Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Urinary tract infection wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Sarcocystis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Hepatitis C wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
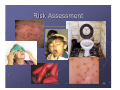
Common cold wikipedia , lookup
Marburg virus disease wikipedia , lookup
Hepatitis B wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
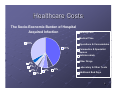
Routine Practices Protecting You Protecting the Patient Protecting the Public Infection Prevention & Control The Mission Protect the Patient Protect the Worker Protect the Public From exposure to disease causing organisms. It’s everybody's responsibility! 2 Impact of Hospital Acquired Infections on the Patient & Family “At any one time approximately 1 in 10 patients in acute care hospitals have a hospital-acquired infection (HAI)” Economic - lost productivity Additional 5 days of lost work Social - disruption of family life Twice the time spent doing post-hospital care at home Personal - pain, suffering, loss function → life Additional 6 to 13 days returning to normal ADL’s In the UK, 13% of patients with HAI died compared with 2% of patients who did not present with an HAI in hospital 3 Healthcare Costs The Socio-Economic Burden of Hospital Acquired Infection Nursing Care Medical Time 33% Operations & Consumables 41% Paramedics & Specialist Nurses Antimicrobials Other Drugs 4% 4% 2% Laboratory & Other Tests 4% 6% 6% Additional Bed Days 4 Communicable Infections of Concern Skin & soft tissue → S.aureus → GAS 5 Communicable Infections of Concern Gastrointestinal → Noroviruses → C.difficile → E.coli 0157:H7 → Campylobacter → Rotavirus 6 Communicable Infections of Concern Respiratory → RSV → Influenza → Pertussis → TB → MRSA pneumonia 7 Troubling Clinical Issues Antibiotic Resistant Organisms (AROs) Virulence factors disable cell mediated defenses Serious and invasive infections Limited antibiotic choices C.difficile Toxin producing > tissue damage Pressured by antibiotics Added morbidity > extends hospital stay 8 Troubling Environmental Issues Environmental contamination is greatest in the presence of infection or incontinence 1. 2. 3. 4. 5. 6. Overcrowding & clutter Insufficient dedicated toileting facilities Inadequate cleaning & housekeeping measures Inconsistent application of appropriate precautions Staffing levels Patient compliance with Infection Control measures 9 Who’s Got What – Can You Tell? 10 Routine Practices Routine Practices are to be applied at all times, by all staff, regardless of the patient's presumed infection status. 11 Routine Practices also known as Standard Precautions are more encompassing then previous Bloodborne Pathogen Precautions or Universal Precautions based on the assumption that all blood and certain body fluids (urine, feces, wound drainage, sputum) contain organisms (bacteria, virus, or fungus) Routine Practices reduce exposure (both volume and frequency) of blood/body fluid to the health care provider 12 What are Routine Practices? Risk Assessment Risk Reduction Education 13 Risk Assessment 14 Risk Assessment •Fever/Cough with or without a rash? •Skin/Soft tissue infection? •Diarrhea illness, NYD? (with or without vomiting) 15 Risk Assessment No risk of Infectious Disease? Continue Routine Practices Risk of Infectious Disease? Continue Routine Practices and add Additional Precautions 16 Risk Reduction 1. Hand Hygiene and Respiratory/Cough Etiquette 2. Use of Personal Protective Equipment (gloves, gown, mask) when/where appropriate 3. Placement of patients 4. Cleaning and disinfection of equipment and care items 5. Healthy workplace practices (e.g. immunization) 6. Handling of sharps and laundry 7. Management of waste (e.g. biohazard waste disposal) 17 Hand Hygiene Method Social Solution Alcohol based hand rub Task For Routine Practices or Hygienic hand disinfection Soap