DESIGNS AND THEIR ADVANTAGES AND DISADVANTAGES 3.1 Dispersive and Diode-array Systems Before going into details of analysis, it is important to discuss the design of a UV/VIS specrophotometer and the implications of the various design types for a particular analysis, and to understand the limiting factors in making that measurement. UV/VIS instruments are available in two main types, dispersive and photodiode array (usually shortened to diode array). The dispersive design uses a monochromator before the sample to convert the white light produced by the light source into a single pure wavelength of light. This single wavelength is then passed through the sample and detected. The monochromator can be either a fixed-wavelength filter or a variable-wavelength design such as a prism (rare nowadays) or a diffraction grating. On higher specification instruments, there may be two monochromators linked in series to permit higher performance – particularly at high absorbance values (e.g. over 3.0 AU). 3.3 Single-beam Spectrophotometers The single-beam spectrophotometer is the simplest optical configuration. It consists of a light source, monochromator (either a grating or a filter), the sample area and the detector, as shown in Figure 6. In the singlebeam design, it is necessary first to zero the instrument (to establish the I0 value) and then to measure the sample. Single-beam instruments are used mainly on grounds of cost. They have poorer noise specifications compared with their dual- and double-beam counterparts and are prone to drifting with time. This makes accurate kinetics and applications involving repetitive sampling over time more difficult. The cheaper models often lack the spectral resolution demanded by some clinical applications (e.g. porphyrin analysis). 3.4 Double-beam Spectrophotometers In the double-beam design as shown in Figure 7, there is still a single detector – usually a photomultiplier (a phototube). The beam is then sent alternately through sample and reference positions using a chopper wheel or vibrating mirror. The electronics in the instrument are also able to synchronize the beam switching with the detector so that it can distinguish whether the detector is measuring the sample or reference beam at any one time. Even in complete darkness, a photomultiplier will output a signal. This is known as the dark current. As a result, the beam shuttling device will also have some means of temporarily blocking the light from both beams so that this residual signal (the dark current) can be measured and subtracted from each sample and reference measurement. Tungsten lamp (for visible region) Mirror Deuterium lamp (UV models only) Mirror (for source change) Filter wheel Entrance slit 3.2 Dispersive Ultraviolet/Visible Spectrophotometers ž ž ž ž single beam double beam (single detector) dual beam (dual detector) photodiode array. Mirror Exit slit Dispersive UV/VIS spectrophotometers have four main optical configurations: Diffraction grating (monochromator) Mirror Figure 6 Single-beam optical configuration. Sample Detector 7 UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY Tungsten lamp Source mirror Plane mirror Deuterium lamp Light beam Plane mirror Spherical mirror Holographic grating Open Mirror S R ¢ , Q ¢Q,¢Q, Slit Chopper assembly Blank portions for zeroing detector dark current Spherical mirror Spherical mirror Reference cell Optical chopper Collimating mirror Plane mirror Spherical mirror Spherical mirror Sample cell Photomultiplier detector Figure 7 Double-beam (chopper wheel) optical layout. Tungsten lamp Mirror Mirror Deuterium lamp Filter wheel Entrance slit Mirror Reference Mirror Beam splitter (half-silvered mirror) Exit slit Mirror Sample Monochromator Figure 8 Dual-beam spectrophotometer optical layout. Photodiode detectors 8 CLINICAL CHEMISTRY 3.5 Dual-beam Spectrophotometers An alternative to the double-beam design is the dualbeam layout (Figure 8). In this design, the beam is split using a half-silvered mirror (beam splitter) into its sample and reference components. Each beam has its own detector. This design is only practical with solid-state detectors (which have fairly constant dark current) and gives equivalent results compared with a double-beam system for most analyses. The design removes the need for a mechanical beam shuttling device (and hence improves reliability) and, as solid-state detectors are used, there is no need for a high-tension