Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
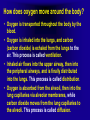
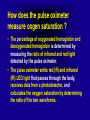
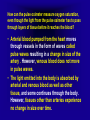
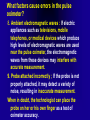
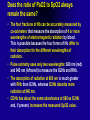
PULSE OXIMETER BY AHMAD YOUNES PROFESSOR OF THORACIC MEDICINE Mansoura faculty of medicine Hypoxia and Oxygenation • Hypoxia is low oxygen tissue content, resulting from inadequate oxygen delivery to meet their oxidative requirements. • There are four basic types of hypoxia. 1- Hypoxic hypoxia occurs when there is a deficiency in oxygen exchange in the lungs. Some causes include: • Decreased partial pressure of oxygen available at altitude. • Conditions that block the exchange at the alveolar capillary level (e.g. pneumonia, pulmonary edema, asthma, drowning). Hypoxia and Oxygenation 2-Anemic hypoxia occurs when the body cannot transport the available oxygen to the target tissues. Causes include: • Anemia from acute or chronic blood loss. • Carbon monoxide poisoning. • Medications such as sulfonamides and nitrites. • Methemoglobinemia. • Sickle cell disease. Hypoxia and Oxygenation 3- Stagnant hypoxia occurs when there is insufficient blood flow. Causes include: • Heart failure. • Decreased circulating blood volume. • Vasodilatation. • Continuous positive pressure ventilation. Hypoxia and Oxygenation 4- Histotoxic (histologic) hypoxia occurs when the body’s tissues are not able to use the oxygen that has been delivered to them. This is not a “true hypoxia” because the tissue oxygenation levels may be at or above normal. Causes include: • Cyanide poisoning. • Alcohol consumption. • Narcotics. Hypoxemia • Hypoxemia is a condition in which there is an inadequate amount of oxygen in arterial blood (decreased PaO2, SaO2, or hemoglobin content). • Hypoxia (low O2 content, low cardiac output, or low oxygen uptake at the tissue level) occurs whether hypoxemia is present or not. • In adults, children, and infants older than 28 days, hypoxemia exists when the PaO2 is less than 60 mmHg or the arterial oxygen saturation (SaO2) is less than 90% when breathing room air. If the partial pressure of O2 (PaO2) is less than the level predicted for the individual’s age, hypoxemia is said to be present. Predicted Pao2 = 105 - 1/2 age (year) • oxygen is a treatment for “hypoxemia, not breathlessness”. Further, “oxygen has not been shown to have any effect on the sensation of breathlessness in non-hypoxemic patients” • The main goal of oxygen therapy is:“To treat or prevent hypoxemia thereby preventing tissue hypoxia which may result in tissue injury or even cell death” Some of the causes of hypoxemia are: • • • • • • Low inspired PO2 (e.g., at high altitude). Hypoventilation, V/Q mismatch (e.g., COPD). Anatomical Shunt (e.g., cardiac anomalies). Physiological Shunt (e.g., atelectasis). Diffusion deficit (e.g., interstitial lung disease). Hemoglobin deficiencies. What is a pulse oximeter ? • Oxygen binds to hemoglobin in red blood cells when moving through the lungs. It is transported throughout the body as arterial blood. • A pulse oximeter uses two frequencies of light (red and infrared) to determine the percentage (%) of hemoglobin in the blood that is saturated with oxygen. • The percentage is called blood oxygen saturation, or SpO2. • A pulse oximeter also measures and displays the pulse rate at the same time it measures the SpO2 level. Pulse oximetry • Clinical recognition of decreased arterial oxygen saturation of haemoglobin (SaO2) is subjective and unreliable, with the classic sign of cyanosis appearing late when Sao2 is between 80 - 85%. • Pulse oximetry is simple to use, relatively cheap, noninvasive and provides an immediate, objective measure of Sao2. • It is now used widely in all in-hospital settings and increasingly in both primary care and the pre-hospital environment. • Oxygen saturation, ‘the fifth vital sign’, now also forms a component of many early warning systems to identify the deteriorating patient. What can be learned by monitoring blood oxygen saturation? • Each lung contains nearly 300 million alveoli which are surrounded by blood capillaries. • Since alveolar walls and capillary walls are very thin, oxygen passing into the alveoli immediately transfers into the blood capillaries. (Usually in adults, the transfer would take about 0.25 seconds while resting.) • A large proportion of the oxygen diffusing into the blood binds to hemoglobin in the red blood cells, while a