and Water (if visibly soiled and/or contact with spores) An alcohol based hand rub or Soap and Water (if visibly soiled and/or following contact with spores) followed by alcohol based hand rub Aseptic (Surgical scrub) A 2 minute antiseptic wash (i.e. chlorhexidine (CHG 4%)) and dry on sterile towels In high risk areas (e.g. when Additional Precautions are implemented) and during outbreaks as directed by Infection Prevention and Control Prior to surgical and other invasive procedures 18 Cough/Respiratory Etiquette 19 Personal Protective Equipment 20 Contamination Rates Pathogen Contamination rate(s) of health care workers’ hands (%) Duration of persistence on hands Duration of persistence on inanimate surfaces C. Difficile 14-59 unknown 1 day (vegetative cells) to 5 months (spores) E. Coli unknown 6-90 minutes 2 hours to 16 months MRSA up to 16.9 unknown 1 month to 7 months Rhinovirus up to 65 unknown 2 hours to 7 days VRE up to 41 up to 60 minutes 5 days to 4 months “Yeasts” including Candida spp. 23-81 1 hour 1 day to 5 months Extract from Kampf, G., Kramer, A., Epidemiologic Background of Hand 21and Rubs, Hygiene and Evaluation of the Most Important Agents of Scrubs Clinical Microbiology Reviews, Oct 2004, pg. 865. Education Understand and demonstrate work practices that reduce the risk of infection hand hygiene proper use of personal protective equipment be immunized do not come to work with a communicable disease 22 Education Educate patients/residents/families about hygiene and infection prevention and control strategies (ie. Hand Hygiene) 23 Precautions 24 Precautions Additional Precautions are required for interventions sustained over a period of time, such as: Diseases either suspected or confirmed during their infectious state Situations in which extensive contamination of the patient’s environment is expected (e.g. an incontinent patient with diarrhea which can’t be contained within a diaper) Patients infected or colonized with epidemiological important organisms (e.g. MRSA, VRE) 25 26 Contact Precautions Micro-organism large & bound to skin or body substances Transmission • Transferred through direct contact with colonized or infected host tissue/secretions OR indirectly from a contaminated fomite • Transmission is completed when the care provider transfers the organism from the fomite to their hands and then to another host or another host has skin contact with the contaminated fomite 27 Contact Precautions Prevention • Gown & gloves for all direct care contact • Hand hygiene • Dedicated toilet & dedicate or disinfect care assessment equipment • Segregation or cohort • Housekeeping (bleach with C.diff) 28 29 Droplet Precautions Micro-organism > 5 microns in size Transmission • Transferred by aerosol of respiratory secretions, emesis or diarrhea through forceful expulsion of these • Distance traveled about 2 meters • Acquisition through fecal oral route by contact transmission or through the respiratory route 30 Norovirus The Norovirus is transmitted primarily through the fecal-oral route However, aerosolized vomit has also been impacted as a mode of norovirus transmission 31 Droplet Precautions Prevention • • • • Surgical mask – Patient & HCW Hand hygiene Segregation of 1 to 2 metres Gown & gloves 32 33 Airborne Precautions Micro-organism is < 5 microns in size • Expelled from the respiratory tract by cough, sneeze or laugh Transmission • Transferred to another host as the particles drift through the air • Acquisition through the respiratory route Prevention • Negative air isolation/N95 mask 34 Organize your work 35 Summary 1. Always use Routine Practices 2. Apply appropriate Precautions as required 3. Consult your Infection Control Manual if any questions 4. Learn your Infection Control Practitioner’s name and number and call if you have any questions 36 FORMS and MORE FORMS! ARO Admission 37 ARO screening Identifies at risk populations (NOTE: now req’d for every