power supply to provide the high voltages (around 1000 V) which are required to set the photomultiplier gain. The design also produces very good baseline noise characteristics as, again, there is no contribution from the mechanical beam shuttle. If the design has a weakness, it is at very high absorbance (over 3 AU) as the photomultiplier is able to detect lower light levels than solid-state detectors. Routine clinical analyses rarely exceed these absorbance values and, in any case, a single monochromator instrument is limited by its stray light (see later). If samples exceed the upper absorbance limit of a spectrophotometer, they can either be diluted or a shorter path length cell can be used. 3.6 Photodiode-array Spectrophotometers Photodiode-array spectrophotometers have been available since the early 1980s with the advent of the early designs from Hewlett-Packard (now Agilent) (Figure 9). The design is basically a single-beam instrument but the sample is irradiated with white light (as opposed to monochromatic light in a dispersive instrument). This light, after it has passed through the sample, is then dispersed by a dispersion monochromator (often referred Diode array Polychromator Sample Source Dispersion device Entrance slit Figure 9 Diode-array spectrophotomer optical layout. to as a polychromator) on to a special solid-state detector with individual segments, one for each wavelength. The main appeal of these instruments is that the measurement of a spectrum takes only a few seconds. The system has some disadvantages, however. A diode-array spectrophotometer is a single-beam instrument (although a nonanalytical wavelength may be used as a pseudoreference to overcome nonwavelength-specific drift). It is also less suitable for some single-wavelength measurements as a whole spectrum has to be collected irrespective of whether the data points are required or not. The design is also more prone to errors from sample fluorescence (as the sample irradiation is at all wavelengths and so any fluorophore present will be also excited) and any nonparallel surfaces in the sample (as this will affect the beam dispersion on to the individual elements in the array). Nevertheless, the diode-array system offers a high throughput of scanned data and the ability also to visualize whole spectrum for single-wavelength analyses so that any unexpected results can be investigated further. 3.7 Microplate Reader Spectrophotometers Over the past 20 years, many clinical analyses have been transferred from the traditional, cuvette-based spectrophotometer to a microwell (normally 96-well) format. The microwell started life in the early 1960s for microbiological culture. Later, it was realized that the format could be applied to bulk analysis using clear microplates and a dedicated reader. Microplates are manufactured from plastic (usually polystyrene or acrylic, depending on the required wavelength range). They are cheap, disposable and provide a universal format. The plates also have the advantage that they are compatible with liquid handling devices such as plate fillers and washers. Although 96 wells is the most common format, the requirement for greater speed and throughput has seen the introduction of even higher density formats such as 384 wells per plate. The dedicated reader is really a spectrophotometer in an applied form. Most plate readers work in the visible region only (as the polystyrene microplates absorb in the UV region) and use optical filters rather than monochromators. More sophisticated readers may also offer multiple reading modes such as fluorescence and bioluminescence in addition to absorbance. Many modern readers can also be used in conjunction with a robotic system. In terms of performance, there is a compromise compared with using a spectrophotometer, but for many assays this is far outweighed by the reduced costs and greater convenience which this format offers. UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY 3.8 Reflectance-based Analyzers In recent years, reagent manufacturers have investigated ways of making tests even more simple to perform and less dependent on expensive analytical equipment. An example of this is the portable glucose monitoring systems which diabetics use to check their blood sugar levels. The color reaction is performed on a solid support which is coated with the required reagents. This support is usually a small stick or strip. After