part of the oxygen dissolves in the blood plasma. • The amount of oxygen transported around the body is determined mainly by the degree to which hemoglobin binds to oxygen (lung factor), hemoglobin concentration (anemic factor), and cardiac output (cardiac factor). What can be learned by monitoring blood oxygen saturation? • Oxygen saturation is an indicator of oxygen transport in the body, and indicates if sufficient oxygen is being supplied to the body, especially to the lungs. • The pulse oximeter can also measure pulse rate. • The volume of blood being pumped by the heart per minute is called the cardiac output. • The frequency of pumping during one minute is called the pulse rate. These cardiac function indicators can be determined by the pulse oximeter. How does oxygen move around the body? • Oxygen is transported throughout the body by the blood. • Oxygen is inhaled into the lungs, and carbon (carbon dioxide) is exhaled from the lungs to the air. This process is called ventilation. • Inhaled air flows into the upper airway, then into the peripheral airways, and is finally distributed into the lungs. This process is called distribution. • Oxygen is absorbed from the alveoli, then into the lung capillaries via alveolar membranes, while carbon dioxide moves from the lung capillaries to the alveoli. This process is called diffusion. How does oxygen get into the blood? • Only about 0.3 ml of gaseous oxygen dissolves in 100 ml blood per mmHg (pressure). • This amount is only 1/20 of carbon dioxide solubility. This suggests that a human could not get sufficient oxygen if solubility were the only way to get oxygen in the blood. For this reason, hemoglobin (Hb) has an important role as a carrier of oxygen. • One molecule of hemoglobin can bind to 4 molecules of oxygen, and 1 g of hemoglobin can bind to 1.34 ml of oxygen. Since 100 ml of blood contain about 15 g of hemoglobin, the hemoglobin contained in 100 ml of blood can bind to 20.1 ml of oxygen. • Amount of oxygen contained in 100 ml of blood (20.4 ml) = Dissolved oxygen (0.3 ml) + Hb-bound oxygen (20.1 ml) How does oxygen get into the blood? • • • • Oxygen content of arterial blood (CaO2 [mL O2/100 mL]) CaO2 =1.34 mL /g X Hb (g/100Ml) XSaO2 + 0.003 X PaO2 SaO2 =100XO2Hb/(O2Hb + RHb) The arterial oxygen saturation (SaO2) is usually expressed as the ratio of oxygenated hemoglobin (O2Hb) to the total amount of Hb that can bind oxygen. The amount of hemoglobin that can bind oxygen is the sum of O2Hb and deoxygenated (reduced) hemoglobin (RHb). • The SaO2 value for a given PaO2 depends on the position of the oxygen-hemoglobin saturation curve (also called the oxygen-hemoglobin dissociation curve) • At the usual body temperature and pH, a PaO2 of 60 mm Hg corresponds to approximately an SaO2 of 90%. How does oxygen get into the blood? • A left shift results in a lower PaO2 being associated with a given SaO2 and vice versa. • A shift to the left can occur with decreasing temperature, hydrogen ion concentration [H+], PaCO2, or level of 2, 3-diphosphoglycerate (2, 3DPG). What is oxygen saturation? • Hemoglobin bound to oxygen is called oxygenated hemoglobin (HbO2). Hemoglobin not bound to oxygen is called deoxygenated hemoglobin (Hb). • The oxygen saturation is the ratio of the oxygenated hemoglobin to the hemoglobin in the blood, as defined by the following equation. What is oxygen saturation? • Since each hemoglobin molecule can bind to 4 molecules of oxygen, it may bind with 1 to 4 molecules of oxygen. However, hemoglobin is stable only when bound to 4 molecules of oxygen or when not bound to any oxygen. It is very unstable when bound to 1 to 3 molecules of oxygen. • Hemoglobin exists in the body in the form of deoxygenated hemoglobin (Hb) with no oxygen bound, or as oxygenated hemoglobin with 4 molecules of oxygen. • Oxygen saturation can be assessed by SaO2 or SpO2. • SaO2 is oxygen saturation of arterial blood, while SpO2 is oxygen saturation as detected by the pulse oximeter. They are called arterial blood oxygen saturation and percutaneous oxygen saturation, respectively. How does the pulse oximeter measure oxgen saturation ? • Hemoglobin bound to oxygen is called oxygenated hemoglobin and has a bright red color. • Hemoglobin with no oxygen bound to it is called deoxgenated hemoglobin and has a dark red color. That is why arterial blood has bright red color and venous blood has dark red color . • The pulse oximeter probe containing light-emitting diodes (LEDs) and a photoreceptor