patient on entry to a LTC facility on VI) Supports continued infection control measures Informs clinical decisions when infection is 250 present 200 150 CA-MRSA HA-MRSA Total 100 50 0 2002-2003 2003-2004 2004-2005 2005-2006 38 ARO Screening A N T IB IO T IC R E S IS T A N T O R G A N IS M S [A R O s ] S c r e e n in g Q u e s t io n n a ire fo r A d m is s io n s F o r S a fe ty 1 st H o s p ita ls a d d re ss o g ra p h Is th e A R O A le rt s h o w in g o n A d m is s io n F o rm ? Yes No A . S c re e n in g Q u e s tio n s Yes P le a s e a s k th e fo llo w in g S c r e e n in g Q u e s tio n s : 1. H a v e yo u b e e n a d m itte d to h o s p ita l fo r 2 d a ys o r m o re (> 4 8 h o u rs ) in th e p a s t ye a r? T h is in c lu d e s tra n s fe rs b e tw e e n h o s p ita ls & re a d m is s io n s . 2. H a v e yo u re c e iv e d d ia lys is o r c h e m o th e ra p y in th e p a s t ye a r? 3. H a v e yo u o r a m e m b e r o f yo u r h o u s e h o ld h a d a s k in in fe c tio n in th e p a s t ye a r th a t w a s d iffic u lt to tre a t? E x a m p le : a b s c e s s o r b o il. 4. H a v e yo u o r a m e m b e r o f yo u r h o u s e h o ld b e e n fo u n d to h a v e b a c te ria re s is ta n t to a n tib io tic s , lik e M R S A /V R E ? C irc le if k n o w n . 5. H a v e yo u u s e d s tre e t d ru g s o th e r th a n m a riju a n a w ith in th e p a s t 5 ye a rs ? 6. H a v e yo u s p e n t tim e in a c o rre c tio n s fa c ility w ith in th e p a s t ye a r? 7. D o yo u liv e o n th e s tre e t (h a v e n o fix e d h o m e a d d re s s )? If Q u e s tio n n a ire n o t c o m p le te d , s ta te re a s o n & p ro c e e d to S e c tio n “ B ” : P a tie n t u n c o o p e ra tiv e /r e fu s e d P a tie n t c o g n itiv e ly im p a ire d /u n c o n s c io u s S ig n a tu re : U n it: No O th e r _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ D a te : T im e : B . A c tio n s IF If a n s w e rs to a ll 7 q u e s tio n s a b o v e is N O a n d th e re is N O A R O A le rt o n A d m is s io n F o rm → • If a n s w e r to a n y q u e s tio n a b o v e is Y E S o r if A R O A le rt is p re s e n t o n A d m is s io n F o rm → • If u n a b le to c o m p le te S c re e n in g Q u e s tio n n a ire → THEN N o L a b S p e c im e n s re q u ire d . st Im p le m e n t ro u tin e p re c a u tio n s (re fe r to S a fe ty 1 ). • • • C o lle c t a p p ro p ria te L a b S p e c im e n s st A s s e s s fo r in fe c tio n (re fe r to S a fe ty 1 ) Im p le m e n t a p p ro p ria te p re c a u tio n s → o b ta in L a b S p e c im e n s C . L a b S p e c im e n C o lle c tio n (S e p a ra te s w a b fo r e a c h A R O ) M R S A : If “ye s ” to a n y A R O s c re e n q u e s tio n o r u n a b le to c o m p le te q u e s tio n n a ire o r A R O a le rt fo r M R S A p re s e n t C o lle c t s e p a r a te s w a b fro m e a c h s ite : N a re s R e c tu m U n h e a le d o r d ra in in g w o u n d o r a b s c e s s S to m a , in c lu d in g tra c h e o s to m y, s u p ra p u b ic c a th e te r a n d P E G tu b e s ite s U rin e if c a th e te r in p la c e D e v ic e in s e rtio n s ite if IN F L A M E D a ls o c o lle c t s p u tu m (if p ro d u c tiv e c o u g h ) If “ye s ” to q u e s tio n s # 2 o r # 4 o r A R O a le rt fo r V R E p re s e n t VRE: R e c tu m a n d O s to m y (if p re s e n t) C o lle c t: S w a b fro m E S B L : If th e re is a re c o rd o f c lin ic a l in fe c tio n w ith a n E S B L o r A R O a le rt fo r E S B L p re s e n t U rin e s p e c im e n a n d s w a b fro m R e c tu m a n d D ra in in g w o u n d (if p re s e n t) C o lle c t: C O L L E C T IO N M E T H O D F O R S W A B S A B O V E 1. 2. 3. M o is te n tip o f c u ltu re s w a b w ith c u ltu re m e d iu m . U s e firm c irc u la r/tw is tin g m o tio n . F o r n a re s , b ris k ly ru b th e m u c o u s m e m b ra n e s (b o th s id e s ) w ith o n e s w a b . S ig n a tu re : U n it: D a te : T im e : 39