exposure to a blood or urine sample, this support is inserted in the analytical device and the reading displayed. These devices are based on reflectance rather than absorbance (as the supports are opaque it is not possible to pass light through them). When light falls on a surface it can be reflected in two main ways, as either specular or diffuse reflectance. Specular reflectance (from the Latin word speculum for mirror) is the study of mirror-like reflectance. The path of the reflected ray of light is entirely predictable as it should be at the same angle as the angle of light incidence. In diffuse reflectance, the surface has a matt surface which scatters the reflected light in all directions and this scattered reflectance can be collected by a detector. In practice, a sample may exhibit both types of reflectance (e.g. a coating with a glossy surface) and so the geometry of the collection sphere can be adjusted either to include or exclude the specular component. Reflectance is normally expressed as a percentage compared with a standard – normally a white surface such as Teflon . The relationship between reflectance and concentration is much less clearly defined when compared with absorbance as there are physical factors to consider (e.g. particle size, layer thickness). A fairly accurate quantitative result can be obtained by taking the logarithm of reflectance or by using the Kubelka – Munk equation. Manufacturers of reflectancebased devices need to spend considerable development work in providing an accurate calibration which can be stored inside the instrument to produce the correct results. These results will need to be verified by regulatory bodies Test strip Blood Membrane LED Detector Figure 10 Principle of reflectance-based hand-held analyzer for diabetes monitoring. 9 such as the US Food and Drug Administration (FDA) before such a device can be marketed. As many of these devices are designed for use in the home or general practitioner’s surgery, they must be manufactured as cheaply as possible. As a result, an LED can be used in place of a light source and monochromator. Detection is by means of a silicon photodiode or other solid-state detector. A diagram of a reflectance-based analyser for the measurement of blood sugar for diabetes monitoring is shown in Figure 10. 4 COMMON CLINICAL APPLICATIONS USING ULTRAVIOLET/VISIBLE ABSORPTION SPECTROSCOPY There are many clinical tests which employ UV and visible spectrophotometry. For readers who want a detailed and exhaustive list, there are many textbooks on the subject..1/ In this section I have highlighted a range of these tests and detailed how they work. 4.1 Enzyme Rate Assays Enyzmes are biocatalysts, which are extremely efficient in converting their chosen substrates into product. Apart from their efficiency, they are also highly specific and often will not work with a slightly different substrate. Often it is useful to study the rate of this catalysis by measuring either the rate of depletion of substrate or the formation of products. This may be a matter of simply measuring the absorbance of one of the reaction components directly or by forming an absorbing conjugate with another molecule. Enzyme kinetics are usually zero order. This means that, after an initial lag phase, there should be a linear relationship between substrate (or product) concentration with time until one of these components becomes limiting. It is therefore useful if the instrument software is able to allow the user to choose where this linear portion is (either prior to or, better, after data collection) and to use this portion to calculate the rate. The enzyme activity is normally expressed in International Units (IU) by applying a simple factor to the measured slope (absorbance/time). Enzyme rate assays are nearly always performed at a single wavelength (340 and 405 nm are commonly used) and require a temperature-controlled environment. This may take the form of a simple water-jacketed cell holder where water (or other liquid) is passed through the water jacket at a constant temperature (supplied by a thermostated water circulator). Some cell holders use thermoelectric (or Peltier effect) cell holders. These cell 10 CLINICAL CHEMISTRY holders have the advantage of much more precise temperature control and the ability to work below ambient temperatures (Peltier cells can cool by reversing the electric current flow). Some Peltier designs, particularly