situated opposite, is placed across tissue, usually a finger or earlobe. • Some of the light is transmitted through the tissues while some is absorbed.The ratio of transmitted to absorbed light is used to generate the peripheral arterial oxygen saturation (SpO2) displayed as a digital reading, waveform, or both. How does the pulse oximeter measure oxgen saturation ? • As a result of rapid sampling of the light signal, the displayed reading will alter every 0.5 - 1 s, displaying the average SpO2 over the preceding 5 - 10 s. • Most pulse oximeters are accurate to within +/- 2% above an SaO2 of 90%. • Tissue thickness should be optimally between 5 - 10 mm. • Poor readings may be improved by trying different sites , warming sites or applying local vasodilators. • Information about pulse rate and waveform (plethysmographic waveform) may also be provided. • A poor signal may indicate a low blood pressure or poor tissue perfusion - reassess the patient. The graph shows spectroscopic and absorptive properties (properties regarding which color is absorbed) of oxygenated hemoglobin (HbO2) and deoxygenated hemoglobin (Hb) Oxygenated hemoglobin absorb more infra red while deoxygenated hemoglobin absorb more red How does the pulse oximeter measure oxgen saturation ? • The percentage of oxygenated hemoglobin and deoxygenated hemoglobin is determined by measuring the ratio of infrared and red light detected by the pulse oximeter. • The pulse oximeter emits red (R) and infrared (IR) LED light that passes through the body, receives data from a photodetector, and calculates the oxygen saturation by determining the ratio of the two waveforms. How does the pulse oximeter measure oxgen saturation ? • When the amount of HbO2 is greater, the absorption of red light becomes smaller and the absorption of infrared light becomes larger, resulting in a lower ratio of absorption of the two wavelengths. • In contrast, when the amount of deoxygenated hemoglobin is greater, the absorption of red light becomes greater while the absorption of infrared light becomes smaller, resulting in an increased ratio of absorption of the two wavelengths. Thus, the pulse oximeter determines oxygen saturation by measuring the ratio of oxygenated hemoglobin to deoxygenated hemoglobin. How can the pulse oximeter measure oxygen saturation, even though the light from the pulse oximeter has to pass through layers of tissue before it reaches the blood? • Arterial blood pumped from the heart moves through vessels in the form of waves called pulse waves resulting in a change in size of the artery . However, venous blood does not move in pulse waves. • The light emitted into the body is absorbed by arterial and venous blood as well as other tissue, and some continues through the body. However, tissues other than arteries experience no change in size over time. The following figure shows temporal change in pulse wave signals. How does the pulse oximeter measure oxgen saturation ? • Since tissues other than arterial blood experience no change in size over time, the light passing though the body changes in intensity over time depending on the change in the size of arterial blood layers due to pulse waves. The change in intensity results from the change in size of the arterial blood layer, uninfluenced by venous blood and other tissues. • Monitoring changes in the components of the exiting light provides data on arterial blood. • Measuring the cycle of the changes in light components also reveals the pulse rate. • The pulse oximeter can measure oxygen saturation as well as pulse rate based on the pulsing of arterial blood. What factors cause errors in the pulse oximeter? 1. Abnormal hemoglobin :Blood may contain abnormal hemoglobins such as carboxyhemoglobin and methemoglobin which do not contribute to oxygen delivery. The dual-wavelength pulse oximeter may be affected by these abnormal hemoglobins. 2. Medical dyes :If dyes such as cardio green, intravascular dyes, and indocyanine green have been injected into the blood, they may influence the level of transmission of the red and infrared light. 3. Manicure and pedicure : If users wear nail polish, it may absorb the light emitted from the LED, and change the light transmitted though the body, influencing the values calculated. What factors cause errors in the pulse oximeter? 4. Major body motion :Body motion may cause noise that affects the values calculated. When noise, including that caused by body motion, reduces the reliability of the values calculated, the pulse oximeter will display a warning. 5. Blood flow blocked due to pressure on arms or fingers :The pulse oximeter measures oxygen saturation based on changes in the blood flow. Therefore, if the blood flow is blocked, correct measurement becomes impossible. In addition, if the fingers are flexed at a uniform pace (if, for example, grip strength is intensified at a uniform pace on an ergometer), the pulse oximeter may interpret the pressure as changes in pulse rate, causing errors (particularly pulse rate errors) What factors cause errors in the pulse oximeter? 6. Peripheral circulatory failures :The pulse oximeter utilizes blood flow to monitor changes in the amount of light transmitted to calculate values. If the peripheral blood flow is reduced, adequate data may not be obtained, and the result is inaccurate measurement. In this case, it is necessary to promote blood flow by massaging or warming the fingers or measuring other fingers with more regular blood flow. 7. Excessive ambient light (panel lamp, fluorescent lamp, infrared heating lamp, direct sunlight, etc.) The pulse oximeter can usually cancel out the effects of ambient light. However, if the ambient light is too strong, the device will not be able to cancel out the effects, and this may cause errors What factors cause errors in the pulse oximeter? 8. Ambient electromagnetic waves : If electric appliances such as televisions, mobile telephones, or medical devices which produce high levels of electromagnetic waves are used near the pulse oximeter, the electromagnetic waves from these devices may interfere with accurate measurement. 9. Probe attached incorrectly ; If the probe is not properly attached, it may detect a variety of noise, resulting in inaccurate measurement. When in doubt, the technologist can place the probe on her or his own finger as a test of oximeter accuracy. Why an ABG instead of Pulse oximetry? • Pulse oximetry is non-invasive and provides immediate and continuous data. • Pulse oximetry does not assess ventilation (pCO2) or acid base status. • Pulse oximetry becomes unreliable when saturations fall below 70-80%. • Technical sources of error (ambient or fluorescent light, hypoperfusion, nail polish, skin pigmentation) • Pulse oximetry cannot interpret methemoglobin or carboxyhemoglobin Why an ABG instead of Pulse oximetry? • Pulse oximetry provides only a measure of oxygen saturation, not content, and thus gives no indication of actual tissue oxygenation. • Readings from a pulse oximeter must not be used in isolation: it is vital to interpret them in light of the clinical picture and alongside other investigations, and potential sources of error. Pulse oximeters are not affected by: • Anaemia (reduced haemoglobin) • Jaundice (hyperbilirubinaemia) • Skin pigmentation Does the ratio of PaO2 to SpO2 always remain the same? • The amount of oxygen dissolved in the blood is proportional to the partial pressure of oxygen. • The amount of oxygen bound to hemoglobin will increase as the partial pressure of oxygen increases. • The amount of oxygen bound to hemoglobin does not increase in proportion to the partial pressure of oxygen. The increase may be indicated by an S-shaped curve.This is called the oxygen dissociation curve. In the following graph, the low pH curve shows that when PaO2 is 80 mmHg (Torr), oxygen saturation is 80%. Does the ratio of PaO2 to SpO2 always remain the same? • The sinusoid shape of the curve means that an initial decrease from a normal PaO2 is not accompanied by a drop of similar magnitude in the oxygen saturation of the blood,and early hypoxaemia may be masked. • At the point where the SpO2 reaches 90-92%, the PaO2 will have decreased to around 60 mmHg. In other words, the PaO2 will have decreased by almost 50% despite a reduction in oxygen saturation of only 6-8%. • The output from a pulse oximeter relies on a comparison between current signal output and standardised reference data derived from healthy volunteers. • Readings provided are increasingly unreliable with increasing hypoxaemia. Below 70% the displayed values are highly unreliable. Does the ratio of PaO2 to SpO2 always remain the same? • Because of the normal position on the flat portion of the O2Hb dissociation curve, there is little change in the SaO2 as a result of the fall in PO2 associated with sleep. • If the baseline awake PaO2 is lower, the fall in SaO2 will be greater for the same drop in PaO2. In patients with lung disease and