those requiring high or low temperatures, will still require a flow of cold water in order to operate correctly whereas those covering a more restricted range do not. Most enzyme reactions are fairly slow, taking place for 5 min or more. In order to increase productivity, most UV/VIS instruments offer a cell changer as an accessory. This is a shuttle device, which can hold six or more cuvettes at once. The instrument then cycles through each of the cell positions taking a reading on each cell every 30 s during the course of the reaction. The collected data can be analyzed either using the instrument’s own kinetic software or externally, using either a computer or manual calculation. Some statistical data on the quality of the curve fit are also useful. An example of a clinical rate assay is the determination of butyrylcholinesterase (BchE). Certain individuals express a mutant form of the BchE gene. This then encodes for a defective form of the enzyme, which lacks the ability to hydrolyze succinylcholine. In some rare cases, the complete BchE gene is missing. A defective or missing gene will not, normally, be of any consequence. If, however, succinylcholine is used during tracheal intubation in the administration of inhalation anesthetics, this will then cause the patient to undergo complete paralysis. The test for this enzyme.2/ is commonly performed using a UV/VIS spectrophotometer with a temperature-controlled cell holder (most tests will be performed at 37 ° C). One important class of enzyme-catalyzed reactions involves the oxidation and reduction of pyridine nucleotides [nicotinamide adenine dinucleotide (NADC ) and nicotinamide adenine dinucleotide (reduced form) (NADH), respectively]. If the reaction is followed at 340 nm, NADC does not absorb whereas NADH shows a strong absorbance. Examples of NADC /NADH kinetic reactions include glucose dehydrogenase,.3/ aspartate aminotransferase.4/ and urea..5/ Other enzymatic tests often include a colorless compound, which is added to the reaction. This is then enzymatically converted to a colored product (e.g. p-nitrophenol). Examples of this type of test include alkaline phosphatase,.6 – 8/ acid phosphatase.4/ and amylase..1/ These tests are included in the summary of common clinical tests in Table 3. 4.2 Colorimetric and End-point Assays It is also possible to perform a reaction to completion and then to calculate the quantity of initial substrate by extrapolation. This type of assay is termed an endpoint assay. There are a vast number of such tests and, if an exhaustive list is sought, the reader is directed to a compendium of methods such as Tietz..1/ A summary of some common clinical end-point analyses is given in the summary of common clinical tests in Table 3. The methods will prescribe a time after which the reading can be taken. In the case of enzyme-catalyzed reactions, the incubation time will need to be at constant temperature. Most diagnostics companies provide premixed reagents to perform these tests together with a detailed protocol describing their use. Different protocols may use slightly Table 3 Some common clinical tests Analyte .4/ Acid phosphatase Alanine aminotransferase.9/ Alkaline phosphatase.6 – 8/ a-Amylase.1/ Aspartate aminotransferase.10/ Bilirubin.11/ Cholesterol.12/ Creatinine.13/ GGT.14/ Glucose.15/ LDH.16/ Porphyrins (total).17/ Pseudocholinesterase.28/ Triglycerides.18,19/ Urea.20/ Method UV wavelength (nm) Kinetic: PNP Kinetic: NADC /NADH Kinetic: PNP Kinetic: 2-chloro-4-nitrophenylmaltoheptaoside 2-chloro-PNP Kinetic: NADC /NADH 405 340 405 405 Evelyn – Molloy Kinetic: cholesterol oxidase Jaffe Kinetic: carboxy substrate Kinetic: hexokinase (NADC /NADH) Kinetic: lactate/pyruvate Acidification using HCl NADC /NADH Kinetic: GPO colorimetric Kinetic: NADC /NADH 340 555 500 510 405 340 340 Absorbance ¾ 405 (Soret peak) 340 520 340 PNP, p-nitrophenyl phosphate; GGT, g-glutamyl transferase; LDH, lactate dehydrogenase; GPO, glycerol-3-phosphate oxidase. 11 UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY 4.3 Immunoassays, Enzyme-linked Immunosorbent Assays and Microplate Assays Immunoassays rely on the very strong affinity between an antibody and its target molecule (antigen). This strong affinity has been used to design a wide range of assays for a variety of targets. These include pathogens (where a chemical associated with the organism or virus will be targeted), tumor markers and drug monitoring (either therapeutic or drugs of abuse). In fact, anything which can elicit an antibody response can be developed into an immunoassay. These assays are ideal where high specificity is required. They are not good at dealing with a range of possible compounds. For example, it is difficult to design an immunoassay to detect all abused drugs, only specific types. If a ‘‘designer’’ drug is synthesized with an additional functional group, this may adversely affect the assay. Immunoassays are competitive assays. The reaction mixture will contain antigens labeled with some kind of tag (this is either a radiolabel, a fluorophore or a site which will bind to a chromophore). When the (unlabeled) sample antigens are introduced, there will be competition between the labeled and unlabeled antigens and this can be calibrated against a binding curve (which will be sigmoidal in nature). Prior to measurement, it will be necessary to separate the free and bound antigens and so a separation step will be required (heterogeneous assay). Much effort has been spent in previous years trying to simplify this process (e.g. using magnetized, latex-covered beads) or using a technique which inherently separates bound from unbound antigens (e.g. fluorescence polarization) to produce a homogeneous assay. For the highest sensitivity immunoassays, either radioactivity or fluorescence (or time-resolved fluorescence) has to be used. In situations where lower sensitivity is acceptable, an absorption-based assay can be employed. A popular assay type is the enzyme-linked immunosorbent assay (ELISA). In this assay, an antibody (specific to the analyte) is coated on the bottom of the microplate. In some cases, any exposed area on the microplate (i.e. any area where the antibody has not been coated) is blocked using bovine serum albumin (BSA) and the excess antibody is washed away. The blocking agent is to help prevent unbound antigen from adhering directly to the plate, thus affecting the final result. The analyte and enzyme conjugate [e.g. horseradish peroxidase (HRP)] is added. The analyte will bind to the antibody, which has previously been coated on the microplate. The enzyme conjugate also binds to the analyte. This will be used later in conjunction with a specific dye to produce the color, which will then be measured on the reader. 4.4 Porphyrin Analysis Porphyria is the name given to a number of related conditions, some genetic, which result from an over production of porphyrins, which are precursors in the production of hemoglobin. Sufferers are prone to bouts of severe abdominal pain, vomiting, severe personality changes and sensitivity to light. Some types of porphyria produce characteristic dark-colored (‘‘port wine’’) urine and this is a good first indication that porphyria is present. One of the main types of porphyria (a generic term for porphyrin-related disease) is variegate porphyria. In this case a mitochondrial enzyme called protoporphyrinogen oxidase is defective (owing to incorrect genetic coding) and as a result excess protoporphyrin (one of the porphyrin types) is produced. The protoporphyrinogen reacts with oxygen to produce protoporphyrin in an uncontrolled reaction. Other porphyria types include acute intermittent porphyria. Accurate diagnosis of the exact type of porphyria is vital as incorrect treatment could have very serious consequences. Porphyrins.17/ have a characteristic UV/VIS absorption peak (Soret peak) in the region 400 – 410 nm depending on the type of porphyrin present (coproporphyrin has a peak between 402 and 403 nm whereas the uroporphyrin peak lies between 406 and 407 nm). The urine sample is filtered, diluted with distilled water and acidified with hydrochloric acid. The sample is scanned between 300 and 500 nm and the spectrum peak positions are noted. The measurement is taken by first constructing a baseline at points at either side of the main peak (usually around 380 and 430 nm) and then measuring the height of the peak down to this baseline (Figure 11). Absorbance altered wavelengths for each analyte. As with rate assays, the test may be based on reading the analyte directly or an additional color reaction may be required to develop the test. 380 405 430 Wavelength (nm) Figure 11 Porphyrin analysis using three wavelengths. 12 CLINICAL CHEMISTRY total porphyrin.