a lower awake PO2, even a normal sleep-related drop in PO2 will be associated with a larger decrease in the SaO2. • The change in ventilation with sleep is due to a fall in VT with minimal change in the RR. Does the ratio of PaO2 to SpO2 always remain the same? • The position of the O2Hb dissociation curve is often defined by the P50, which is the PaO2 corresponding to an SaO2 of 50%. • For Hb A, the P50 is 26 mm Hg but is 42 to 56 mm Hg in sickle cell disease patients. The net effect is a rightward shift in the O2Hb dissociation curve for HbS. This means that for a given SaO2, the PaO2 is higher in SCD patients than would be expected based on the normal O2Hb dissociation curve. Does the ratio of PaO2 to SpO2 always remain the same? • The oxygen dissociation curve is called the “standard oxygen dissociation curve” in which the body temperature is 37°C, pH 7.4. • The curve may shift to the right or left, depending on patient conditions. • If the body temperature decreases and pH increases, the curve will shift to the left. If the temperature increases and pH decreases, the curve will shift to the right. Does the ratio of PaO2 to SpO2 always remain the same? • Determining the oxygen-carrying capacity of Hb is complicated by the fact that both carboxyhemoglobin (COHb) and met-hemoglobin (MetHb) are forms of circulating Hb that do not bind oxygen. • Carboxyhemoglobin occurs when carbon monoxide (CO) binds to Hb. Smokers have increased carboxyhemoglobin. • MetHb occurs when the normal ferrous state (Fe2+) of the iron moiety in Hb is oxidized to the ferric stage (Fe3+). Significant methemoglobinemia can occur after exposure to certain medications. Does the ratio of PaO2 to SpO2 always remain the same? • The sum of the fractional concentrations of O2Hb, RHb, COHb, and MetHb equal 100%. • FO2Hb + FRHb + FCOHb + FMetHb = 100% or • FO2Hb = O2Hb X 100 /(O2Hb+RHb +COHb + MetHb) Does the ratio of PaO2 to SpO2 always remain the same? • The four fractions of Hb can be accurately measured by co-oximeters that measure the absorption of 4 or more wavelengths of electromagnetic radiation by blood . This is possible because the four forms of Hb differ in their absorption for the different wavelengths of radiation. • Pulse oximetry uses only two wavelengths: 660 nm (red) and 940 nm (infrared) to measure the O2Hb and RHb . • The absorption of radiation at 660 nm is much greater with RHb than O2Hb, whereas O2Hb absorbs more radiation at 940 nm. • COHb has about the same absorbance at 660 as O2Hb and, if present, increases the measured SpO2 value . Does the ratio of PaO2 to SpO2 always remain the same? • In normal individuals, FCOHb is 2% or less but can be 8% or more in cigarette smokers. • Patients with SCD often have FCOHb values of 4% or more due to production of CO from chronic hemolysis. • In patients who are heavy smokers, it is important to remember that the SpO2 may overestimate the FO2Hb. Does the ratio of PaO2 to SpO2 always remain the same? • If a patient has a lower than expected SpO2 while awake, a number of possibilities should be considered including a faulty oximetry probe, poor signal quality due to poor perfusion, a shift in the O2Hb saturation curve or an abnormal Hb. • If oximetry issues are ruled out, an arterial blood gas is needed to determine whether hypoxemia is really present . In this situation, co-oximetry analysis could also determine whether significant COHb or MetHb is present and determine a true SaO2 and the fraction of Hb that is oxygenated. • If clinically indicated, analysis with a co-oximeter will provide more accurate information. Concerning mmHg and Torr • Standard atmospheric pressure is 760 mmHg. This means atmospheric pressure is the same as that exerted by a 760 mm high column of mercury (Hg). • The first measurement of atmospheric pressure was performed by Torricelli, a student of Galileo Galilei. One mmHg is referred to by the term “Torr” after his name. • The unit “mmHg” is the same as “Torr,” and one atmospheric pressure is 760 mmHg = 760 Torr. • Currently, Torr is generally used when measuring PaO2. Does the ratio of PaO2 to SpO2 always remain the same? • SpO2 is accurate down to about 70%. Whereas values below 70% are often reported, one must keep in mind that they probably do not correspond accurately to the actual SaO2. • In the case of COHb, the absorption of 660 nm is similar to O2Hb and causes a falsely elevated SpO2 estimate of the FO2Hb. It is estimated that for every 1% of circulating COHb, the