µg L 1 / D 2A.lmax / .A380 C A430 /e .4/ where A is absorbance, lmax is the wavelength at maximum absorption and e is the molar absorptivity (a constant) for the analyte; for porphyrins (in a 1-cm cell) e D 4740 µg L 1 . Alternatively, second-derivative spectroscopy has been used.1/ (as this reduces background effects and produces sharper peaks). It should be borne in mind that, for a full and correct diagnosis, the type of porphyrin must be accurately identified. This can only be done using a good UV/VIS spectrophotometer offering narrow slits and a skilled user, as interpretation of the corrected spectrum or the second-derivative spectrum may be involved. UV/VIS absorption spectroscopy is generally used for screening and other techniques such as high-performance liquid chromatography (HPLC) or fluorescence spectroscopy (which gives much better selectivity as each porphyrin has a different excitation and emission wavelength) are often used to make the final, confirmatory, diagnosis. These techniques are usually offered by porphyria reference centers. 4.5 Hemoglobin Analysis Hemoglobin is a protein with a nonprotein core consisting of an iron atom surrounded by heme groups. It has remarkable oxygen transportation properties where it can change its conformation to accept oxygen (oxyhemoglobin). This process can be inhibited by carbon monoxide, which has a 200 times stronger affinity for hemoglobin (carboxyhemoglobin) than oxygen, resulting in severe respiratory problems and death in cases of carbon monoxide poisoning. Hemoglobin possesses an iron atom core in its ferrous (Fe2C ) state. If the iron is oxidized to its ferric (Fe3C ) state, its oxygen transport capabilities are diminished and the molecule is called methemoglobin (metHb). Total hemoglobin can be measured by performing a reaction of the total hemoglobin present with potassium cyanide to form a hemoglobin– cyanide complex (Figure 12). This is the basis of the method of Zijlstra et al..20/ In this method, hemoglobin is reacted with potassium cyanide (taking great care with pipetting and certainly never by mouth!) and sodium (or potassium) hexacyanoferrate(III) to produce a hemoglobin– cyanide complex (Equation 5): hemoglobin C CN C Fe(CN)6 3 ! hemoglobin– cyanide .5/ Absorbance The total porphyrin concentration is given by Equation (4): 0.300 0.280 0.260 0.240 0.220 0.200 0.180 0.160 0.140 0.120 0.100 0.080 0.060 0.040 0.020 0.000 470 500 520 540 560 580 600 620 640 660 680 700 720 750 Wavelength (nm) Figure 12 Absorption spectrum of hemoglobin – cyanide complex. This complex has a peak around 546 nm, which can be measured and quantitated. Franzini et al..21/ have described a method based on second-derivative spectroscopy to measure hemoglobin and its homologs. This method helps to overcome the interference from bilirubin, which is also often present in these analyses. Shih et al..22/ also used multicomponent analysis in order to quantitate carboxy-, met- and oxyhemoglobin independently from a single scan. This is a statistical approach which compares each data point in a spectrum with a calibration set of known references – either mixtures or single components – and attempts to calculate the relative proportions of each in the unknown spectrum. This approach has its attractions as it is potentially able to measure each component without the need for a separation step. The main drawback is when there is significant spectral overlap or in situations where the concentrations of the various components differ widely. Problems may also occur if there is a strong background matrix which is not constant. More powerful techniques exist, such as principle component regression or partial least-squares fitting. These techniques are a science in themselves (chemometrics) and go beyond this article. 4.6 Protein Assays Proteins are composed of amino acid building blocks. Protein has some intrinsic absorbance at approximately 280 nm (from the aromatic amino acids – tyrosine and tryptophan) but it is more common to perform a reaction to produce a colored complex which can be assayed in the visible region. The three most common procedures for protein analysis are biuret, Bradford and bicinchoninic acid (BCA) assays. Table 4 lists the various protein methods. These are all simple colorimetric determinations. 13 UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY Table 4 Summary of protein assays Assay method and reference Principle Lowry.23/ Bradford.24/ Biuret.25/ BCA.26/ Absorbance at 280 nm.23/ Warburg – Christian.27/ Range (µg mL 1 ) As biuret plus determination of aromatic amino acids Dye binding with coomassie brilliant blue Determination of number of peptide bonds Reduction of copper by protein and formation of Cu(I) – BCA complex Determination of tyrosine and tryptophan in protein Determination of aromatic amino acids with compensation for nucleic acids Absorbance 1.10 1.00 0.80 0.60 0.40 0.20 0.00 220 240 260 280 300 320 340 Wavelength (nm) Figure 13 Absorption spectrum of DNA. 4.7 Molecular Biology The use of UV/VIS spectroscopy for molecular biology strictly falls outside the scope of clinical analysis. On the other hand, more routine clinical laboratories are using molecular biology techniques (such as the PCR and automated dideoxy sequencing) as these give more direct diagnosis for genetically based disorders. As a result of these techniques, UV/VIS spectroscopy is useful for assessing the purity of the starting template in either a sequencing or PCR reaction and, as a result, saves time in optimizing the reaction and helps to reduce reagent costs. Pure DNA and RNA absorb at 260 nm (Figure 13). Protein (which is the main source of contamination) absorbs at around 280 nm (this is dependent on the exact amino acid composition as individual amino acids have slightly different absorption maxima). There is a rule of thumb which is now widely adopted in molecular biology laboratories as a quick method for assessing purity. This method measures the absorbance at 260 and 280 nm and the ratio (A260 /A280 ) 5 – 200 10 – 200 Interferences Phenols, aromatic amino acids Detergents 200 – 5000 Amines, ammonium salts 200 – 1200 High concentrations of metals, strong reducing agents, chelating agents Nucleic acids, phenols, aromatics >50 50 – 3000 purity check Phenols, aromatics is calculated. Optionally, a third reference point can be taken at 320 nm (to assess the amount of turbidity and scatter) and this absorbance value can be subtracted from either of the two absorbance values prior to calculating the ratio. If the ratio of the two absorbances is between 1.7 and 2.0, then the DNA preparation is considered to be pure. If it is >2, then there is probably a high RNA content. A lower ratio would indicate a high protein or phenol content (a reagent commonly used in DNA extraction). One major issue in molecular biology is sample volume. It is not uncommon to have volumes of 10 µL and so special low-volume cells are available. These special cuvettes are made from quartz (as plastic and glass cuvettes generally absorb below 300 nm). Dedicated lowcost instruments are available for the assessment of nucleic acid purity. ACKNOWLEDGMENTS I thank Hanswilly Müller at PerkinElmer, Überlingen, Germany, for providing some of the spectra shown here, Jackie Woolf at the Porphyria Reference Centre, Heath Park Hospital, Cardiff, and Ipswich Hospital, UK, for some information and spectra of porphyrins and Chris Royle at the Brompton Hospital, UK, for keeping me up to date with the latest developments in clinical analysis. I also thank Agilent Technologies (formerly HewlettPackard Instruments) and Hypoguard for permission to use their diagrams. ABBREVIATIONS AND ACRONYMS BchE BSA Butyrylcholinesterase Bovine Serum Albumin 14 CRM ELISA FDA GGT GPO HPLC HRP IR LDH LED metHb NADC NADH NIST PCR PNP TRIS UV UV/VIS CLINICAL CHEMISTRY Certified Reference Material Enzyme-linked Immunosorbent Assay Food and Drug Administration g-Glutamyl Transferase Glycerol-3-phosphate Oxidase High-performance Liquid Chromatography Horseradish Peroxidase Infrared Lactate Dehydrogenase Light-emitting Diode Methemoglobin Nicotinamide Adenine Dinucleotide Nicotinamide Adenine Dinucleotide (Reduced Form) National Institute of Standards and Technology Polymerase Chain Reaction p-Nitrophenyl Phosphate Tris(hydroxymethyl)aminomethane Ultraviolet Ultraviolet/Visible RELATED ARTICLES Biomedical Spectroscopy (Volume 1) Biomedical Spectroscopy: Introduction ž Glucose, In Vivo Assay of ž Infrared Spectroscopy in Clinical and Diagnostic Analysis ž Infrared Spectroscopy in Microbiology ž Near-infrared Spectroscopy, In Vivo Tissue Analysis by REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Biomolecules Analysis (Volume 1) Biomolecules Analysis: Introduction Carbohydrate Analysis (Volume 1) Disaccharide, Oligosaccharide and Polysaccharide Analysis ž Glycolipid Analysis ž Monosaccharides and Sugar Alcohol Analysis Clinical Chemistry (Volume 2) Atomic Spectrometry in Clinical Chemistry ž Diagnostic Hematology ž Gas Chromatography and Mass Spectrometry in Clinical Chemistry ž Immunochemistry ž Infrared Spectroscopy in Clinical Chemistry ž Laboratory Instruments in Clinical Chemistry, Principles of ž Nucleic Acid Analysis in Clinical Chemistry ž Phosphorescence, Fluorescence, and Chemiluminescence in Clinical Chemistry ž Serum Proteins 13. 