pulse oximeter reading is falsely elevated by about 1% compared with the FO2Hb. Does the ratio of PaO2 to SpO2 always remain the same? • MetHb absorbs nearly equal amounts of red and near infrared light, giving an R = 1. As the concentration of MetHb increases, the pulse oximeter reads closer and closer to 85%. Therefore, methemoglobinemia may cause the SpO2 to give a falsely low estimate of the SaO2 and, hence, the PaO2. On the other hand methemoglobin shifts the oxyhemoglobin saturation curve to the left and the SaO2 is less than the FO2Hb as oxygen does not bind methemoglobin . Methemoglobinemia can occur from medications (e.g., benzocaine, sulfonamides) Factors that impair the accuracy of SpO2 • In sleep monitoring, an arterial oxygen desaturation is usually defined as a decrease in the SpO2 of 3% or 4% or more from baseline. • Note that the nadir in SaO2 commonly follows apnea (hypopnea) termination by approximately 6 to 8 seconds (longer in severe desaturations). This delay is secondary to circulation time and instrumental delay (the oximeter averages over several cycles before producing a reading). Apneas are followed by arterial oxygen desaturations. Longer apneas are associated with more severe desaturation. SpO2 = pulse oximetry. Handheld Pulse Oximeter Fingertip pulse oximeter Portable pulse oximeter Factors that impair the accuracy of SpO2. • Oximeters may vary considerably in the number of desaturations they detect and their ability to discard movement artifact. • Using long averaging times may dramatically decrease the detection of desaturations. The ability of oximeters to detect desaturations is especially important in light of the definitions of hypopnea that depend on an associated desaturation. • The AASM scoring manual recommends a maximum averaging time of 3 seconds at a heart rate of 80 bpm. In patients with a slow heart rate, a slightly longer averaging time (at least a 3-beat average) may be needed. A long averaging time impairs the ability of oximetry to detect arterial oxygen desaturation. SpO2 = pulse oximetry. Uses Pulse oximetry has four main uses: 1. detection of /screening for hypoxaemia; (SPo2 < 92%-94% should be referred to ABG to assess elegibilty for LTOT). 2. targeting oxygen therapy; 3. routine monitoring during anaesthesia; 4. diagnostic (e.g. sleep hypnoea). Targeted oxygen therapy in critically ill patients • In critically ill patients, the target of oxygen therapy is SpO2 94-98% in non hypercapnic patients and 88-92 % in hypercapnic patients . Guidelines for long term use of oxygen • Referral for assessment for long-term oxygen therapy is considered if SPo2 <92 - 94% (need ABG ) • Patients potentially requiring LTOT should not be assessed using pulse oximetry alone • Each applicant's condition must be stabilized and treatment regimen optimized before long-term oxygen therapy is considered. Optimum treatment includes smoking cessation. • Applicants must have chronic hypoxemia on room air at rest (Pa02 of 55 mmHg or less, or Sa02 of 88% or less). Guidelines for long term use of oxygen • Applicants with persistent Pa02 in the range of 56 to 60 mmHg may be considered candidates for long-term oxygen therapy if any of the following medical conditions are present: cor pulmonale ; pulmonary hypertension; peripheral oedema or persistent erythrocytosis (Haematocrit >55%). • Persistent Pa02 in the range of 56 to 60mmHg may be candidates for long-term oxygen therapy if the following occurs: Exercise limited hypoxemia ; documented to improve with supplemental oxygen ; Nocturnal hypoxemia. • LTOT should be for minimum 15 hours per day .and up to 24 hours per day may be of additional benefits. Guidelines for long term use of oxygen • Type I: low PaO2 (< 60 mm Hg), normal PaCO2 (< 6 - 7 kPa).In these patients it is safe to give a high concentration of oxygen initially with the aim of returning their PaO2 to normal and then once clinically stable, adjusting the inspired oxygen concentration to maintain an SpO2 of 94 - 98%. • Type II: low PaO2 (< 60 mm Hg), increased PaCO2 (> 6 - 7 kPa). This is often described as hypercapnic respiratory failure and is usually caused by COPD. If given excessive oxygen, these patients may develop worsening respiratory failure with further increases in PaCO2 and the development of a respiratory acidosis. If unchecked, this will eventually lead to unconsciousness, and respiratory and cardiac arrest. The target oxygen saturation in this at risk population should be 88 - 92%.