14. 15. 16. 17. C. Burtis, E.R. Ashwood (eds.), Tietz Textbook of Clinical Chemistry, 2nd edition, W.B. Saunders, Philadelphia, 1994. R.T. Evans, J. Wroe, ‘Is Serum Cholinesterase Activity a Predictor of Succinylcholine Sensitivity? An Assessment of Four Methods’, Clin. Chem., 24, 1762 – 1766 (1978). D. Barham, P. Trinder, ‘An Improved Colour Reagent for the Determination of Blood Glucose by the Oxidase System’, Analyst, 97, 142 – 145 (1972). Deutsche Gesellschaft für Klinische Chemie, Z. Clin. Chem. Klin. Biochem., 8, 658 (1970); 9, 464 (1971); 10, 182 (1972). H. Talke, G.E. Schubert, Klin. Wochenschr., 42, 172 (1965). H.U. Bergmeyer, Methods of Enzymatic Analysis, VCH, Weinheim, 1986. ‘Biochemica Information’, Boehringer Mannheim, Mannheim, 1975. W.F. Gohara, ‘Rate of Decrease of Glutamyltransferase and Acid Phosphatase Activities in the Human Vagina after Coitus’, Clin. Chem., 26, 254 – 257 (1980). Expert Panel on Enzymes, International Federation of Clinical Chemistry, ‘IFCC Methods for the Measurement of Catalytic Concentrations of Enzymes’, Clin. Chim. Acta, 105, 147F – 154F (1980). R.J. Henry, N. Chiamori, O.J. Golub, S. Berkman, ‘Revised Spectrophotometric Methods for the Determination of Glutamic – Oxaloacetic Transaminase, Glutamic – Pyruvate Transaminase and Lactic Acid Dehydrogenase’, Am. J. Clin. Pathol., 34, 381 – 398 (1960). J.B. Henry (ed.), Clinical Diagnosis and Management by Laboratory Methods, 18th edition, W.B. Saunders, Philadelphia, 1991. G.R. Cooper, P.H. Duncan, J.S. Hazelhurst et al., ‘Cholesterol, Enzymatic Method’, in Selected Methods of Clinical Chemistry: Selected Methods for the Small Clinical Chemistry Laboratory, eds. W.R. Faulkner, S. Meites, American Association for Clinical Chemistry, Washington, DC, 1982. R.J. Henry, D.C. Cannon, J.W. Winkelman (eds.), Clinical Chemistry: Principles and Techniques, 2nd edition, Harper and Row, Hagerstown, MD, 1974. S.B. Rosalki, ‘Gamma Glutamyl Transpeptidase’, Adv. Clin. Chem., 17, 53 – 107 (1975). ‘Chemstrip 10 Package Insert’, Boeringer-Mannheim, Indianapolis, IN, 1992. D. McKenzie, A.R. Henderson, ‘Electrophoresis of Lactate Dehydrogenase Isoenzymes’, in Standard Methods of Clinical Chemistry, ed. G.R. Cooper, American Association for Clinical Chemistry, Washington, DC, Vol. 10, 1983. G.H. Elder, S.G. Smith, S.J. Smyth, ‘Laboratory Investigation of the Porphyrias’, Ann. Clin. Biochem., 27, 395 – 412 (1990). UV/VIS LIGHT ABSORPTION SPECTROPHOTOMETRY IN CLINICAL CHEMISTRY 18. 19. 20. 21. 22. G.R. Warnick, ‘Enzymatic Methods for Quantification of Lipoprotein Lipids’, Methods Enzymol., 129, 101 – 123 (1986). M.W. McGowan, J.D. Artiss, D.R. Strandbergh, B. Zak, ‘A Peroxidase-coupled Method for the Colorimetric Determination of Serum Triglycerides’, Clin. Chem., 29, 538 – 542 (1983). W.G. Zijlstra, A. Buursma, W.P. Meeuwsen-van der Roest, ‘Absorption Spectra of Human Fetal and Adult Oxyhemoglobin, De-oxyhemoglobin, Carboxyhemoglobin and Methemoglobin’, Clin. Chem., 37, 1633 (1991). C. Franzini, G. Cattozzo, A. Pagani, ‘Serum Hemoglobin Measurement by Second Derivative Spectroscopy’, Int. Lab., October, 33 – 39 (1988). M.L. Shih, W.D. Korte, C.R. Clark, ‘Multicomponent Spectroscopic Assay for Hemoglobin and Ferrihemoglobin Species in Methemoglobin Treatment of 23. 24. 25. 26. 27. 28. 15 Cyanide Poisoning’, J. Anal. Toxicol., 21(7), 543 – 547 (1997). E. Layne, Methods Enzymol., 3, 447 – 454 (1957). M.M. Bradford, ‘A Rapid and Sensitive Method for the Quantitation of Microgram Quantities of Protein Utilizing the Principle of Protein – Dye Binding’, Anal. Biochem., 72, 248 – 254 (1976). A.G. Gornall, C.S. Bardawill, M.M. David, J. Biol. Chem., 177, 751 (1949). C.V. Sapan, R.L. Lundblad, N.C. Price, ‘Colorimetric Protein Assay Techniques’, Biotechnol. Appl. Biochem., 29(2), 99 – 108 (1999). O. Warburg, W. Christian, Biochem. Z., 310, 384 (1941). J.R. Huizenga, C.H. Gips, ‘Evaluation of the UV-340 Spectrophotometric Determination for Pseudocholinesterase Activity (EC 31.1.8) in Human Serum’, J. Clin. Chem. Clin. Biochem., 25(3), 161 – 165 (1987).